HIGHLIGHT PUBLICATIONS 2019 - Filière FAVA-Multi
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous
HIGHLIGHT
PUBLICATIONS 2019
Filière FAVA-Multi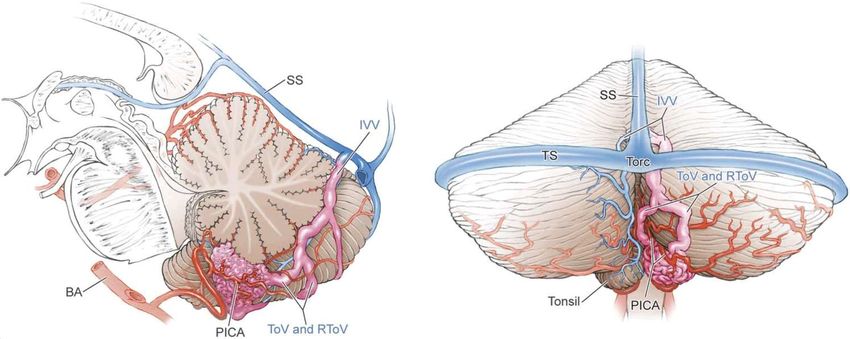
SYNDROME DE MARFAN & APPARENTÉS
Pathogenic FBN1 Genetic Variation and Aortic Dissection in Patients With Marfan Syndrome
Olivier Milleron, Florence Arnoult, Gabriel Delorme, Delphine Detaint, Quentin Pellenc, Richard
Raffoul, Maria Tchitchinadze, Maud Langeois, Celine Guien, Christophe Beroud, Jacques
Ropers, Nadine Hanna, Pauline Arnaud, Laurent Gouya, Catherine Boileau, Guillaume Jondeau
Incidence of cardiovascular events and risk markers in a prospective study of children
diagnosed with Marfan syndrome
Sebastien Hascoet, Thomas Edouard, Julie Plaisancie, Florence Arnoult, Olivier
Milleron, Chantal Stheneur, Bertrand Chevallier, Cécile Zordan, Sylvie Odent, Laurence
Bal, Laurence Faivre, Bruno Leheup, Sophie Dupuis-Girod, Jean-Bernard Ruidavets, Philippe
Acar, Jean Ferrieres, Guillaume Jondeau, Yves Dulac
European reference network for rare vascular diseases (VASCERN) consensus statement for
the screening and management of patients with pathogenic ACTA2 variants ?
Ingrid M B H van de Laar, Eloisa Arbustini, Bart Loeys, Erik Björck, Lise Murphy, Maarten
Groenink, Marlies Kempers, Janneke Timmermans, Jolien Roos-Hesselink, Kalman
Benke, Guglielmina Pepe, Barbara Mulder, Zoltan Szabolcs , Gisela Teixidó-Turà, Leema
Robert, Yaso Emmanuel, Arturo Evangelista, Alessandro Pini, Yskert von Kodolitsch, Guillaume
Jondeau, Julie De Backer
2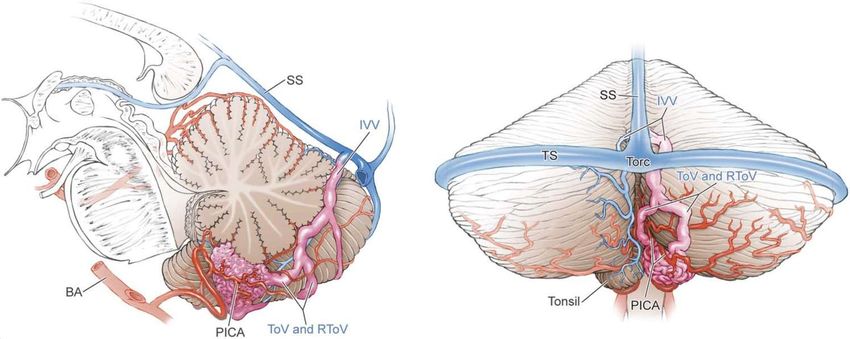
• 1306 MFS patients, 18 years at least (18-89 years) • 999 included, 674 families
Hascoët et al. Archives of Cardiovascular Diseases
113, 2020, 40-49
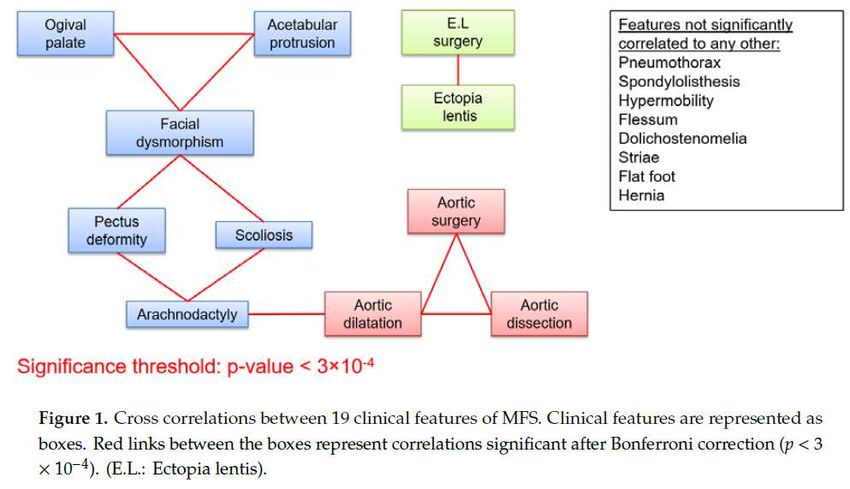
Objectifs: étudier l’incidence et les marqueurs de risque
d’événements cardiovasculaires des enfants avec syndrome
de Marfan
Méthodes: 462 patients de la base de données
multicentrique Marfan diagnostiqués pendant l’enfance
Critère de Jugement principal: survenue d’ événements:
- Décès
- Dissection
- Chirurgie prophylactique de l’aortePopulation: base de données multicentrique • 462 enfants (1993-2013) • Garçons: 52% • Age médian au diagnostic: 10,3 (5,6-14) ans • Suivi médian : 5,4 ans (2-11,2) • Mutation génétique: 74,5% • Dilatation aortique: 77,4% ü Z-score sinus Valsalva > 3: 37% ü Z-score sinus Valsalva > 3 avant 16 ans: 27,3% • Bétabloquants: 75%
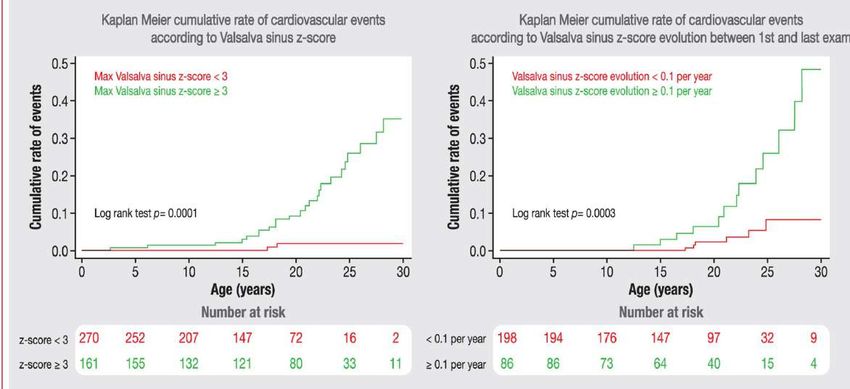
Résultats Evénements cardiovasculaires: 35/462 (7,6%) Evénements cardiovasculaires < 19 ans : 19/203: 9,4% (5,7-14,2) - Dissection type A: 2 (15.0 - 15.9 ans) - Décès: 3 (3,4 - 16,5 - 18,2 ans) - Chirurgie aortique prophylactique: 15 (2,4-18 ans) Evénements cardiovasculaires < 16 ans : 11/269: 4,1% (2,1-7,2)
