2018 ESC Guidelines for the management of cardiovascular diseases during pregnancy - Dr R.Sow CHL
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous

2018 ESC Guidelines for the management of cardiovascular diseases during pregnancy Dr R.Sow CHL
• HTA et grossesse • Pathologies thrombo-emboliques et grossesse • Classification mWHO • Pathologies spécifiques
Hypertension artérielle • L’atteinte cardiovasculaire la plus fréquente concernant 5-10% des grossesses dans le monde. • Cause majeure de morbi-mortalité maternelle , fœtale. • Risque maternel : de décollement placentaire, AVC, de défaillance multiviscérale, et de coagulation intravasculaire disséminée
Hypertension artérielle • Risque fœtal : retard de croissance intra-utérin ( 25% des cas de pré éclampsie), mort intra- utérine (4% des cas de pré éclampsie).
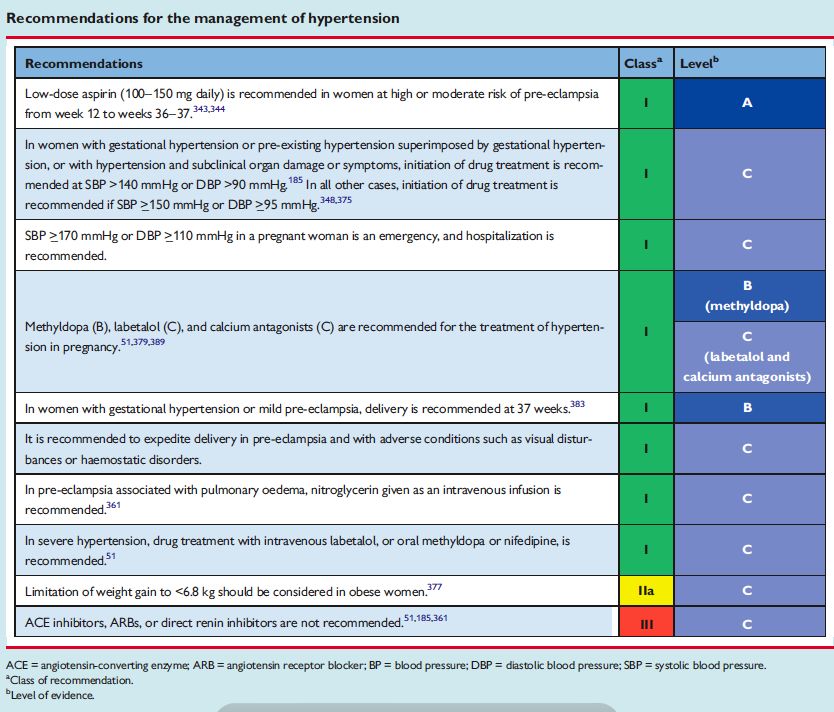
Hypertension artérielle • Définition : SBP >=140 mmHg et/ou DBP90 mmHg. Modérée: 140-159/90-109 mmHg Sévère : >=160/110 mmHg
Hypertension artérielle • Hypertension préexistante : avant 20 SA, persiste >42 jours post-partum et peut être associé à une protéinurie • Hypertension gestationnelle : après 20SA et disparaît dans les 42 jours post-partum • Pré éclampsie : hypertension gestationnelle + protéinurie (>0.3g/24h ou ACR> 30mg/mmol).
Hypertension artérielle • Hypertension pré existante associé à une hypertension gestationnelle avec protéinurie . • Hypertension anténatale inclassable.
