CONTRE Irradiation axillaire, CMI, sus-sous claviculaire - Joseph Gligorov
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous

Irradiation axillaire, CMI,
sus-sous claviculaire
CONTRE
Joseph Gligorov
Remerciements à Y Belkacemi
Control locorégional et gravité de la maladie
Envahissement ganglionnaire et rechute Ø Etude rétrospective Ø n = 9616 FUP médian : 11 ans Evts pN0 pNmic pNmacro p RL 6.1% 6.8% 8.7%
Facteurs de risque de rechute locorégionale
après mastetomie et pN0
• LRR according to the number of prognostic factors
Studies N of prognostic factors Factors
0 1 2 3
Rowell 5% 10% 15-20% 25-50% Age, menop
pT, LVI
Grade, margins
Jagsi 1.2% 10% 17.9% 40,6% Menop
pT
LVI
margins
Abi-Raad 2% 3,3% 5,8% 19,7% Age, menop
pT , LVI
margins
Rowell, Radiother Oncol 2009; Abi-Raad, IJROBP 2011; Jagsi, IJROBP 2005
Facteurs de risque de rechute
locorégionale et indication de RT de paroi
après mastectomie
CT =Mukesh,
AC Radiother
or AC/TOncol 2014
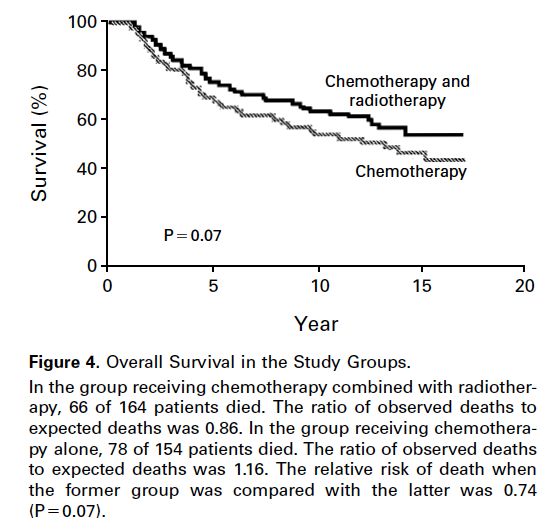
Impact de la RT ganglionnaire dans les essais historiques
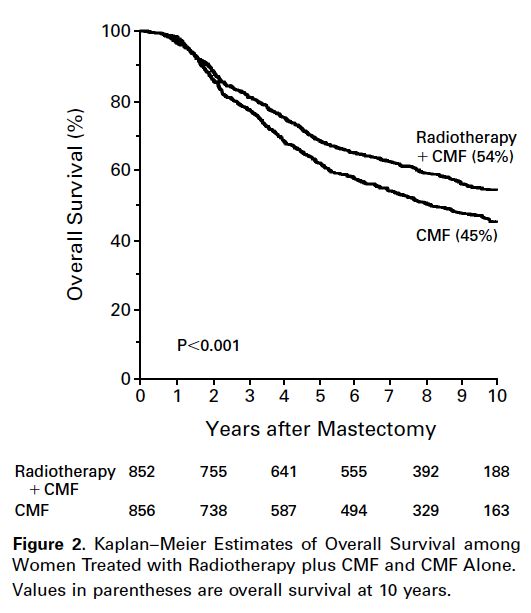
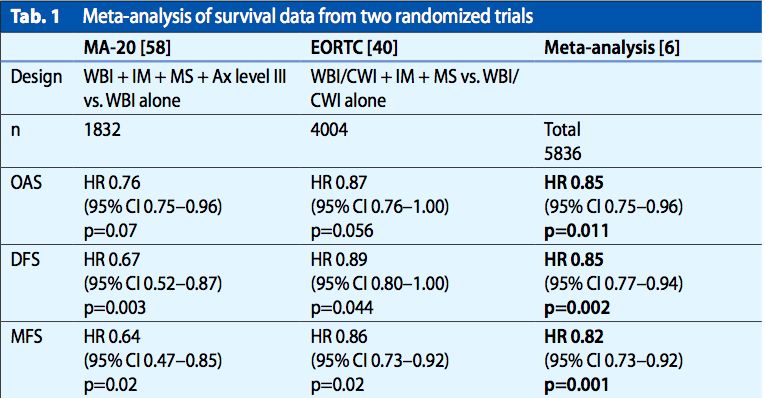
Les essais de RT ganglionnaire OS Whelan et al. Poortmans et al. Budach W et al.