Résultats
Conclusions • Les événements cardio-vasculaires chez les enfants ayant un syndrome de Marfan sont essentiellement les chirurgies prophylactiques de la racine aortique. • Les dissections aortiques sont exceptionnellement observées chez l’enfant. • Le Z-score du sinus de Valsalva est un marqueur fort prédictif de la survenue d’événements cardio-vasculaires.
RENDU-OSLER
Efficacy and Safety of a 0.1% Tacrolimus Nasal Ointment as a Treatment for Epistaxis in
Hereditary Hemorrhagic Telangiectasia: A Double-Blind, Randomized, Placebo-
Controlled, MulLcenter Trial
Sophie Dupuis-Girod, Anne-Emmanuelle Fargeton, Vincent Grobost, Sophie Rivière, Marjolaine
Beaudoin, Evelyne Decullier, Lorraine Bernard, ValenYne Bréant,
BeZna Colombet, Pierre Philouze, Sabine Bailly, Frédéric Faure and Ruben Hermann
Hereditary haemorrhagic telangiectasia and pregnancy: a review of the literature
Dupuis O, Delagrange L, Dupuis-Girod S. Orphanet J Rare Dis. 2020 Jan
Future treatments for hereditary hemorrhagic telangiectasia
Robert F, Desroches-Castan A, Bailly S, Dupuis-Girod S, Feige JJ.Orphanet J Rare Dis. 2020 Jan
7;15(1):4.
2021
Applications nasales
2x/jour
pendant 6 semaines22 - 5 case series - 31 case reports - 1577 pregnancies in 630 women with HHT. - Overall maternal death rate estimated at 1.0% of pregnancies in the case series and 2 maternal deaths occurred in 31 pregnancy case reports. - Severe maternal complications occurred in 2.7 to 6.8% of pregnancies in the case series. Severe complications occurred mostly in the second and third trimester in non-diagnosed and non-screened HHT patients. - most frequent complications related to PAVMs (haemothorax (n = 10), haemoptysis (n = 4), and severe hypoxaemia (n = 3)). - Complications were related to hepatic arteriovenous malformations (HAVMs) in 8 cases (acutely decompensated heart failure due to hepatic involvement (n = 1), dyspnoea related to heart failure (n = 5), and hepatobiliary necrosis (n = 2)).
* HHT mutations lead to inhibition of the pro-angiogenic pathways (VEGF)
BMP9
*
VEGF
*
ENG
ALK1/RII* VEGFR2
PI3K PLCg src
Smad 1/5/9
Smad4
*
PTEN AKT ERK P38 MAPK
EC survival EC migraLon
EC permeability
ANGPT2, VEGFR1, … EC proliferationHHT anti-angiogenic treatments Anti-VEGF
BMP9
*
VEGF
VEGFR2-TKI
*
ENG
ALK1/RII* VEGFR2
PI3K PLCg src
Smad 1/5/9
Smad4
*
PTEN AKT ERK P38 MAPK
EC survival EC migration
EC permeability
ANGPT2, VEGFR1, … EC proliferationFuture HHT treatments Anti-ANGPT2 AnL-VEGF
BMP9
* ANGPT2 VEGF
Tacrolimus
Sirolimus VEGFR2-TKI
Tie2
*
ENG
ALK1/RII* VEGFR2
PI3K
Inhibitor PI3K PLCg src
Smad 1/5/9
Smad4
*
PTEN AKT ERK P38 MAPK
EC survival EC migration
EC permeability
ANGPT2, VEGFR1, … EC proliferation
Robert F, et al., Future treatments for HHT.