Hypertension artérielle • Prise en charge non pharmacologique • Traitement pharmacologique

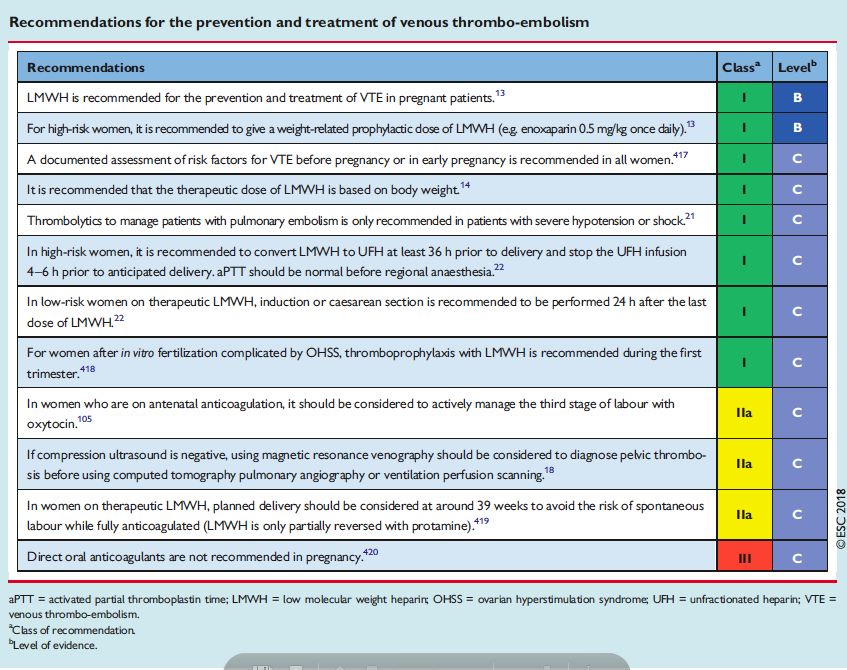
Maladie thrombo-embolique veineuse( TVP et EP) • Représente une cause importante de morbi- mortalité . • Majoration du risque thrombo-embolique de 0.05-0.20% • En Angleterre EP 1ère cause de mortalité maternelle
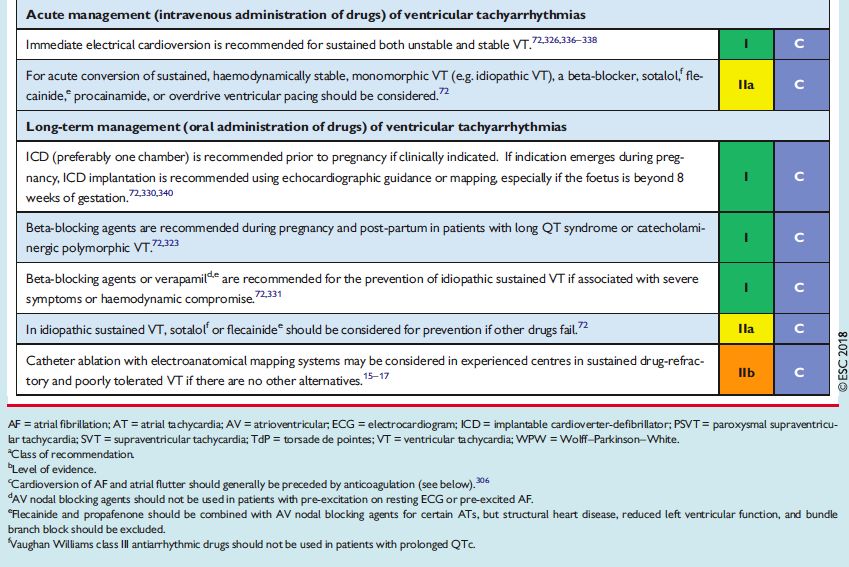
Arythmies
Arythmies
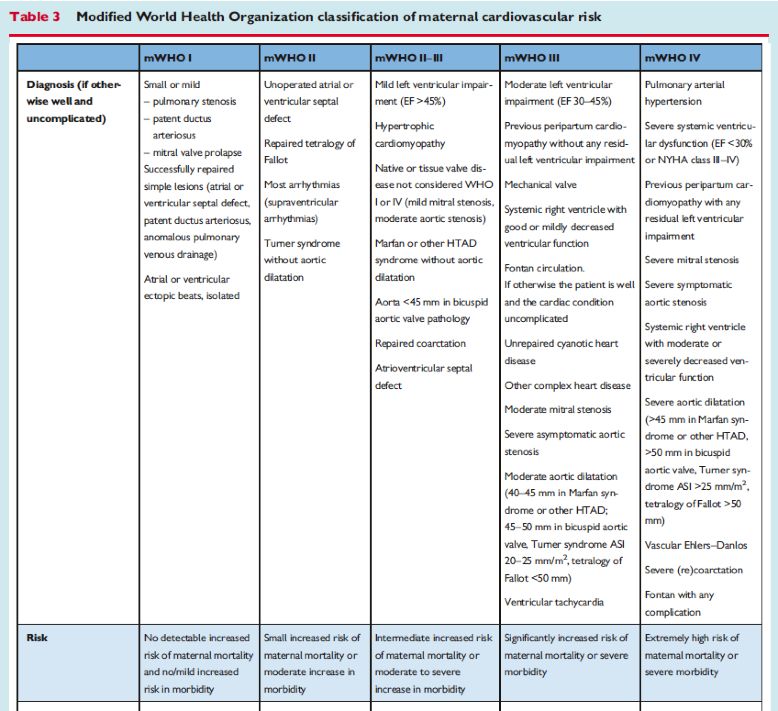
Classification mWHO
Cardiopathies congénitales
Maladie aortique
Maladie aortique
Maladie aortique
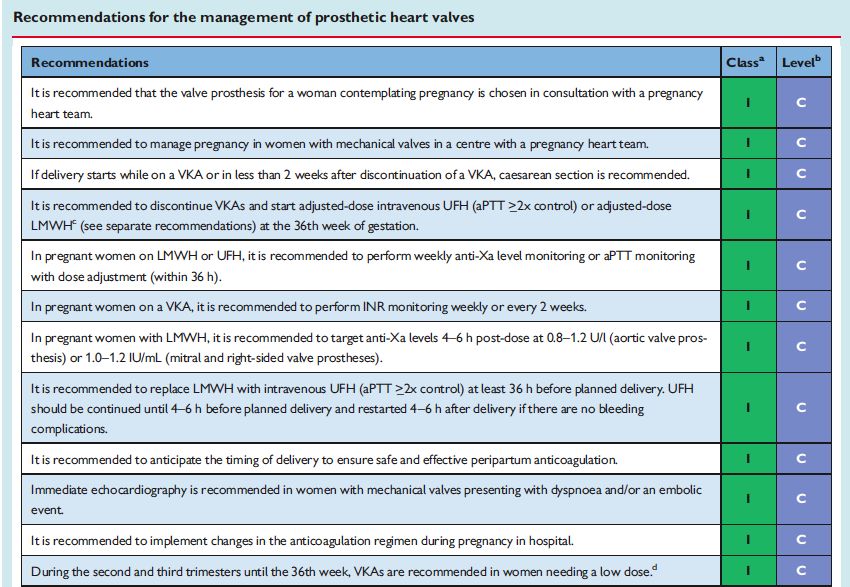
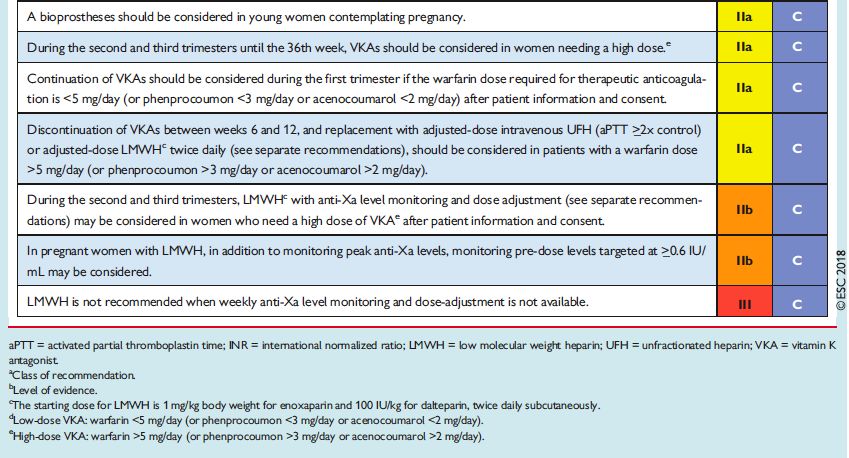
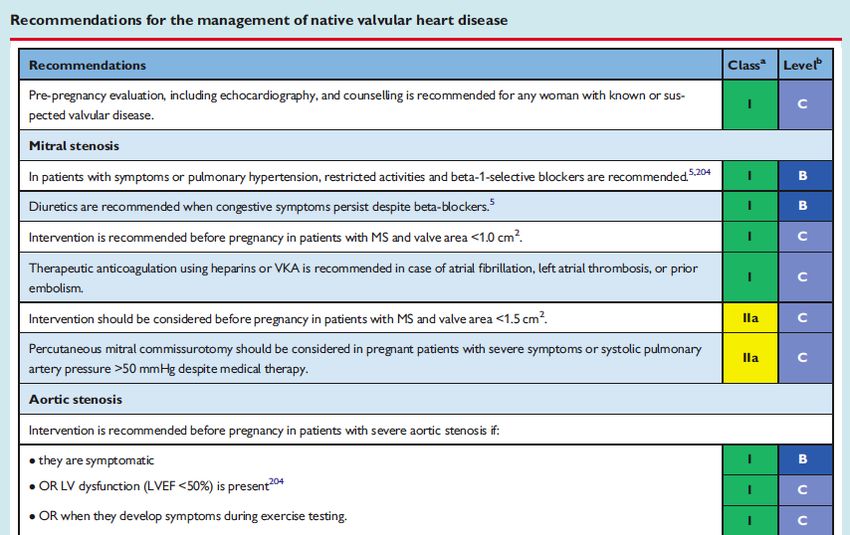
Cardiopathie valvulaire
Cardiopathie valvulaire
Cardiopathie valvulaire
Cardiopathie valvulaire
Cardiopathie ischémique
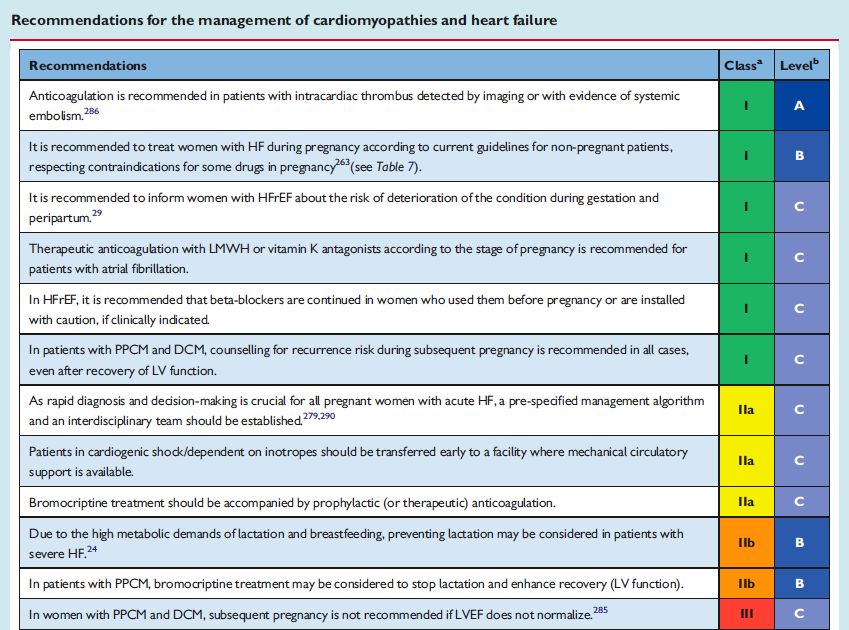
Cardiomyopathie et insuffisance cardiaque
Cardiomyopathie et insuffisance cardiaque
Médicaments et grossesse
Key messages • Risk estimation should be individualized depending on the underlying cardiac diagnosis, ventricular and valvular function, functional class, presence of cyanosis, PAPs, and other factors. • Indications for