ATELIER " DLPD & DM " COLLOQUE TL-DRMG-RTSMC 20 AVRIL 2018 - JEAN CUSSON MD PHD FRCPC MÉDECINE INTERNE ET PHARMACOLOGIE FMSS-US ET CISSSMC ...
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous
Atelier « DLPD & DM »
Colloque TL-DRMG-RTSMC
20 avril 2018
Jean Cusson MD PhD FRCPC
Médecine interne et Pharmacologie
FMSS-US et CISSSMC
Conflits d’intérêt Support $ au déroulement d’essais cliniques avec des Cie pharmaceutiques commercialisant des Rx pour DM et DLPD entre 1986-1996 puis 2001-2018 Occasionnels honoraires pour conférences et expertises pour des Cies pharmaceutiques Honoraires du GouvQc 1996-2001 comme Président du CCP
motivation, contexte Discordances entre diverses lignes directrices Situations où pt ne correspond pas aux LD Pression grandissante pour appliquer des lignes directrices et donc un malaise pour ne pas les appliquer Mon constat que la non-atteinte de cibles est en lien avec une autogestion de santé déficiente et que possiblement il faut y mettre plus d’efforts en inter- disciplinarité
DLPD C’est facile d’intervenir pour un cas de maladie cardiovasculaire existante Pas mal moins facile de gérer la prévention primaire
Diabète type 2 Un déferlement de résultats depuis qq années L’abondance de variétés de situations cliniques menant à un contrôle sous-optimal et où on doit possiblement modifier l’approche L’absence de LD récentes (ad il y a qq jours)
Or download the App
NOT FOR COMMERCIAL USE
Patient A 60 ans, 130 kg, pas MCAS etc, très occupée, reins OK, diabète depuis 15-20 ans, A1C usuelles autour de 10-12% depuis qq années Gly 15-25 avec Lantus 30-0-0-30 et NR 30-30-30-0 et metformin 500 bid
Patient B 68 ans, DM x 35 ans sans MCAS mais avec DLPD et HTA, IMC 24 Tx avec metf 850 bid, gliclMR60x1, NPH 30 HS Gly am autour de 6-8, A1C 7.5 à 8.2% x 2 ans

Patient B2 68 ans, DM x 35 ans sans MCAS mais avec DLPD et HTA, IMC 24 Tx avec metf 850 bid, gliclMR60x1, NPH 30 HS Gly am autour de 6-8, A1C 8.2 à 8.7% x 1 an
Patient B3 68 ans, DM x 15 ans sans MCAS mais avec DLPD et HTA, IMC 33 Tx avec metf 850 bid, gliclMR60x1, NPH 30 HS Gly am autour de 6-8, A1C 8.2 à 8.7% x 1 an
2018 Diabetes Canada CPG – Chapter 13. Pharmacologic Glycemic Management of Type 2 Diabetes
GET TO TARGET
WITHIN
3-6 MONTHS
OF DIAGNOSIS
NOT FOR COMMERCIAL USEUne réduction précoce et énergique du taux
d’HbA1c apporte d’importants bienfaits
Réduction de L’atteinte rapide de l’équilibre
glycémique
37% aidera à réduire les
complications microvasculaires
des complications
microvasculaires* et macrovasculaires (IM)
Réduction
p < 0,0001 ultérieures (étude UKPDS)
du taux
d’HbA1c de Une intervention plus tardive
Réduction de avec une maîtrise glycémique
1% 14% stricte peut ne pas prévenir
les complications
des macrovasculaires
complications
macrovasculaires (décès d’origine CV, IM, AVC)
p < 0,0001
Une intervention précoce est primordiale pour prévenir les
complications du diabète à long terme
Les patients admis à l’étude UKPDS (N = 4585) présentaient un taux d’HbA1c initial de 9,1 %. Le groupe ayant reçu un
traitement classique a atteint un taux médian d’HbA1c sur 10 ans de 7,9 %, et le groupe ayant reçu un traitement intensif
par des hypoglycémiants facilement accessibles a atteint un taux d’HbA1c médian de 7,0 %.
* Incluant la rétinopathie, la neuropathie, la néphropathie, la maladie vasculaire périphérique; CV =
cardiovasculaire, IM = infarctus du myocarde; Stratton IM et al. BMJ 2000;321:405-412.Guidance Statement 1:
Clinicians should personalize goals for glycemic control in patients with
type 2 diabetes on the basis of a discussion of benefits and harms of
pharmacotherapy, patients' preferences, patients' general health and life
expectancy, treatment burden, and costs of care.
Guidance Statement 2:
Clinicians should aim to achieve an HbA1c level between 7% and 8% in
most patients with type 2 diabetes.