Orphanet J Rare Dis 2020MALADIES VASCULAIRES RARES
Syndrome d’Ehlers-Danlos vasculaire
Classical Ehlers-Danlos syndrome with a propensity to arterial events: A new report on a
French family with a COL1A1 p.(Arg312Cys) variant
Salma Adham, Sophie Dupuis-Girod, Etienne Charpentier, Jean-Michaël Mazzella, Xavier
Jeunemaitre, Anne Legrand
Malformations lymphatiques et lymphœdème primaire
Clinical and Scintigraphic Predictors of Primary Lower Limb Lymphedema-Volume
Reduction During Complete Decongestive Physical Therapy
Stéphane Vignes, Laura Simon, Bani Benoughidane, Magali Simon, Caroline Fourgeaud
Out-of-pocket payments, vertical equity and unmet medical needs in France: A national
multicenter prospective study on lymphedema
Gregoire Mercier, Jenica Pastor, Valerie Clément, Ulysse Rodts, Christine Moffat, Isabelle
Quéré
26Cas Clinique COL1A1 p.Arg312Cys 26/06/2020 –JOURNÉE ANNUELLE FAVA MULTI DR ANNE LEGRAND DR SOPHIE DUPUIS-GIROD DR SALMA ADHAM
Les syndromes d’Ehlers-Danlos
u SED vasculaire
u COL3A1
u Dissections/ruptures artérielles, perforation colique, rupture utérine T3,
FCC
u SED classique
u COL5A1 (90%), COL5A2
u Hyper extensibilité cutanée, cicatrices atrophiques, hyperlaxité
généraliséePhénotypes frontières
u Hyperlaxité articulaire, fragilité cutanée, fragilité artérielle
u Existence de complications artérielles dans des sous-types de SED non vasculaire
u Dans le SEDv, peu de complications articulaires et cutanées comparativement au
SEDc
u Variant COL1A1 p.Arg312Cys Malfait et al. 2007Arbre généalogique
†64y 87y †58y 81y
I-1 I-2 I-3 I-4
67y 66y 61y 59y 57y
3
II-1 II-2 II-3 II-4 II-5
41y †23y 23y 29y 33y 29y
3
III-1 III-5 III-6 III-7 III-8 III-9Hallux valgus opéré, recurvatum des genoux et pigmentation hémo-sidérémique
Déchaussement dentaire
Hyperextensibilité et transparence cutanée
Complications artérielles
Complications artérielles
Diagnostic moléculaire
u Sanger
u COL3A1 c.3818A>G, p.Lys1273Arg
u Propeptide C-terminal
u Ségrégation familiale
u Co-ségrégation avec le phénotype obstétrical de sa sœur
(II:1)
u Absence de co-segregation avec les signes mineurs de la
mère (I:2)
u Panel de gènes
u COL3A1, COL1A1, COL1A2, COL5A1, COL5A2, FBN1,
SMAD3, TGFß2, TGFßR1 et TGFßR2
u COL1A1 c.934C>T, p.Arg312CysSégrégation familiale
COL1A1 c.934C>T, p.Arg312Cys
COL3A1 c.3818A>G, p.Lys1273Arg
†64y 87y †58y 81y I-2
COL3A1 +/+
COL1A1 +/-
I-1 I-2 I-3 I-4
II-1
67y 66y 61y 59y 57y
COL3A1 +/- COL3A1 +/- COL3A1 +/+
COL1A1 +/+ COL1A1 +/- COL1A1 +/+
3
II-1 II-2 II-3 II-4 II-5
II-3
41y †23y 23y 29y 33y 29y
3
III-1 III-5 III-6 III-7 III-8 III-9
II-4Discussion
u Fréquence en population générale
u Critère majeur pour l’interprétation des variations
u GnomAD
u COL1A1 c.934C>T, p.Arg312Cys à Absent
u COL3A1 c.3818A>G, p.Lys1273Arg à Européens: 2,7x10-4 et total: 1,2x10-4
u Seuils proposés – littérature
u 0,01% Kobayashi et al. Genome Medicine 2017
u 2x10-5 (prévalance 1/50.000) Whiffin et al. Genet Med 2017
u COL3A1 c.3818A>G, p.Lys1273Arg
u Reclassé bénin (ACMG)
u Fréquence supérieure à celle attendee
u Autre variation pathogène identifiée
u Variation classée 1x bénigne – ClinVar
u Rôle modificateur?Discussion
u Ségrégation familiale incomplète
u Expression cellulaires des collagènes I et III
u 3e cas décrit de complication artérielle porteur du variant
COL1A1 p.Arg312Cys
u Hétérogénéité inter et intra familiale
u Panel incluant COL1A1
u Complication artérielle + phénotype classique et COL3A1 négatif
u Phénotype classique atténué et COL5A1/A2 négatifs
u Diagnostics difficilesPrévalence des complications artérielles dans le
SEDv, le SEDc et chez les patients COL1A1
p.Arg312Cys
Types de SED Prévalence Référence
Frank et al 2015; Shalhub et al
SEDv 72% 2014
Ritelli et al 2013; Symoens et al
SEDc 0 to 2.15% (0/40 and 2/93) 2012
Gaines et al 2015; Malfait et al
COL1A1 p.Arg312Cys 21.4% (3/14) 2007; and current case reportDiscussion
u Pas de guidelines à ce jour
u Prise en charge comme SED vasculaire si complication
artérielle ?
u Intérêt de bilans artériels en l’absence de complication
artérielle ?
