ALCAPA Prise en charge de l'anomalie de naissance de la coronaire gauche - Abnormal Left Coronary Artery into Pulmonary Artery Dr Daniela Laux ...
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous
Prise en charge de l’anomalie de
naissance de la coronaire gauche
Le point de vue du cardiopédiatre
ALCAPA
Abnormal Left Coronary Artery into Pulmonary Artery
Dr Daniela Laux
UE3C-Paris et M3C-CCML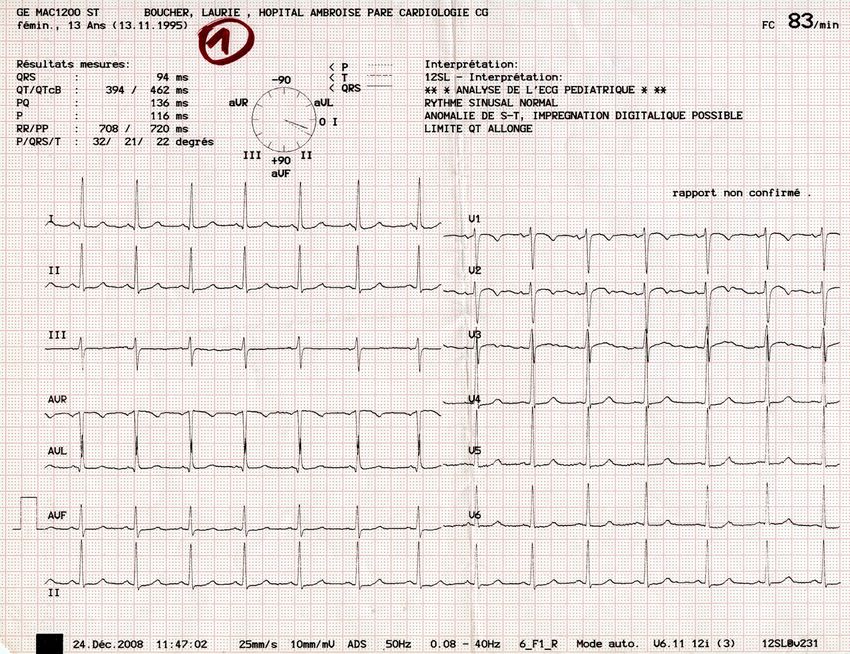
Repères chronologiques
Formation valves
Bourgeons endocardiques
semilunaires
Entonnoir tricuspidien
Délamination valve
Elongation voie éjection
tricuspide
Arcs Ao 4et 6
Wedging
Croissant Convergence
cardiaque Septation
cardiaque
LOOP
J18 J23 30 40 42 44 50
Corne D du sinus veineux
Connexion coronaires - aorte
Apparition VP 1°
Arcs Ao 2 et 3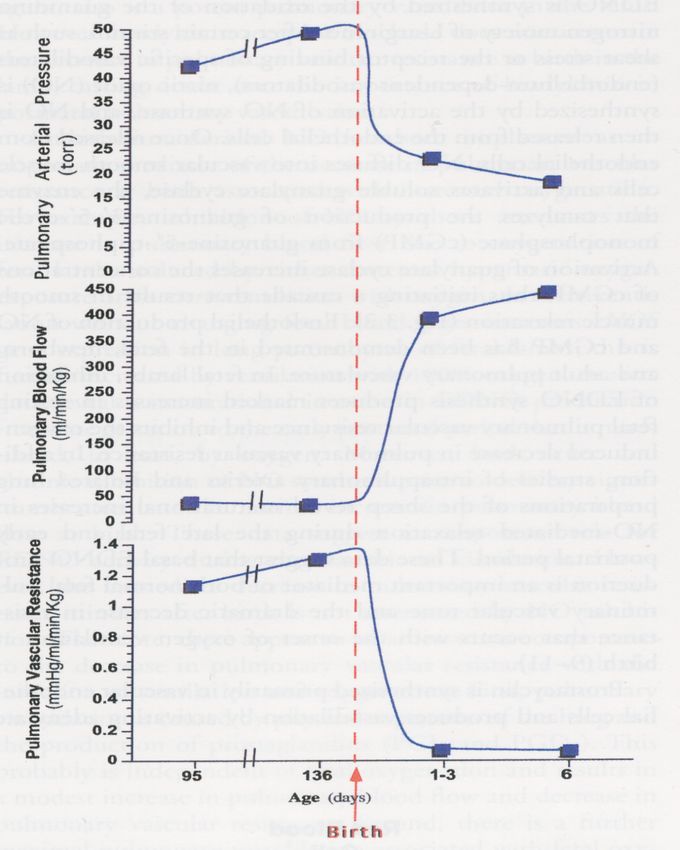
Embryologie
Les artères coronaires ne naissent pas de l’aorte (notion
ancienne de bourgeons coronaires)
…mais se connectent à l’aorte
Bogers AJJC. Anat Embryol 1989
Origine: proépicarde ou pôle veineux?