Guidance Statement 3:
Clinicians should consider deintensifying pharmacologic therapy in
patients with type 2 diabetes who achieve HbA1c levels less than 6.5%.
http://annals.org/aim/fullarticle/2674121/hemoglobin-1c-targets-
glycemic-control-pharmacologic-therapy-nonpregnant-adults-typeGuidance Statement 4:
Clinicians should treat patients with type 2 diabetes to
minimize symptoms related to hyperglycemia and avoid
targeting an HbA1c level in patients with a life expectancy less
than 10 years due to advanced age (80 years or older),
residence in a nursing home, or chronic conditions (such as
dementia, cancer, end-stage kidney disease, or severe
chronic obstructive pulmonary disease or congestive heart
failure) because the harms outweigh the benefits in this
population.
http://annals.org/aim/fullarticle/2674121/hemoglobin-1c-targets-
glycemic-control-pharmacologic-therapy-nonpregnant-adults-type2018 Diabetes Canada CPG – Chapter 13. Pharmacologic Glycemic Management of Type 2 Diabetes
GET TO TARGET
WITHIN
3-6 MONTHS
OF DIAGNOSIS
NOT FOR COMMERCIAL USE2018 Diabetes Canada CPG – Chapter 7. Self-Management Education and Support
Steps to Success
Evaluate and
support long-term
self-management
Implement a realistic plan
for skills training
Collaborate on decisions and
goals for action
Make informed consideration of
self-care options
Assess & identify personal self-care
needs
NOT FOR COMMERCIAL USE2018 Diabetes Canada CPG – Chapter 7. Self-Management Education and Support
Key Messages
Offer collaborative and interactive self-management
education and support
Incorporate problem solving, goal setting and self-
monitoring of health parameters for ongoing self-
management of clinical and psychosocial aspects of
care
Design and implement person-centred learning to
facilitate informed decision-making and achievement
of individual goals2018 Diabetes Canada CPG – Chapter 7. Self-Management Education and Support
Key Messages
Individualize self-management education interventions
according to the type of diabetes and recommended
therapy within the context of the individual’s ability for
learning and change, culture, health beliefs and
preferences, literacy level, socioeconomic status, and
other health challenges
Create and offer self-management support that
reflects person-centred goals and needs2018 Diabetes Canada CPG – Chapter 13. Pharmacologic Glycemic Management
of Type 2 Diabetes
Initial choice of therapy
Initiate healthy behavior
interventions and start metformin
A1C2018 AT DIAGNOSIS OF TYPE 2 DIABETES
Start healthy behaviour interventions
HEALTHY BEHAVIOUR INTERVENTIONS (nutritional therapy, weight management, physical activity) +/- metformin
Symptomatic hyperglycemia
A1C2018 Clinical CVD?
NO
Add additional antihyperglycemic agent best suited to the individual based
on the following
CLINICAL CONSIDERATIONS CHOICE OF AGENT
Avoidance of hypoglycemia and/or DPP-4 inhibitor, GLP-1 receptor
weight gain with adequate glycemic agonist or SGLT2 inhibitor
efficacy
Other considerations:
Reduced eGFR and/or albuminuria see Renal Impairment Appendix
Clinical CVD or CV risk factors
Degree of hyperglycemia See Table Below
Other comorbidities (CHF, hepatic
disease)
Planning pregnancy
Cost/coverage
Patient preference
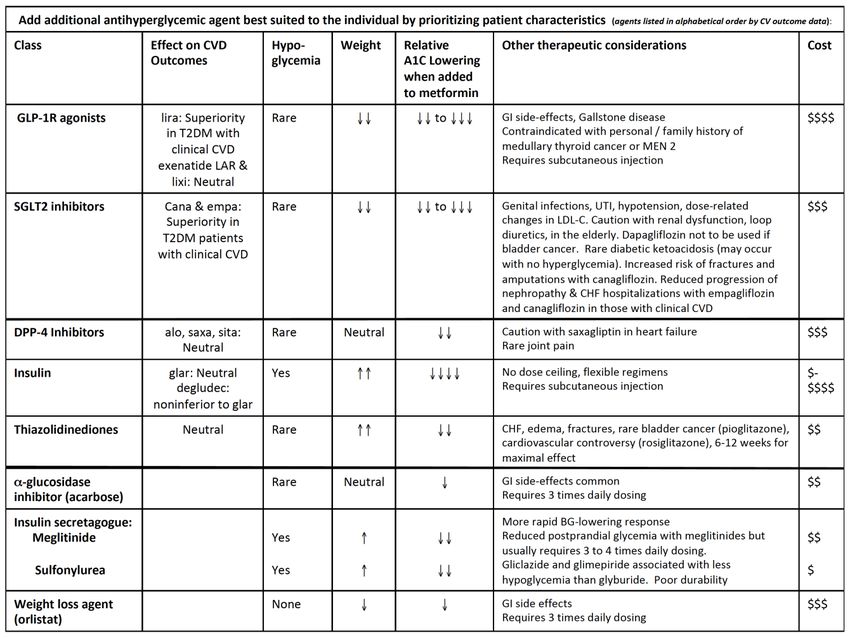
NOT FOR COMMERCIAL USEAdd additional antihyperglycemic agent best suited to the individual by prioritizing patient characteristics (agents listed in alphabetical order by CV outcome data):
Class Effect on CVD Hypo- Weight Relative Other therapeutic considerations Cost
Outcomes glycemia A1C Lowering
when added to
metformin
GLP-1R agonists lira: Superiority Rare to GI side-effects, Gallstone disease $$$$
in T2DM with Contraindicated with personal / family history of medullary
clinical CVD thyroid cancer or MEN 2
exenatide LAR & Requires subcutaneous injection
lixi: Neutral
SGLT2 inhibitors Cana & empa: Rare to Genital infections, UTI, hypotension, dose-related changes in $$$
Superiority in LDL-C. Caution with renal dysfunction, loop diuretics, in the
T2DM patients elderly. Dapagliflozin not to be used if bladder cancer. Rare
with clinical CVD diabetic ketoacidosis (may occur with no hyperglycemia).