u Céliprolol ?MALADIES VASCULAIRES RARES
Syndrome d’Ehlers-Danlos vasculaire
Classical Ehlers-Danlos syndrome with a propensity to arterial events: A new report on a
French family with a COL1A1 p.(Arg312Cys) variant
Salma Adham, Sophie Dupuis-Girod, Etienne Charpentier, Jean-Michaël Mazzella, Xavier
Jeunemaitre, Anne Legrand
Malformations lymphatiques et lymphœdème primaire
Clinical and Scintigraphic Predictors of Primary Lower Limb Lymphedema-Volume
Reduction During Complete Decongestive Physical Therapy
Stéphane Vignes, Laura Simon, Bani Benoughidane, Magali Simon, Caroline Fourgeaud
Out-of-pocket payments, vertical equity and unmet medical needs in France: A national
multicenter prospective study on lymphedema
Gregoire Mercier, Jenica Pastor, Valerie Clément, Ulysse Rodts, Christine Moffat, Isabelle
Quéré
42Original Research Lymphology, Hôpital Cogna
p.com/ptj/article-abstract/100/5/766/5707306 by bibliotheque interuniv
Lymphology,
sufficiency, heart failure, hypoprotidemiaHôpital Cognacq-Jay. etc.)—ruled Caroline Four
Clinical
S. Vignes, MD, Department of
ut by physical examination and Scintigraphic
and complementary
Lymphology, Hôpital Cognacq-Jay, 15, [Vignes S, Simon L, Benough
[VignesPredictors
S, Simon L,
rue Eugène-Millon, 75015 Paris,
of Benoughidane
Primary LowerB, Limb
xplorations, such as ultrasound, computed-tomography
France. Address all correspondence to
Dr Vignes at: Simon M, Fourgeaud C. Clin
Simon Lymphedema-Volume
M,imaging
Fourgeaud (Fig.C. 1).Clinical andscintigraphic predictors of p
Downloaded from https://academic.oup.com/ptj/article-abstract/100/5/766/5707306 by bibliotheque interuniversitaire de medecine use
stephane.vignes@cognacq-jay.fr.
an, or magnetic resonance
L. Simon, MD, Department of
Reduction
scintigraphic DuringofComplete
predictors
Lymphology, Hôpital Cognacq-Jay.
B. Benoughidane, MD, Department of primary lower limb lymphedema-vol Background
Lymphology, Hôpital Cognacq-Jay.
or this study, all consecutive Decongestive
lower limb patients Physicalin
consulting
lymphedema-volume
M. Simon, MD, Department of
Lymphology, Hôpital Cognacq-Jay.
Therapy
our reduction curative treatm
during complete
epartment for unilateral primary
reductionCarolineduring
lower limb lymphedema
Stéphane Vignes, Laura Simon, Bani Benoughidane, Magali Simon,
C. Fourgeaud, MD, Department of
Fourgeaud complete
Lymphology, Hôpital Cognacq-Jay.
decongestive volume, where
physical therap
uppl. Fig. 1, available at https://academic.oup.com/ptj)
[Vignes S, Simon L, Benoughidane B,
decongestive
Background. physical therapy. Phys Ther. 2020;100:766–772.]
Simon M, Fourgeaud C. Clinical and
Primary lower limb lymphedema
scintigraphic predictors of primary is a chronic debilitating disorder without
Primary Lymphedema-Volume Reduction
etween January 2009 andvolume, December 2017 and treated
curative treatment. The initial treatment phase is dedicated to reducing lymphedema
Objective.
lower limb lymphedema-volume
Ther. 2020;100:766–772.] © 2020 American Physical T
whereas the second aims to stabilize that volume.
reduction during complete
ith complete decongestive physical therapy were
decongestive physical therapy. Phys
Ther. 2020;100:766–772.] T
Objective. The objective of this study was to analyze clinical and lymphoscintigraphic
characteristics
characteristics during complete decongestive physical therapy as predictors of primary
cluded. Stemmer’s©sign
Association
2020(Suppl.
unilateral lowerFig.
© 2020 American Physical Therapy
American 2,Physical
available
limb lymphedema-volume at
Therapy
reduction. Association
tps://academic.oup.com/ptj),
Published Ahead of Print:
Design. This considered to bestudy included 222 consecutive patients
( January 2009–January 2017; median age: 45.8 years) with lymphedema affecting theunilateral lowe
January 16, 2020 observational, retrospective
Association
Downloaded from https://academic.oup.com/ptj/article-a
lower limb, who received complete decongestive physical therapyPublished for the first time in aAhead of Print:
Accepted: November 18, 2019 entire
athognomonic of lymphedema,
Submitted: January 24, 2019
was required
specialized lymphedema management center.
for all
atients; it is not seen in lower limb January 16, 2020
Published Methods. Complete edema
Ahead of Print:
decongestive of other
physical therapy consisted of low-stretch bandaging,
auses.
manual lymph drainage, exercises, and skin care for all patients. Lymphoscintigraphy
January 16, 2020
preceded treatment. Design.
Accepted: November 18, Thi20
Results. Median lymphedema evolution was 73 months, and median Submitted:
excess volume was January 24, 2019
34%. Median (interquartile range) lymphedema volumes were 2845 (1038–3487) mL ( January 2009–
ecause no specific definition Accepted: and 1276November
for lower limb lymphedema 18,
(601–2195) mL after a median of2019
11 days of complete decongestive physical
before
we increased lower limb, wh
therapy, with 34% median reduction. Multivariate analyses retained age, body mass
xists using differences Submitted:
in index
volume
January
circumferences
>40 kg/m 2
24,
, and previous
or2019 volumes,
cellulitis,
reduction. For each additional
as independently associated with lymphedema
year of age, volume reduction 0.16%.
referred using the volumethatdifference
Unexpectedly, log-transformed initial lymphedema volumes indicated a negative impact,
between
is, 4.95%, for each log-unit the
gain. Patients with
2
specialized lym
previous cellulitis episode(s) obtained
6.9% and those with BMI >40 kg/m 17.1% higher lymphedema volume reductions. Lower
fected and normal lower limb limbs. For upper
lymphoscintigraphy was available limb
for 150 (67.6%) patients. Having dermal back flow
was associated with greater lymphedema volume reduction than not (respectively, 39% vs
mphedema after breast cancer
ct patients with primary lower limb lymphedema
treatment, Armer and
treated for the first time with complete decongestive therapy.
Methods.
31%).
ewart analyzed all the published Limitations. This study was retrospective, and only 67.6% of patients underwent
lymphoscintigraphy. definitions and Cocurative treatment. The initial treatment phase is dedicated to reducing lymphedema
volume, whereas the second aims to stabilize that volume.
Objective. The objective of this study was to analyze clinical and lymphoscintigraphic
characteristics during complete decongestive physical therapy as predictors of primary
unilateral lower limb lymphedema-volume reduction.