Wada AM et al. Arterioscler Thromb Vasc Biol 2003 Red-Horse K et al. Nature 2010
PEO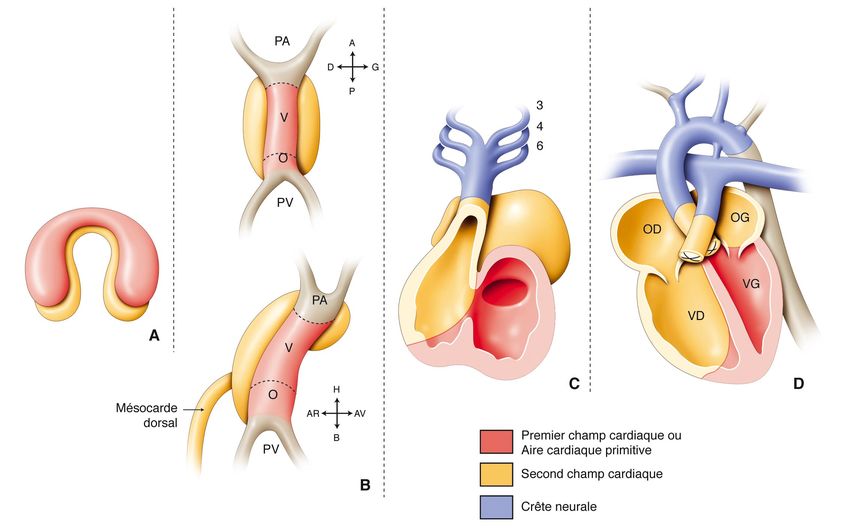
Développement des coronaires
Migration de Formation de Transformat° Formation des Développement
l’OPE l ’épicarde mésenchymateuse plexus des artères
capillaires coronaires
OPE
COEUR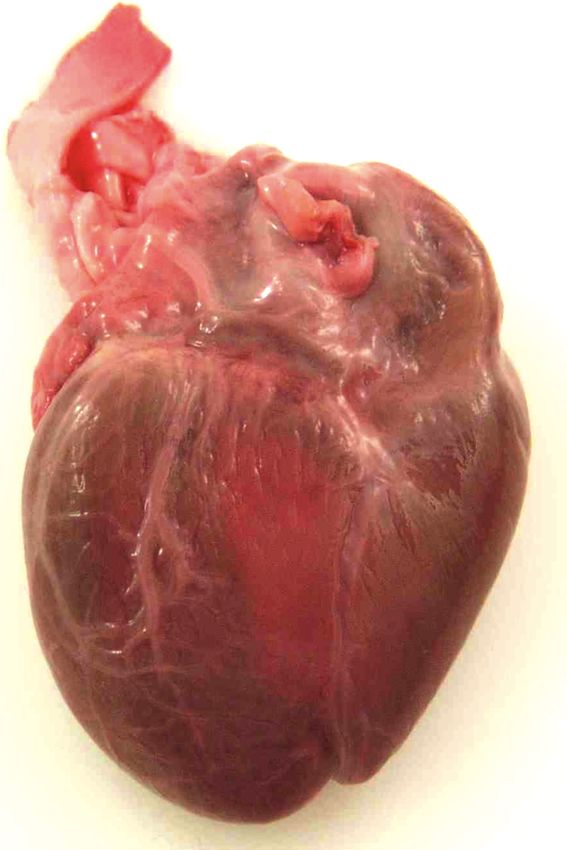
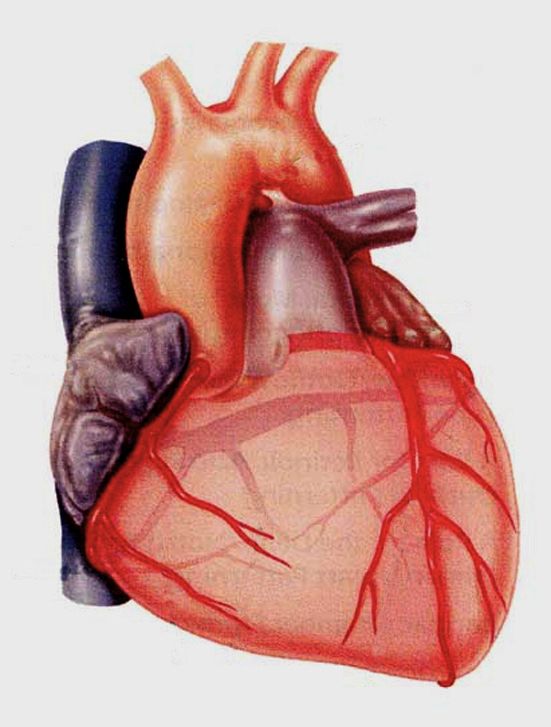
Formation des coronaires
Tronc commun
circonflexe
Coronaire
droite
Inter-ventriculaire
antérieure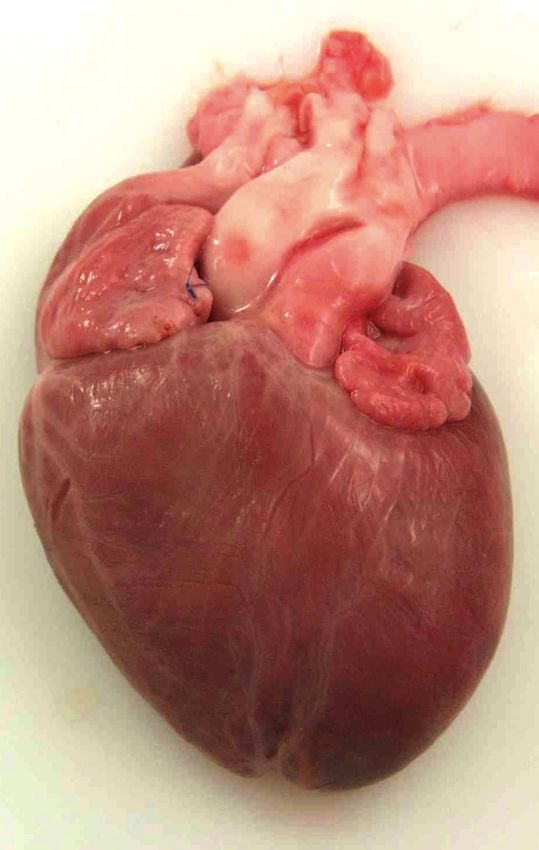
ALCAPA – anatomie et incidence • 1/300 000 naissance vivantes • 0,25-0,5% des cardiopathies congénitales Cowles et al. 2007
O RI GIN AL ARTI CL E
Anomalous Left Coronary Artery Connected to the Pulmonary
Artery Associated WithAuthor's
Other Cardiac Defects:
personal copy A Difficult Joint
Diagnosis Laux
et
al.
2014
Ped
Cardiol
Pediatr Cardiol
Daniela Laux • Claire Bertail • Fanny Bajolle •
Table 1 Overview of all the anatomic cardiac and extracardiac features of anomalous left coronary artery connected to the pulmonary artery
Lucile Houyel
(ALCAPA) • Younes Boudjemline •
and the associated cardiovascular defects
Damien Bonnet
Case LCA anomaly Associated congenital heart disease Extracardiac anomalies
1 ALCAPA Aortic coarctation Coloboma, external genital
anomaly
Received: 7 December 2013 / Accepted: 25 April 2014