Increased risk of fractures and amputations with
canagliflozin. Reduced progression of nephropathy & CHF
hospitalizations with empagliflozin and canagliflozin in those
with clinical CVD
DPP-4 Inhibitors alo, saxa, sita: Rare Neutral Caution with saxagliptin in heart failure $$$
Neutral Rare joint pain
Insulin glar: Neutral Yes No dose ceiling, flexible regimens $-
degludec: Requires subcutaneous injection $$$$
noninferior to glar
Thiazolidinediones Neutral Rare CHF, edema, fractures, rare bladder cancer (pioglitazone), $$
cardiovascular controversy (rosiglitazone), 6-12 weeks for
maximal effect
-glucosidase Rare Neutral GI side-effects common $$
inhibitor (acarbose) Requires 3 times daily dosing
Insulin secretagogue: More rapid BG-lowering response
Meglitinide Yes Reduced postprandial glycemia with meglitinides but usually $$
requires 3 to 4 times daily dosing.
Sulfonylurea Yes Gliclazide and glimepiride associated with less hypoglycemia $
than glyburide. Poor durability
Weight loss agent None GI side effects $$$
(orlistat) Requires 3 times daily dosingAdd additional antihyperglycemic agent best suited to the individual by prioritizing patient characteristics (agents listed in alphabetical order by CV outcome data):
Class Effect on CVD Hypo- Weight Relative Other therapeutic considerations Cost
Outcomes glycemia A1C Lowering
when added to
metformin
GLP-1R agonists lira: Superiority Rare to GI side-effects, Gallstone disease $$$$
in T2DM with Contraindicated with personal / family history of medullary
clinical CVD thyroid cancer or MEN 2
exenatide LAR & Requires subcutaneous injection
lixi: Neutral
SGLT2 inhibitors Cana & empa: Rare to Genital infections, UTI, hypotension, dose-related changes in $$$
Superiority in LDL-C. Caution with renal dysfunction, loop diuretics, in the
T2DM patients elderly. Dapagliflozin not to be used if bladder cancer. Rare
with clinical CVD diabetic ketoacidosis (may occur with no hyperglycemia).
Increased risk of fractures and amputations with
canagliflozin. Reduced progression of nephropathy & CHF
hospitalizations with empagliflozin and canagliflozin in those
with clinical CVD
DPP-4 Inhibitors alo, saxa, sita: Rare Neutral Caution with saxagliptin in heart failure $$$
Neutral Rare joint pain
Insulin glar: Neutral Yes No dose ceiling, flexible regimens $-
degludec: Requires subcutaneous injection $$$$
noninferior to glar
Thiazolidinediones Neutral Rare CHF, edema, fractures, rare bladder cancer (pioglitazone), $$
cardiovascular controversy (rosiglitazone), 6-12 weeks for
maximal effect
-glucosidase Rare Neutral GI side-effects common $$
inhibitor (acarbose) Requires 3 times daily dosing
Insulin secretagogue: More rapid BG-lowering response
Meglitinide Yes Reduced postprandial glycemia with meglitinides but usually $$
requires 3 to 4 times daily dosing.