Predictors of Primary Lymphedema-Volume Reduction
Design. This observational, retrospective study included 222 consecutive patients
rcises, and skin care,2009–January
( January as Table 1.
2017; median age: 45.8 years) with lymphedema affecting the entire
nternational consensus guidelines.18 Characteristics of the 222 Patients at Inclusiona
lower limb,
e was conducted who received complete decongestive physical therapy for the first time in a
by a physical
Characteristic Value
specialized
lymphatic lymphedema
techniques who also management center.
multilayer-bandaging technique and
Downloaded from https://academic.oup.com/ptj/article-abstract/100/5
Age, y 45.8 [32–60.4]
h session lasted 30 minutes, and BMI, kg/m2
Methods. Complete
was covered with foam (N/N) or decongestive
40 kg/m
and breathing 2 , and previous
exercises, Right side cellulitis, as independently 105 (47.3) associated with lymphedema
andages in place to enhance Volume, mL 2003 [1038–3487]
volume reduction.
eripheral to central compartments.
For each additional year of age, volume reduction increased 0.16%.
Excess volume, % 32.4 [16.2–51]
Unexpectedly,
muscle groups: log-transformed
each articulation of initial lymphedema volumes indicated a negative impact,
≥1 past cellulitis episode(s) 91 (41)
that is,
ck (smoothly raise4.95%,
shoulders for each log-unit gain. Patients with previous cellulitis episode(s) obtained
them back down, and forward in a a
Results are expressed2 as n (%) or median [interquartile range], unless stated
6.9% and those with
otion; flex elbows without and with BMI >40 kg/m
otherwise. BMI = body 17.1%
mass index.higher lymphedema volume reductions. Lower
limb
aw elbows lymphoscintigraphy
back squeezing the was available for 150 (67.6%) patients. Having dermal back flow
er; form a fist, then slowly andcom/ptj/article-abstract/100/5/766/5707306 by bibliotheque interuniversitaire de medecin
Lymphoscintigraphie MI
ower limb lymphedema treated for the first time with complete decongestive therapy.
rds the ankle (below
nee). Lymphedema
) was calculated for
truncated cone, also
+ Cc + c2 )/12π ,
erence of the top of
e base of the cone.15
has demonstrated
oducibility
hich remains the
were measured at
congestive physical
ed as the difference
olume (LLV ) and the
pressed as the
HLV ] × 100].
nd after the intensive Figure 2.
Lower limb lymphoscintigraphy: (A) normal; (B) left unilateral pri-
therapist.
mary lymphedema with diminished inguinal lymph-node uptake
(triangle); (C) right unilateral primary lymphedema with complete
absence of inguinal lymph-node uptake; (D) left unilateral primary
al, but lymphedema with dermal backflow in the calf (asterisk) and con-
on of the diagnosis. tralateral popliteal node visualization (arrow).
s always done in theRésultats (1)
Predictors of Primary Lymphedema-Volume Reduction
Table 2.
Multivariate Analysis of Predictors of Lymphedema Volume Reduction After Complete Decongestive Physical Therapya
Parameter Estimate Standard Error T P
Downloaded from https://academic.oup.com/ptj/article-abstract/100/5/766/
Age, per year gain 0.16 0.07 2.09 .038
2
BMI >40 kg/m 17.1 6.68 2.57 .01
Past cellulitis 6.9 2.85 2.41 .017
b
Log initial lymphedema volume, per log-unit gain –4.95 1.50 −3.30 .001
a
BMI = body mass index.
b
To meet the basic assumptions of the linear regression, log-transformation was applied.
Table 3.
Lymphoscintigraphic Characteristics of the 150 Patients Tested
Characteristic Lymphedematous Limb Normal Limb P
Inguinal lymph node uptake
Normal, n (%) 8 (5.3) 142 (94.7)aded from https://academic.oup.com/ptj/article-abstract/100/5/766/5707306 by bibliotheque interuniversitaire de medecine use
Past cellulitis 6.9 2.85 2.41 .017
b
Log initial lymphedema volume, per log-unit gain –4.95 1.50 −3.30 .001
a
BMI = body mass index.
Résultats (2)
b
To meet the basic assumptions of the linear regression, log-transformation was applied.
Table 3.