2 ICAPA Aortic coarctation, hypoplastic horizontal aortic arch, muscular VSD
! Springer Science+Business Media New York 2014
3 ALCAPA/RPA Aortic coarctation, tubular hypoplastic aortic arch, malaligned VSD
4 ALCAPA/RPA Aortic coarctation, muscular VSDs, ASD ostium secundum type
5 Abstract
ALCAPAAnomalous left
Aortic coronarybicuspid
coarctation, artery aortic
connected
valve to that ALCAPA associated with other cardiac defects often is
6 the ALCAPA
pulmonary artery ToF(ALCAPA) can be associated rarely misdiagnosed before surgery, mostly Goldenhar due to specific
syndrome
7 withALCAPA
other congenital heart
ToF, defects. The
dextrocardia, preoperative
scimitar syndrome joint hemodynamics masking myocardial Severeischemia
right lungpreopera-
hypoplasia
diagnosis is challenging. From 1987 to 2012,
Right aberrant subclavian arterya retrospec- tively. Survival was compromised due to the unrecognized
Cleft palate, facial dysmorphia
8 tive bicentric
ALCAPA assessment of 12 patients with ALCAPA diagnosis
ToF with pulmonary atresia, aberrant right subclavian artery of an associated coronary abnormality but also
related to other cardiac defects
Persisting left focused on the
superior caval veinassociated because of midterm complications related to the other
to coronary sinus
9 heartALCAPA
defect, the moment
Dividedofleft
complete diagnosis
atrium, partial related
anomalous to
pulmonarycardiac
venousdefects.