Sulfonylurea Yes Gliclazide and glimepiride associated with less hypoglycemia $
than glyburide. Poor durability
Weight loss agent None GI side effects $$$
(orlistat) Requires 3 times daily dosingAdd additional antihyperglycemic agent best suited to the individual by prioritizing patient characteristics (agents listed in alphabetical order by CV outcome data):
Class Effect on CVD Hypo- Weight Relative Other therapeutic considerations Cost
Outcomes glycemia A1C Lowering
when added to
metformin
GLP-1R agonists lira: Superiority Rare to GI side-effects, Gallstone disease $$$$
in T2DM with Contraindicated with personal / family history of medullary
clinical CVD thyroid cancer or MEN 2
exenatide LAR & Requires subcutaneous injection
lixi: Neutral
SGLT2 inhibitors Cana & empa: Rare to Genital infections, UTI, hypotension, dose-related changes in $$$
Superiority in LDL-C. Caution with renal dysfunction, loop diuretics, in the
T2DM patients elderly. Dapagliflozin not to be used if bladder cancer. Rare
with clinical CVD diabetic ketoacidosis (may occur with no hyperglycemia).
Increased risk of fractures and amputations with
canagliflozin. Reduced progression of nephropathy & CHF
hospitalizations with empagliflozin and canagliflozin in those
with clinical CVD
DPP-4 Inhibitors alo, saxa, sita: Rare Neutral Caution with saxagliptin in heart failure $$$
Neutral Rare joint pain
Insulin glar: Neutral Yes No dose ceiling, flexible regimens $-
degludec: Requires subcutaneous injection $$$$
noninferior to glar
Thiazolidinediones Neutral Rare CHF, edema, fractures, rare bladder cancer (pioglitazone), $$
cardiovascular controversy (rosiglitazone), 6-12 weeks for
maximal effect
-glucosidase Rare Neutral GI side-effects common $$
inhibitor (acarbose) Requires 3 times daily dosing
Insulin secretagogue: More rapid BG-lowering response
Meglitinide Yes Reduced postprandial glycemia with meglitinides but usually $$
requires 3 to 4 times daily dosing.
Sulfonylurea Yes Gliclazide and glimepiride associated with less hypoglycemia $
than glyburide. Poor durability
Weight loss agent None GI side effects $$$
(orlistat) Requires 3 times daily dosingAdd additional antihyperglycemic agent best suited to the individual by prioritizing patient characteristics (agents listed in alphabetical order by CV outcome data):
Class Effect on CVD Hypo- Weight Relative Other therapeutic considerations Cost
Outcomes glycemia A1C lowering
when added to
metformin
GLP-1R agonists lira: Superiority Rare to GI side-effects, Gallstone disease $$$$
in T2DM with Contraindicated with personal / family history of medullary
clinical CVD thyroid cancer or MEN 2
exenatide LAR & Requires subcutaneous injection
lixi: Neutral
SGLT2 inhibitors Cana & empa: Rare to Genital infections, UTI, hypotension, dose-related changes in $$$
Superiority in LDL-C. Caution with renal dysfunction, loop diuretics, in the
T2DM patients elderly. Dapagliflozin not to be used if bladder cancer. Rare
with clinical CVD diabetic ketoacidosis (may occur with no hyperglycemia).
Increased risk of fractures and amputations with
canagliflozin. Reduced progression of nephropathy & CHF
hospitalizations with empagliflozin and canagliflozin in those
with clinical CVD
DPP-4 Inhibitors alo, saxa, sita: Rare Neutral Caution with saxagliptin in heart failure $$$
Neutral Rare joint pain
Insulin glar: Neutral Yes No dose ceiling, flexible regimens $-
degludec: Requires subcutaneous injection $$$$
noninferior to glar
Thiazolidinediones Neutral Rare CHF, edema, fractures, rare bladder cancer (pioglitazone), $$
cardiovascular controversy (rosiglitazone), 6-12 weeks for
maximal effect
-glucosidase Rare Neutral GI side-effects common $$
inhibitor (acarbose) Requires 3 times daily dosing
Insulin secretagogue: More rapid BG-lowering response
Meglitinide Yes Reduced postprandial glycemia with meglitinides but usually $$
requires 3 to 4 times daily dosing.
Sulfonylurea Yes Gliclazide and glimepiride associated with less hypoglycemia $
than glyburide. Poor durability
Weight loss agent None GI side effects $$$
(orlistat) Requires 3 times daily dosingAdd additional antihyperglycemic agent best suited to the individual by prioritizing patient characteristics (agents listed in alphabetical order by CV outcome data):
Class Effect on CVD Hypo- Weight Relative Other therapeutic considerations Cost
Outcomes glycemia A1C Lowering
when added to
metformin
GLP-1R agonists lira: Superiority Rare to GI side-effects, Gallstone disease $$$$
in T2DM with Contraindicated with personal / family history of medullary
clinical CVD thyroid cancer or MEN 2
exenatide LAR & Requires subcutaneous injection
lixi: Neutral
SGLT2 inhibitors Cana & empa: Rare to Genital infections, UTI, hypotension, dose-related changes in $$$
Superiority in LDL-C. Caution with renal dysfunction, loop diuretics, in the
T2DM patients elderly. Dapagliflozin not to be used if bladder cancer. Rare
with clinical CVD diabetic ketoacidosis (may occur with no hyperglycemia).