intervention (surgical or catheter) in the majority of patients do not differ in women who consider pregnancy compared with other patients. There are a few exceptions, such as some degree of aortic dilatation and severe asymptomatic MS.
Key messages • the pregnancy heart team : In women with a moderate or high-risk of complications during pregnancy (mWHO II–III, III, and IV), pre-pregnancy counselling and management during pregnancy and around delivery should be performed in an expert centre by a multidisciplinary team. Management of women with a mechanical valve prosthesis are at high- risk of maternal morbidity (especially valve thrombosis and bleeding) and even mortality.
Key messages • Vaginal delivery is the first choice for the majority of patients. • Indications for caesarean section are: – pre-term labour in patients onOACs – aggressive aortic pathology – acute intratable HF – severe forms of PH (including Eisenmenger’s syndrome)
Key messages • The following patients should be counselled against pregnancy: – with a Fontan operation and additional comorbidities (ventricular dysfunction, arrhythmias, or valve regurgitation) – with PAH – severe systemic ventricular dysfunction (EF
Key messages – with severe aortic dilatation or (history of) aortic dissection – with severe MS (even when asymptomatic) – Patients with severe AS who are symptomatic, or asymptomatic patients with impaired LV function or a pathological exercise test – if LVEF does not normalize in women with previous PPCM.
Key messages • Women with HF during pregnancy should be treated according to current guidelines for non-pregnant patients, respecting contraindications for some drugs in pregnancy (see table ‘Recommendations for drug use in pregnancy’). When inotropes or more advanced treatment is necessary, transport to an expert centre is recommended.
Key messages • In women with PPCM and DCM, subsequent pregnancy is not recommended if LVEF does not normalize. • Patients with congenital LQTS and catecholaminergic polymorphic VT are recommended beta-blockers during pregnancy and post-partum. • Methyldopa, labetalol, and calcium antagonists are recommended for the treatment of hypertension in pregnancy. • LMWH is the agent of choice for VTE prophylaxis and treatment.
Merci de votre attention
Vous pouvez aussi lire