return of entire right lung
surgery, and outcome. Coarctation was the most frequently
Stenosis of both left pulmonary veins
10
associated
ALCAPA
heart defect (n = 5) followed by tetralogy of
Right aortic arch
Keywords Anomalous left coronary artery connected to
11
Fallot with or without
ALCAPA
pulmonary atresia (n = 3). The
Congenital mitral valve insufficiency
the pulmonary artery ! ALCAPA ! Aortic coarctation !
study group comprised one case of hypoplastic left heart Tetralogy of Fallot ! Congenital heart disease ! Cardiac
Prolapse of anterior mitral valve leaflet and hypoplastic posterior leaflet
12
syndrome,
ICAPA
one right aortic arch, one congenital mitral
HLHS with aortic atresia and mitral atresia
defect
malformation, and one infant with divided left atrium and
LCA left coronarypulmonary
anomalous artery, ICAPA infundibular
venous return.coronary artery patients
Only four branch connected to the pulmonary artery, VSD ventricular septal defect, RPA right
pulmonary artery, ToF tetralogy of Fallot, ASD atrial septal defect, HLHS hypoplastic left heart syndrome
had a complete diagnosis of both the cardiac defect and the Introduction
coronary abnormality before surgery. In two cases, the
coronary anomaly was discovered during surgery per- Anomalous left coronary artery connected to the pulmon-
formed for another cardiac defect and treated at the same ary artery (ALCAPA) is a congenital coronary anomaly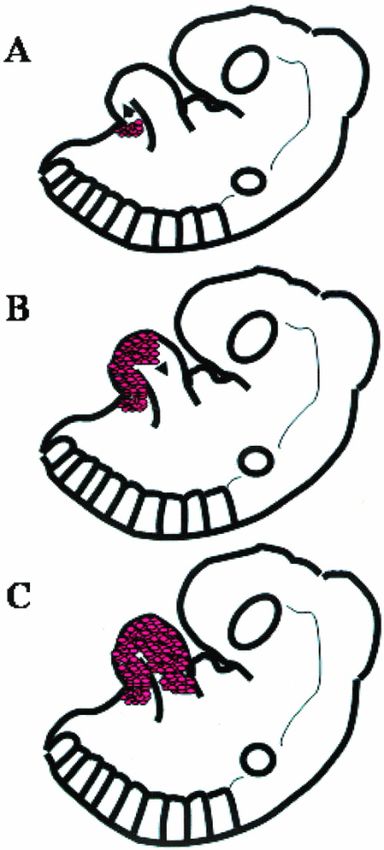
Physiopathologie
• Perfusion anténatale assurée (Re et O2 identiques dans Ao et AP)
• Perfusion postnatale coronaire maintenue pendant quelques
semaines en raison des résistances pulmonaires encore un peu
élevées (mais baisse de la saturation en O2)
• Défaut de perfusion coronaire après quelques semaines (RVP très
basses) entrainant un « infarctus » antéro-latéral
• Développement d’une circulation collatérale à contre-courant avec
revascularisation de la coronaire gauche par la coronaire droite
Diagnostic des formes classiques
• Période de latence de quelques semaines à quelques
mois
• Tableau d’insuffisance cardiaque variable
• Consultation aux urgences
– Difficultés alimentaires, polypnée, sueurs
– Collapsus
– Syncope
– Douleur angineuse parfois retrouvée à
l’interrogatoire (cri et pâleur aux biberons)
– Galop, souffle d’IM
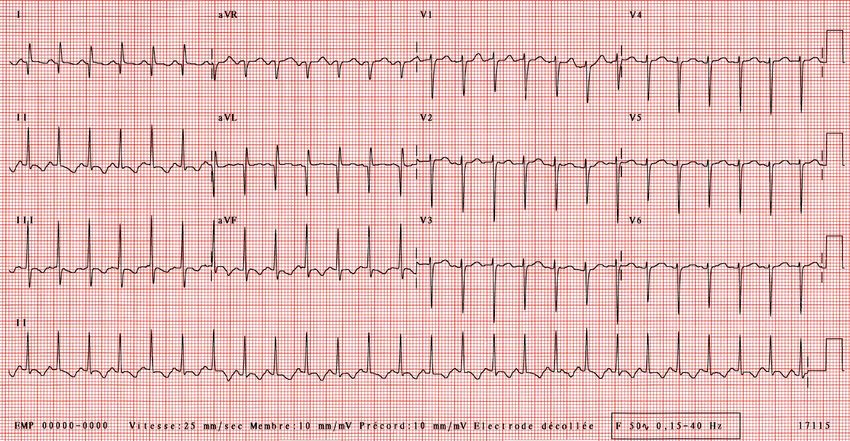
– Troponine: peut être normale!!Face à une cardiomégalie: toujours faire un ECG