Les essais de RT ganglionnaire
à l’aire du GS
Essais MA20 (RNI : 916) EORTC 22922
pN1 90% (85% 1-3N+ & 5% > 4N+ )
pN1 56% (43% 1-3N+ & 13% > 4N+)
Critères d’inclusion pN0 10%
pN0 44% (1/3 de CT)
T>2cm + 1 facteur : GIII, RH-, Emboles
Volume SCL + CMI
SCL + CMI (3ème EIC)
3ème EIC sauf pour les Qinf 5ème EIC
Rechutes régionales 63% Axillaires N = 54
27% SCL 27 Axillaires; 30 SCL & 4 CMI
Application des résultats à 39% de GS 7% de GS
l’ère du GS? 2/3 des CA avec > 10N
Impact sur la SSM Oui OuiImpact de la RT ganglionnaire dans les essais actuels
Radiothérapie dans les essais du GS
Trial ACOSOG Z0011 IBCSG 23-01 NSABP B32
Number of patients
891 (target =1900) 934 (target =1960) 5600
randomized
Eligibility criteria Micro and
Micro and macrometastases
SLN involvement Only micrometastases macrometastases
Patients with matted nodes, gross
extranodal and >3 SLNs should be
excluded
Median follow-up
6.3 5 8
(years)
Micrometastasis in both 15% of micro after
41% (301/731) 98% (909/930)
SLN and ALND review
% of adjuvant
radiotherapy in both 100% 98% 82%
arms
Whole breast irradiation using PBI (ELIOT) alone: 19%
TgF (1/3 of pts: 228/604)
Type and volumes of No RT parameters
Analyses of axilla coverage: 23% ELIOT as a boost: 9%
RT reported
Axillary field (+TgF): 43 cases
No individual data No individual dataLa radiothérapie de l’aisselle
Criteria ACOSOG Z0011 AMAROS trial
N 891 1425
Randomization SLNB only vs SLNB+ALND ALND vs ALN-RT
Type of surgery BCS (100%) BCS (89%) and TM (11%)
pN status SLNB only SLNB+ALND ALND arm ALN-RT arm
(n=436) (n=420) (n=744) (n=681)
- Isolated tumor cells - - 87 (12%) 67 (10%)
- Micrometastases 164 (44.8%) 137 (37.5%) 215 (29%) 195 (29%)
- Macrometastatses 202 (55.2%) 228 (62.5%) 442 (59%) 419 (61%)
- Unknown 55 70 - -
Radiotherapy WBI using TgF partially covering axillary ALN-RT covered all three levels of the
nodes axilla and the medial part of the
supraclavicular fossa
Outcome endpoints:
- DFS and OS - No difference - No difference
- Lymphoedema - Not assessed - Increased in ALND arm (vs ALN-RT)
Implications for RT consideration in ALND not needed in case of WBI with ALN-RT is an option to ALND
1-2 positive SLN TgF and systemic therapyRéférentiels
NCCN
§ pT1-2 pN0
ü Pas de RT ganglionnaire
ü RT SCL (si T > 5cm , « positive marines »)
§ 1 ou 2 GS +
ü Pas de CA si radiothérapie adjuvante (TgF)
§ 1-3N+
ü RT SCL et CMI
Lyman GH 2014; Gradishar WJ 2016DEGRO
Axillaire
§ 1 ou 2GS micrométastatique (sans CA)
ü Pas de rationnel pour une RT axillaire
§ 1 ou 2GS macrométastatique (sans CA)
ü RT axillaire = alternative au CA
CMI et SCL
ü Tous les N+ et tumeurs des QI et QC
ü pN0 uniquement si T > 5cm
ü CMI non systématique pour les tumeurs des QE
Sautter-Bihl ML 2014 & 2015ESMO 2013
Axillaire
§ Envahissement massif ?
“Short section to RNI indications, recommending that, the
resected part of the axilla should not be irradiated after ALND,
except for specific cases of residual disease after surgery”.
CMI et SCL
ü Indications non abordées spécifiquement
“Until the results from recent trials become available, RNI
remains indicated for only patients with involved LNs”
Senkus E, 2013Belkacemi et al. Ann Oncol 2014
Conclusion
pN0 pNi+ : même risque ganglionnaire
T centrales et internes : RTG au cas par cas
T des QE : bénéfice incertain
Micrométastases (1 ou 2 GS+)
Si CT et RT du sein : pas de RT ganglionnaire
Tangentiels vs maladie résiduelle
Macrométastases (nb de GS prélevés)
CA ou RT axillo-sus claviculaire +/- CMI
RT axillaire selon le ratio N macro/N prélevésMerci
Vous pouvez aussi lire