Increased risk of fractures and amputations with
canagliflozin. Reduced progression of nephropathy & CHF
hospitalizations with empagliflozin and canagliflozin in those
with clinical CVD
DPP-4 Inhibitors alo, saxa, sita: Rare Neutral Caution with saxagliptin in heart failure $$$
Neutral Rare joint pain
Insulin glar: Neutral Yes No dose ceiling, flexible regimens $-
degludec: Requires subcutaneous injection $$$$
noninferior to glar
Thiazolidinediones Neutral Rare CHF, edema, fractures, rare bladder cancer (pioglitazone), $$
cardiovascular controversy (rosiglitazone), 6-12 weeks for
maximal effect
-glucosidase Rare Neutral GI side-effects common $$
inhibitor (acarbose) Requires 3 times daily dosing
Insulin secretagogue: More rapid BG-lowering response
Meglitinide Yes Reduced postprandial glycemia with meglitinides but usually $$
requires 3 to 4 times daily dosing.
Sulfonylurea Yes Gliclazide and glimepiride associated with less hypoglycemia $
than glyburide. Poor durability
Weight loss agent None GI side effects $$$
(orlistat) Requires 3 times daily dosingAdd additional antihyperglycemic agent best suited to the individual by prioritizing patient characteristics (agents listed in alphabetical order by CV outcome data):
Class Effect on CVD Hypo- Weight Relative Other therapeutic considerations Cost
Outcomes glycemia A1C Lowering
when added to
metformin
GLP-1R agonists lira: Superiority Rare to GI side-effects, Gallstone disease $$$$
in T2DM with Contraindicated with personal / family history of medullary
clinical CVD thyroid cancer or MEN 2
exenatide LAR & Requires subcutaneous injection
lixi: Neutral
SGLT2 inhibitors Cana & empa: Rare to Genital infections, UTI, hypotension, dose-related changes in $$$
Superiority in LDL-C. Caution with renal dysfunction, loop diuretics, in the
T2DM patients elderly. Dapagliflozin not to be used if bladder cancer. Rare
with clinical CVD diabetic ketoacidosis (may occur with no hyperglycemia).
Increased risk of fractures and amputations with
canagliflozin. Reduced progression of nephropathy & CHF
hospitalizations with empagliflozin and canagliflozin in those
with clinical CVD
DPP-4 Inhibitors alo, saxa, sita: Rare Neutral Caution with saxagliptin in heart failure $$$
Neutral Rare joint pain
Insulin glar: Neutral Yes No dose ceiling, flexible regimens $-
degludec: Requires subcutaneous injection $$$$
noninferior to glar
Thiazolidinediones Neutral Rare CHF, edema, fractures, rare bladder cancer (pioglitazone), $$
cardiovascular controversy (rosiglitazone), 6-12 weeks for
maximal effect
-glucosidase Rare Neutral GI side-effects common $$
inhibitor (acarbose) Requires 3 times daily dosing
Insulin secretagogue: More rapid BG-lowering response
Meglitinide Yes Reduced postprandial glycemia with meglitinides but usually $$
requires 3 to 4 times daily dosing.
Sulfonylurea Yes Gliclazide and glimepiride associated with less hypoglycemia $
than glyburide. Poor durability
Weight loss agent None GI side effects $$$
(orlistat) Requires 3 times daily dosing2018 Diabetes Canada CPG – Chapter 13. Pharmacologic Glycemic Management of Type 2 Diabetes
2018
If not at glycemic targets
Add another antihyperglycemic agent from a different class and/or add/intensify insulin regimen
Make timely adjustments to attain target A1C within 3-6 months2018 Diabetes Canada CPG – Chapter 13. Pharmacologic Glycemic Management of Type 2 Diabetes
Antihyperglycemic Agents and Renal Function
CKD Stage 5 4 3b 3a 1 or 2
eGFR (mL/min/1.73 m2): 30 ml/min/1.732Messages (DM2)
Les lignes directrices viennent de changer et les infos
sont en général claires et complètes
Attention, cible A1C plus conservatrice cependant, ok
entre 7 et 8% pour la plupart des patients
Si votre patient va bien, pas nécessaire de chambouler
son Tx
sauf si en présence de maladie cardiovasculaire
avérée…
Important de considérer franchir des « étapes
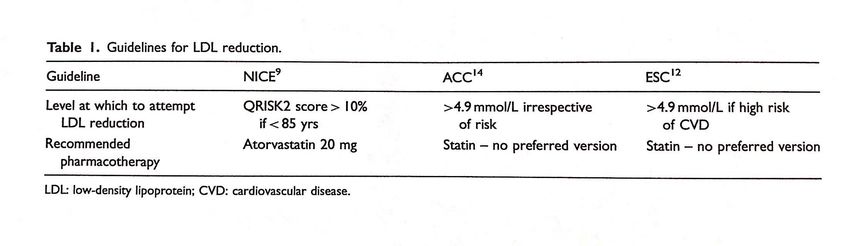
préalables » (RAMQ)Dlpd et prévention « primaire »
Patient Z H50 avec CT 6, LDL à 4.5, HDL 1.1, TG 2 Non fumeur, en forme, pas DM ni HTA, adopté Préfère les demi-ironman aux médicaments Votre recommandation?