Lymphoscintigraphic Characteristics of the 150 Patients Tested
Characteristic Lymphedematous Limb Normal Limb P
Inguinal lymph node uptake
Normal, n (%) 8 (5.3) 142 (94.7) 40 kg/m2 as independentlyConclusions (1)
1. Facteurs cliniques associés à
une perte de volume
– IMC > 40
– ↑ âge
– antécédents d’érysipèle
– + le volume initial ↑ - le
traitement est efficaceConclusions (2)
2. Facteurs scintigraphiques
– utile au Dg
– utile car prédictifs de la
réponse au traitement
dermal backflow, logique
car reflux sous-dermique
accessible au traitementMAV CÉRÉBRALES
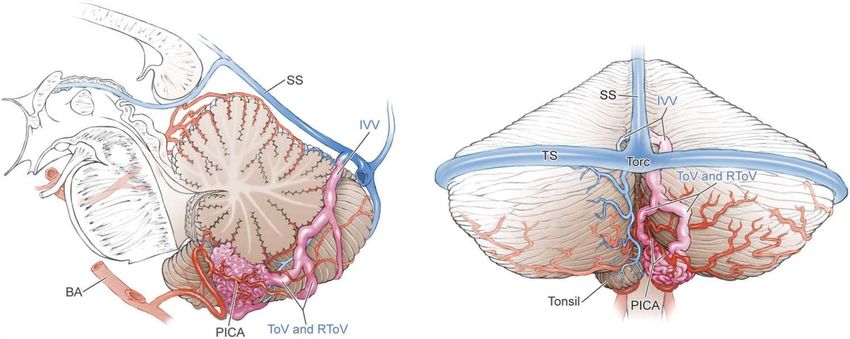
Presence of direct vertebrobasilar perforator feeders in posterior fossa arteriovenous
malformations and association with poor outcomes after endovascular treatment
Etienne Lefevre, Thomas Robert, Simon Escalard, Robert Fahed, Stanislas Smajda,
Gabriele Ciccio, Jean-Philippe Desilles, Mikael Mazighi , Raphaël Blanc, Michel Piotin
MAV et fistule durale médullaires concomittantes: une forme méconnue de lésions
multiples
Alexis Guédon, Stéphanie Condette-Auliac, Arturo Consoli, Federico Di Maria, Oguzhan
Coskun, Georges Rodesch
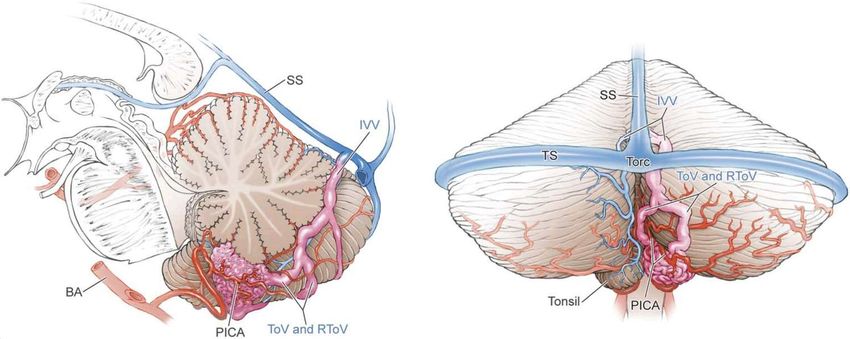
Concomitant conus medullaris arteriovenous shunts and sacral dural arteriovenous
fistulas: pathophysiological links related to the venous drainage of the lesions in a series
of five cases
Andrea Rosi, Arturo Consoli, Stéphanie Condette-Auliac, Oguzhan Coskun, Federico Di
Maria, Georges Rodesch
50La présence d’afférences vertebro-basilaires directes dans les malformations artério-veineuses de fosse postérieure (PFAVMs) est prédictif de détérioration neurologique et de faible taux d’occlusion après un traitement endovasculaire. E T I E N N E L E F E V R E ; T H O MA S R O B E R T ; S I MO N E S C A L A R D ; R O B E R T F A H E D ; R A P H A Ë L B L A N C ; MI C H E L PIOTIN
Conflit d’intérêt o Aucun conflit d’intérêt avec cette présentation.
Grading system for arteriovenous malformations
Size of the A VM. The size of the AVM is deter-
mined by measuring on angiograms the largest diameter
of the nidus o f the malformation. When magnified
Introduction
angiographic views are considered, a correction for the4. Carotid angiograms, lateral view (left) and antero-
FIG.
magnification factor is required. The size of theformation posterior
AVM view (right), showing a Grade II arteriovenous mal-
FIG. 2. Carotid angiograms, lateral view (left) and antero- (AVM). The AVM is less than 3 cm (small: 1
is determined
posterior view (right), showingto be smallI arteriovenous
a Grade (< 3 cm), medium
mal- (3 to 6located in the dominant hemisphere adjacent to the
point),
formation cm),
(AVM). or This
largeAVM
(> 6iscm), and 3the
less than cm AVM is scoredreceptive
in diameter appro- language area (Wernicke's area) (eloquent: 1 point),
(small: 1 point),
priately.located in the anterior frontal lobe (non- and has exclusively superficial venous drainage (arrow) (su-
eloquent: 0 points), and drains through cortical veins (arrows) perficial drainage: 0 points).
The size
(superficial drainage: of the malformation is responsible for much
0 points).
of the technical difficulty in removing AVM's. The
larger an AVM, the larger the a m o u n t of normal adja-
cent neural tissue that is exposed to injury during
categories (Table 1). The grade o f the lesion is derived
microsurgicalTABLE resection
1 o f the nidus. Large AVM's
by s u m m i n g the points assigned for each category. The
mandate
Determination longer operating
of arteriovenous malformationtime, thereby
(A VM) grade*increasing the
lowest grade possible is G r a d e I; such a lesion would be
risk of anesthesia-related complications. Furthermore, small (1 point), located in a n o n - e l o q u e n t region such
Graded
the Feature of size encompasses
criterion Points Assigned
several of theas other
the anterior frontal lobe (0 points), a n d have exclu-
important
size of AVM factors that determine the degree of surgical sively superficial drainage (0 points) (Figs. 2 and 3).
small (< 3 cm)In general the size of an1 AVM determines,
difficulty. Complete surgical excision o f such an A V M would
medium (3-6 cm) 2
or is closely
large (> 6 cm) related to, the number 3 of feeding arteries,
present relatively m i n o r technical difficulties and would
the amount
eloquence of flow,
of adjacent brain and the degree of steal. entail very little risk o f resultant m o r b i d i t y or mortality.
non-eloquent 0
Pattern of Venous Drainage. 1The course The
eloquent of thehighest grade within this scheme is G r a d e V; an
A V M o f this type would be larger t h a n 6 c m (3 points),
draining
pattern veins
of venous is determined from the angiogram. The
drainage
superficialpattern
only 0 located within or immediately adjacent to eloquent
venous is considered superficial if all thebrain
drain-(1 point), and a portion o f the drainage would
deep 1
age from the AVM is through the cortical venous e m psys-
t y into the deep venous system (1 point) (Figs. 7
* Grade = [size] + [eloquence] + [venous drainage]; that is (1, 2,
tem. The venous
or 3) + (0 or 1) + (0 or 1).
pattern is considered deep if any or
all of the drainage is through deep veins (such as
internal cerebral veins, basal veins, or precentral cere-
Spetzler RF,bellar
Martinvein).
NA. In the posterior
A proposed fossa,
grading only cerebellar
system hemi-
for arteriovenous
spheric
malformations. veins that 1986;65(4):476-483
J Neurosurg. drain directly into the straight sinus
or transverse sinus are considered to be superficial veins.