Onde Q large et profonde de nécrose en D1, AVL Rabotage de l’onde R dans toutes les précordiales Troubles de la repolarisation dans les précordiales Attention au BBG masquant les ondes Q à gauche
Echocardiographie • Cardiomyopathie dilatée à parois minces et brillantes • Fraction de raccourcissement effondrée, le plus souvent, avec VG dilaté (mesurer la taille du VGTD plutôt que FR) • Paroi antéro-septale fine et brillante • Piliers de la valve mitral brillants • Insuffisance mitrale par ischémie des piliers • Vision difficile de l’artère coronaire gauche dans l’AP avec flux diastolique ascendant dans l’AP • Dilatation de la coronaire droite++++ (très bon signe) • Si diagnostic difficile: scanner coronaire • Anomalie associée: CoA, CIV, fenêtre aorto- pulmonaire
Echographie
Echographie
Echographie
Diagnostic différentiel devant une
cardiomyopathie dilatée hypokinétique
sans ALCAPA
– Obstacles gauches
• CoA (pouls, gradient tensionnel)
• Sténose Aortique (auscultation SS, échographie)
– Atrésie ou sténose de l’ostium gauche (aortographie
non selective)
– Myocardite (HDLM, tropo, IRM)
– CMD rythmique (ECG, holter)
– CMD métabolique (ATCD perso et familiaux, bilan
métabolique)
– CMD toxique (interrogatoire)
– CMD sans causeTraitement – Insuffisance cardiaque aigue • Diurétiques, IEC • Soutien nutrionnel • Ventilation non invasive ou invasive si besoin • Amines ssi nécessaire – Rapidement, il faut appeler le chirurgien
Evolution – Décès en absence de diagnostic ou possible récupération (forme de l’enfance, adolescence ou adulte) – Evolution après la chirurgie • Reprise pondérale • Normalisation de l’ECG (repousse des ondes R et disparition onde Q) • Récupération de la fonction VG en un an, le plus souvent • Régression possible de l’IM • IM résiduelle par ischémie des piliers avec prolapsus • Plastie mitrale parfois nécessaire • Cardiomyopathie dilatée séquellaire… – Traitement de l’insuffisance cardiaque chronique après la sortie • Nutrition +++++ (NEDC si besoin), fer et foldine • IEC, Aldactone, Béta-bloquant • Synagis de septembre à mars si moins de un an
Suivi -Scanner coronaire à un an pour contrôle systématique - Plus tôt si aucune récupération ou aggravation… - Coronarographie si besoin (attention si sténose)
pulmonary artery repair: a 40-year single-centre experience. Eur J Cardiothorac Surg 2017; doi:10.1093/ejcts/ezx407.