Patient Y H35 avec CT 6, LDL à 4.5, HDL 1.2, TG 2 Non fumeur, en forme, pas DM ni HTA Père a fait IM à 75 ans Votre recommandation?
Dlpd et prévention « primaire » Plusieurs éléments sont assez clairs dont lorsque risque considéré élevé: on traite (statine) LDL 5 et plus (HCF) 40 ans et plus avec DM ou autre FR signficatif Quelques zones moins claires 21-40 ans et LDL entre 4 et 5 avec ou sans FR 40-75 ans et LDL entre 4 et 5 sans FR
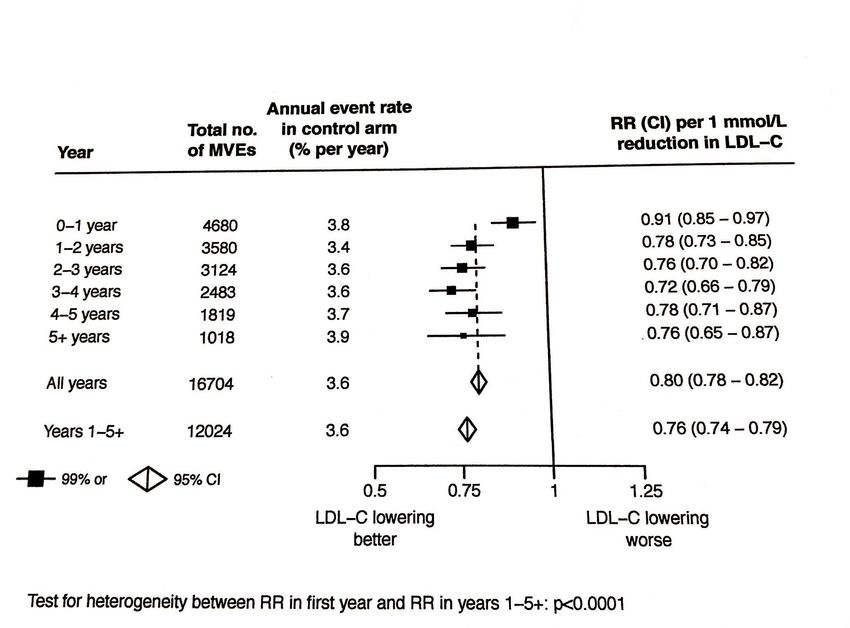
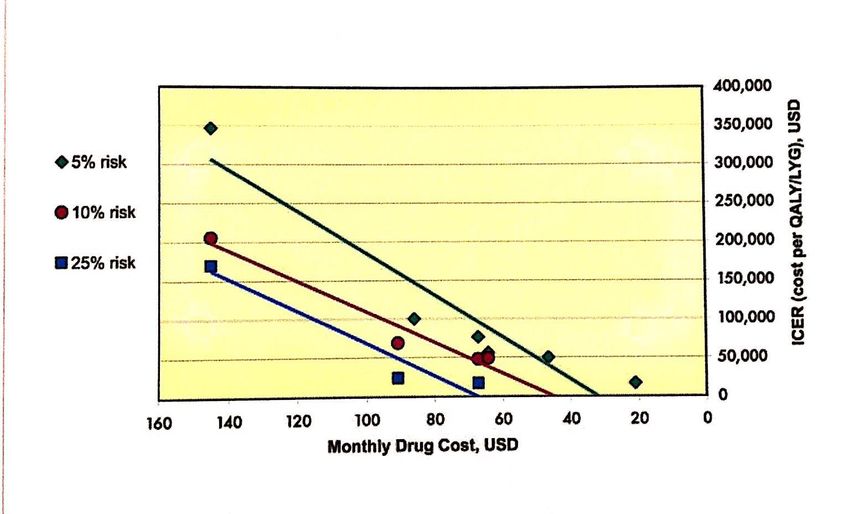
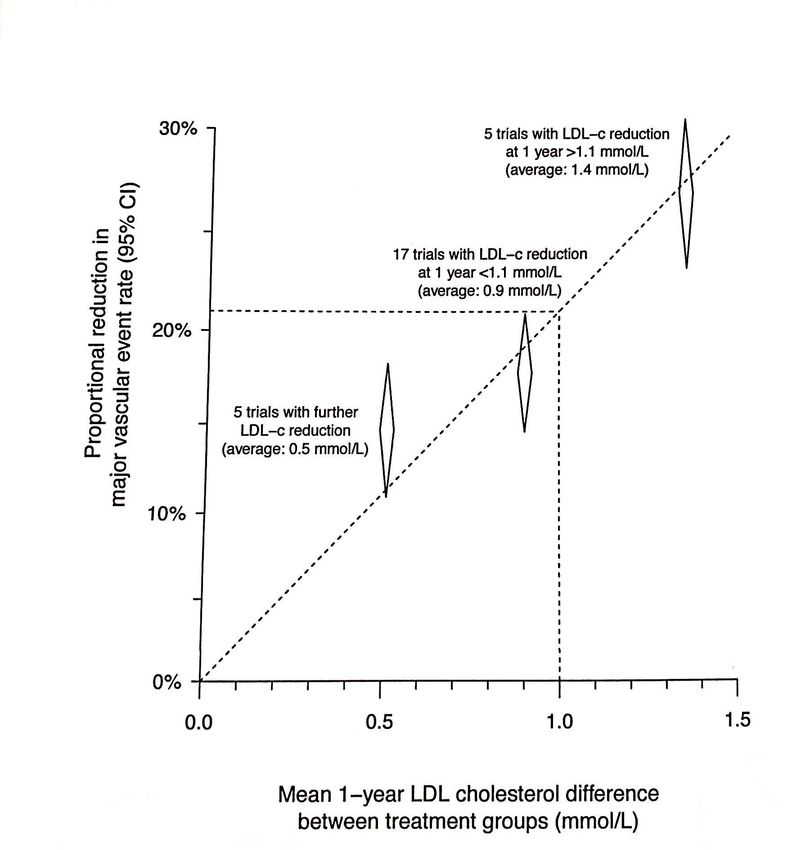
https://spiral.imperial.ac.uk:8443/handle/10044/1/43661
simulation
Disons que pour un patient donné de 40+ ans, on
obtient 10% de FR CV sur 10 ans
Avec statine on réduit de 25% donc de 10 à 7.5%
Donc risque annuel de 1% à 0.75%
L’inverse est de dire que l’on améliore la survie annuelle sans
événement de 99 à 99.25%
Donc pour les patients de 40+ ans à plus faible risque
avec LDL entre 4 et 5, il est difficile d’insister pour
initier un Tx car les évidences prospectives sont moins
solides, donc à individualiser, et Tx max n’est pas
indiquéMessages (DLPD-PP) Bien considérer tous les FR pour la prévention primaire LDL en haut de 5 mérite Tx haute intensité Mais 21-40 ans: niveau = op d’expert LDL entre 4 et 5 avec FR : Tx mod-haute intensité LDL entre 4 et 5 sans FR: discutable iPSK9: bonne chance…