Clearly, the pattern o f venous drainage is closely
related to the surgical accessibility of an AVM. Deep
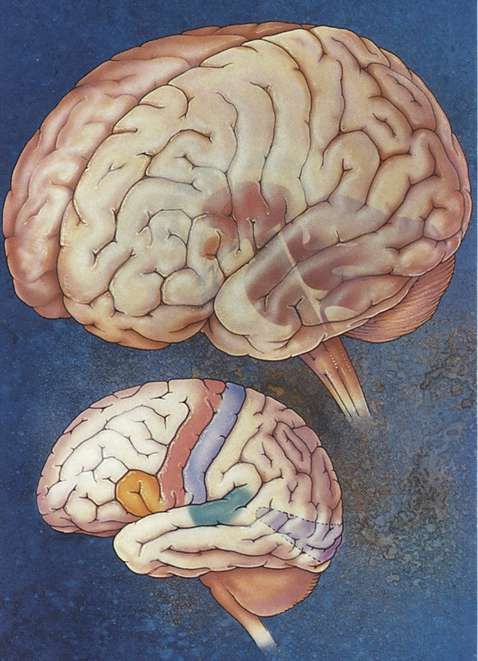
venous drainage, no matter how small, further compli- FIG. 1. The anatomic areas considered neurologically el-
cates AVM excision. Often the vast majority of an oquent for the purposes of the grading system are indicated.
The deep eloquent areas (hypothalamus, thalamus, brain
AVM will have been separated from the surrounding stem, and cerebellar peduncles) are highlighted in the upper
brain when the small arterialized subependymal veins image. The eloquent regions of the cerebral cortex (sensori-
of the deep component are encountered. These veins motor areas, language areas, and primary visual area) are
identified on the lower image.Contexte : PFAVMs
o Risque hémorragique plus élevé
o Hémorragies plus graves
o Traitement dangereux et controversé
o Objectifs :
o Evaluer les effets du traitement endovasculaire des PFAVMs
o Identifier les sous-groupes qui semblent bénéficier du traitementMéthodes o Etude Monocentrique Rétrospective o Relecture des angiographies o Caractéristiques angio-architecturales o Détérioration neurologique : mRS shift > 0 o Echec de traitement : occlusion incomplète
Résultats
Résultats (2)
Angioarchitecture Completely obliterated Not completely obliterated UNAJUSTED (OR) P
Location :
- Eloquent areas 26 (57.8%) 19 (42.2%)
Résultats (3)
2.42 (1.04-5.80) 0.04
- Non-eloquent areas 43 (76.8%) 13 (23.2%)
Arterial feeders
- Vertebral & basilar direct perforators feeders 1 (12.5%) 6 (87.5%)
15.69 (2.52-304.03) 0.01
- Absence of Vertebral or Basilar direct perforators
68 (72.3%) 26 (27.7%)
feeders
- ≤ 2 arterial feeders 46 (75.4%) 15 (24.6%)
2.27 (0.97-5.40) NS
- > 2 arterial feeders 23 (57.5%) 17 (42.5%)
• Facteurs prédictifs d’un Venous drainage
- Deep 33 (56.9%) 25 (43.1%)
faible taux d’occlusion
3.85 (1.56-11.1) 0.006
- Superficial 36 (83.7%) 7 (17.3%)
angiographique après
- Single 40 (76.9%) 12 (23.1%)
2.30 (0.98-5.56) NS
- Multiple 29 (59.2%) 20 (40.8%)
traitement Size
- < 3 cm 54 (75%) 18 (25%)
endovasculaire
2.78 (1.14-7.14) 0.025
- 3-6 cm 15 (51.7%) 14 (48.3%)
Associated aneurysms
- Prenidal 22 (75.9%) 7 (24.1%) 0.60 (0.21-1.54) NS
- Intranidal 13 (72.2%) 5 (27.8%) 0.80 (0.24-2.38) NS
Spetzler & Martin (SM) grade
- Low SM grade (1 & 2) 49 (83%) 10 (17%)
5.39 (2.22-13.89) 0.0003
- High SM grade (3 & 4) 20 (47.6%) 22 (52.4%)Angioarchitecture Completely obliterated Not completely obliterated UNAJUSTED (OR) P
Location :
- Eloquent areas 26 (57.8%) 19 (42.2%)
Résultats (3)
2.42 (1.04-5.80) 0.04
- Non-eloquent areas 43 (76.8%) 13 (23.2%)
Arterial feeders
- Vertebral & basilar direct perforators feeders 1 (12.5%) 6 (87.5%)
15.69 (2.52-304.03) 0.01
- Absence of Vertebral or Basilar direct perforators
68 (72.3%) 26 (27.7%)
feeders
- ≤ 2 arterial feeders 46 (75.4%) 15 (24.6%)
2.27 (0.97-5.40) NS
- > 2 arterial feeders 23 (57.5%) 17 (42.5%)
• Facteurs prédictifs d’un Venous drainage
- Deep 33 (56.9%) 25 (43.1%)
faible taux d’occlusion
3.85 (1.56-11.1) 0.006
- Superficial 36 (83.7%) 7 (17.3%)
angiographique après
- Single 40 (76.9%) 12 (23.1%)
2.30 (0.98-5.56) NS
- Multiple 29 (59.2%) 20 (40.8%)
traitement Size
- < 3 cm 54 (75%) 18 (25%)
endovasculaire
2.78 (1.14-7.14) 0.025
- 3-6 cm 15 (51.7%) 14 (48.3%)
Associated aneurysms
- Prenidal 22 (75.9%) 7 (24.1%) 0.60 (0.21-1.54) NS
- Intranidal 13 (72.2%) 5 (27.8%) 0.80 (0.24-2.38) NS
Spetzler & Martin (SM) grade
- Low SM grade (1 & 2) 49 (83%) 10 (17%)
5.39 (2.22-13.89) 0.0003
- High SM grade (3 & 4) 20 (47.6%) 22 (52.4%)Good neurological outcome Bad neurological outcome after
Angioarchitecture OR p
after treatment treatment
Location :
- Eloquent areas 31 (68.9%) 14 (31.1%)
2.71 (1.04-7.50) 0.05
Résultats (4)
- Non-eloquent areas 48 (85.7%) 8 (14.3%)
Arterial feeders
- Vertebral & basilar direct perforators
3 (42.9%) 4 (57.1%)
feeders
5.63 (1.15-30.76) 0.03
- Absence of Vertebral or Basilar direct
76 (80.9%) 18 (19.1%)