Diabetes Canada Clinical Practice
Guidelines
http://guidelines.diabetes.ca – for health-care providers
1-800-BANTING (226-8464)
http://diabetes.ca – for people with diabetes2018 Diabetes Canada CPG – Chapter 13. Pharmacologic Glycemic Management of Type 2 Diabetes
Empagliflozin reduced CV events
CV death, non-fatal MI, or non-fatal stroke
PBO EMP HR P NNT3
A
CV death, MI, stroke (%) 12.1 10.5 0.86 0.04 63
CV deaths (%) 5.9 3.7 0.622018 Diabetes Canada CPG – Chapter 13. Pharmacologic Glycemic Management of Type 2 Diabetes
Liraglutide reduced CV events
CV death, non-fatal MI, or non-fatal stroke
PBO LIRA HR P NNT4
CV death, MI, stroke (%) 14.9 13.0 0.87 0.01 53
CV death (%) 6.0 4.7 0.78 0.007 77
Nonfatal MI (%) 6.8 6.0 0.88 0.11
Nonfatal stroke (%) 3.8 3.4 0.89 0.30
Patients with event (%)
Hosp. heart failure (%) 5.3 4.7 0.87 0.14
All-cause mortality (%) 9.6 8.2 0.85 0.02 72
Placebo
Liraglutide
HR 0.87
95.02% CI (0.78, 0.97)
P < 0.001 for non-inferiority
p=0.01 for superiority
Time from randomization (months)
Patients at risk
Liraglutide 4668 4593 4496 4400 4280 4172 4072 3982 1562 424
Placebo 4672 4588 4473 4352 4237 4123 4010 3914 1543 407
Marso SP et al. N Engl J Med 2016;375(4):311-22.
NOT FOR COMMERCIAL USE2018 Diabetes Canada CPG – Chapter 13. Pharmacologic Glycemic Management of Type 2 Diabetes
Canagliflozin reduced CV events
CV death, non-fatal MI, or non-fatal stroke
Outcome PBO CANA HR P or 95% CI NNT 5
(per 1000 pt-y)
CV death, MI, stroke 31.5 26.9 0.86 0.02 44
CV deaths 12.8 11.6 0.87 (0.72-1.06)
Nonfatal MI 11.6 9.7 0.85 (0.69-1.05)
Nonfatal stroke 8.4 7.1 0.90 (0.71-1.15) Placebo
Hosp. heart failure 8.7 5.5 0.67 (0.52-0.87) 63 Canagliflozin
All-cause mortality 19.5 17.3 0.87 (0.74-1.01)
HR 0.86
95% CI (0.75, 0.97)
P < 0.001 for non-inferiority
p=0.02 for superiority
No. of patients
Canagliflozin 5795 5566 4343 2555 2460 2363 1661
Placebo 4347 4153 2942 1240 1187 1120 789
Neal B et al. N Engl J Med 2017; DOI:10.1056/NEJMoa1611925 NOT FOR COMMERCIAL USELiraglutide et résultats CV dans le diabète de type 2
(LEADER) – Prévention primaire
L’essai LEADER comprenait des patients de 60 ans et plus avec au
moins un facteur de risque CV
Microalbuminurie ou protéinurie, hypertension et hypertrophie ventriculaire
gauche, dysfonction systolique ou diastolique ventriculaire gauche, ou un
indice de pression systolique à moins de 0,9
N = 1742 (18,7 %) pour la prévention primaire
Nombre Valeur p pour
Sous-groupe de patients Liraglutide Placebo RRI (IC à 95 %) l’interaction
Nbre d’événements/Nbre de patients (%)
Risque de maladie
cardiovasculaire
0,04
≥ 50 ans et maladie CV diagnostiquée 7598 536/3831 (14,0) 629/3767 (16,7) 0,83 (0,74-0,93)
xxxx
≥ 60 ans et présence de facteurs de risques CV 1742 72/837 (8,6) 0,265/905 (7,2) 0,0 2,0 1,20 (0,86-1,67)
En faveur du liraglutideEn faveur du placebo
Steven P. Marso, Gilbert H. Daniels, Kirstine Brown-Frandsen, Peter Kristensen, Johannes F.E. Mann,
Michael A. Nauck, Steven E. Nissen et al. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. New England Journal of Medicine 375, no. 4 (28 juillet 2016) : 311–22. doi :
10.1056/NEJMoa1603827.Sommaire des études sur les hypoglycémiants et les résultats
cardiovasculaires
Prévention secondaire Prévention primaire
Études publiées (Critère d’évaluation (Critère d’évaluation
principal) principal)
EMPA-REG OUTCOME (essai
Ne fait pas partie de l’essai
clinique randomisé)
LEADER (essai clinique
Non significatif
randomisé)
SUSTAIN-6 (essai clinique
Non significatif
randomisé)
CANVAS PROGRAM (essai
Non significatif
clinique randomisé)
CVD-REAL (en situation réelle) Décès toutes causes confondues et IC chez les nouveaux
utilisateurs d’inhibiteurs du SGLT2 avec et sans MCV (étude CVD-
REAL)
Événement N Nbre d’événements RRI (IC à 95 %)
Avec antécédents CV* 30 153 569 0,47 (0,36, 0,61)
Décès
Sans antécédent CV* 185 469 765 0,54 (0,44,
0,66)
Avec antécédents CV* 39 293 706 0,69 (0,59,
IC 0,80)
Sans antécédent CV* 266 863 244 0,45 (0,32,
0,63)
Avec antécédents CV* 30 153 1084 0,59 (0,52,
IC et décès 0,67)
Sans antécédent CV* 185 469 899 0,52 (0,44,
0,61)
En faveur des inhibiteurs du SGLT2 En faveur des autres hypoglycémiants
0,25 0,50 1,00 2,00
Rapport de risques
*Diagnostic d’infarctus aigu du myocarde, angine de poitrine instable, accident vasculaire cérébral, insuffisance cardiaque, accident ischémique transitoire,
revascularisation coronarienne ou maladie artérielle périphérique occlusive avant le début de la prise du médicament de référence.
M.A. Cavender et al. Résumé 377-OR présenté lors des 77e séances scientifiques de l’American Diabetes Association, du 9 au 13 juin, San Diego, CA, É.-U.Vous pouvez aussi lire