perforators feeders
- ≤ 2 arterial feeders 48 (78.7%) 13 (21.3%)
1.07 (0.39-2.79) NS
- > 2 arterial feeders 31 (77.5%) 9 (22.5%)
Venous drainage
• Facteurs prédictifs de - Deep 42 (72.4%) 16 (27.6%)
2.35 (0.87-7.12) NS
détérioration
- Superficial 37 (86%) 6 (14%)
- Single 43 (82.7%) 9 (17.3%)
1.73 (0.67-4.63) NS
neurologique après
- Multiple 36 (73.5%) 13 (26.5%)
Size
traitement -
-
< 3 cm
3-6 cm
57 (79.2%)
22 (75.9%)
15 (20.8%)
7 (24.1%)
1.21 (0.41-3.29) NS
endovasculaire Associated aneurysms
- Prenidal 23 (79.3%) 6 (20.7%) 0.91 (0.30-2.53) NS
- Intranidal 14 (77.8%) 4 (22.2%) 1.03 (0.27-3.30) NS
Spetzler & Martin (SM) grade
- Low SM grade (1 & 2) 50 (84.7%) 9 (15.3%)
2.49 (0.96-6.73) NS
- High SM grade (3 & 4) 29 (69%) 13 (31%)Good neurological outcome Bad neurological outcome after
Angioarchitecture OR p
after treatment treatment
Location :
- Eloquent areas 31 (68.9%) 14 (31.1%)
2.71 (1.04-7.50) 0.05
Résultats (4)
- Non-eloquent areas 48 (85.7%) 8 (14.3%)
Arterial feeders
- Vertebral & basilar direct perforators
3 (42.9%) 4 (57.1%)
feeders
5.63 (1.15-30.76) 0.03
- Absence of Vertebral or Basilar direct
76 (80.9%) 18 (19.1%)
perforators feeders
- ≤ 2 arterial feeders 48 (78.7%) 13 (21.3%)
1.07 (0.39-2.79) NS
- > 2 arterial feeders 31 (77.5%) 9 (22.5%)
Venous drainage
• Facteurs prédictifs de - Deep 42 (72.4%) 16 (27.6%)
2.35 (0.87-7.12) NS
détérioration
- Superficial 37 (86%) 6 (14%)
- Single 43 (82.7%) 9 (17.3%)
1.73 (0.67-4.63) NS
neurologique après
- Multiple 36 (73.5%) 13 (26.5%)
Size
traitement -
-
< 3 cm
3-6 cm
57 (79.2%)
22 (75.9%)
15 (20.8%)
7 (24.1%)
1.21 (0.41-3.29) NS
endovasculaire Associated aneurysms
- Prenidal 23 (79.3%) 6 (20.7%) 0.91 (0.30-2.53) NS
- Intranidal 14 (77.8%) 4 (22.2%) 1.03 (0.27-3.30) NS
Spetzler & Martin (SM) grade
- Low SM grade (1 & 2) 50 (84.7%) 9 (15.3%)
2.49 (0.96-6.73) NS
- High SM grade (3 & 4) 29 (69%) 13 (31%)Conclusion o Confirmation de la classification de Spetzler & Martin et applicabilité aux PFAVMs traitées en endovasculaire o Première description d’un critère prédictif d’échec du traitement endovasculaire des PFAVMs (présence d’afférence vertebro-basilaire directe)
Merci de votre attention…
Article(s) « de l’année »
CRMR constitutif AVANCE MAVs médullaires adultes et enfants (FOR)
Hôpital Foch
FAVA-Multi
Concomitant conus medullaris arteriovenous shunts and sacral dural arteriovenous fistulas:
Pathophysiological links related to the venous drainage of the lesions in a series of five cases
Rosi A, Consoli A, Condette-Auliac S, Coskun O, Di Maria F, Rodesch G
J Neurointerv Surg, 2018
Primary conus medullaris arteriovenous shunt and secondary lumbo-sacral epidural
arteriovenous fistula: one malformation can hide another
Guedon A, Condette-Auliac S, Consoli A, Di Maria F, Coskun O, Rodesch G
J Neuroradiol 20196 patients
MAVs cône terminal
Association fistules durales
lombo-sacrées
2018
F 23 ans
2011 steppage Aggravation depuis 1 an
tr sensitifs MIG Paraparésie
dls lombaires Tr sphinctériens
IRM suspicion MAV Méd
2012 Foch
4 sessions E° /18 mois
Régression symptômes
amélioration clinique
(spasticité MIG +/-)
Décision de suivi…
Mais pas de recontactMAVs médullaires multiples rares
Habituellement génétiques non héréditaires (métamériques)
Fistules durales lombo-sacrées rares (4% localisations habituelles). Homme >50 ans
6 cas: patients jeunes (3 H / 3F)
lien entre MAVs cône et fistules durales par l’intermédiaire veine de draînage
Susceptibilité personnelle du patient? Histologie?
Sac dural plus fin dans la région lombo sacrée. Plus grand nombre de veines radiculaires fibrotiques.
Biologie? DM et veines lombosacrées plus susceptibles à cascade PP HTV->angiogenèse
Fistules durales sont acquises, créées par angiogenèse induite par thrombose et hypertension veineuse, avec
élargissement de microshunts artérioveineux physiologiques
Importance d’un suivi clinique et radiologique précis.
IRM et ARM pour le suivi et en cas de modification de symptomatologieVous pouvez aussi lire