Time point Preoperative Postoperative Discharge
CONGENITA
MI, grade, n (%)
0 7 (9) 19 (24) 22 (32)
Long-term outcome after anomalous left coronary artery from the
1 24 (31) 33 (42) 30 (43)
2 27 (35) 16 (21) 10 (14)
3 13 (17) 8 (10) 5 (7)
pulmonary artery repair: a 40-year single-centre experience 4
LVESD (mm), median (range)
LVEDD (mm), median (range)
7 (8)
33 (19–48)
37 (22–68)
2 (3)
32 (16–44)
37 (25–58)
3 (4)
25 (13–41)
33 (17–61)
Rüdiger Langea,b, Julie Cleuzioua, Markus Kranea,bALCAPA: , Peter Ewert
anomalous
c
, Jelena
left coronary Pabst
artery from von Ohain
the pulmonary
a
, left ventricle end-diastolic dimension; LVESD: left ve
artery; LVEDD:
sion; MI: mitral valve insufficiency.
R. Lange et al. / European Journal a of Cardio-Thoracic Surgery
a,(adult type). ALCAPA: anomalous 5
Figure 2: (A) ALCAPA patient without coronary collateralization Elisabeth Beran
(infant type) and (B) and Ketiin an
coronary collateralization Vitanova
ALCAPA patient *
left coronary artery from the pulmonary artery; RCA: right coronary artery.
N
=
78
a
1977-‐2015
Department of Cardiovascular Surgery, German Heart Centre Munich, Technische Universität München, Munich, Germany
b Table 2: EF in 52 patients (Group A) and 26 patients (Group B) at different time points following ALCAPA repair
German Heart Center Munich–DZHK Partner Site Munich Heart Alliance, Munich, Germany
c
Department of Pediatric Cardiology and Congenital Heart Disease, German Heart Centre Munich, Technische Universität München, Munich, Germany
CONGENITAL
Time point Preoperative, n (%) Postoperative, n (%) Discharge, n (%) Final follow-up, n (%)
* Corresponding author. Department of Cardiovascular Surgery, German Heart Centre Munich, Lazarettstrasse 36, 80636 Munich, Germany. Tel: +49-89-12182962;
Group
fax: A (ne-mail:
+49-89-12184123; = 52) vitanova@dhm.mhn.de
B (n = 26) (K.AVitanova).
(n = 52) B (n = 26) A (n = 44) B (n = 26) A (n = 44) B (n = 24)
EF (%)
Received 6 July 2017; received in revised form 9 October 2017; accepted 23 October 2017
50
Abstract 7 (13) 6 (23) 24 (46) 14 (54) 31 (70) 14 (54) 37 (84) 18 (75)
P-value 0.06 0.4 0.3 0.3
OBJECTIVES: An anomalous left coronary artery from the pulmonary artery (ALCAPA) is a rare congenital anomaly, often associated with
severely
ALCAPA:impaired left
anomalous leftventricular (LV)from
coronary artery contractility andartery;
the pulmonary functional mitral
EF: ejection valve (MV) regurgitation. Current data suggest that earlier correc-
fraction.
tion of ALCAPA may result in a more complete recovery of LV function. By analysing the results of a large single-centre ALCAPA cohort, we
sought to investigate whether these treatment paradigms remain valid.
Figure 3: (A) Freedom from cardiac death in 78 anomalous left coronary artery from the pulmonary artery patients and (B) freedom from cardiac death in 37 anoma-
METHODS: A retrospective
lous left coronary study was
artery from the pulmonary artery performed evaluating
patients who underwent repair after patientsFigure
all1995. valve
5: (A) Mitral valve insufficiency in patients with anomalous left coronary artery from the pulmonary artery at different time poi
undergoing repair
insufficiency (Grade 2 or of ALCAPA
more) overlefta coronary
after anomalous periodartery
of almost 40 years.
from the pulmonary All
artery repair. *statistical significance. 1
preoperative and postoperative echocardiographic reports were reviewed, focusing
3: at the on the
time of hospital recovery
discharge; of follow-up;
4: at the final LV andMI: MV function.
mitral valve insufficiency.
Downloaded from https://academic.oup.com/ejcts/advance-article-abstract/doi/10.1093/ejcts/ezx407/4652928
by Technische Universitaet Muenchen user
RESULTS: The study cohort included 78 patients who underwent ALCAPA repair
on 18 December 2017 between
has evolved 1977and
repair
over time and
the2015, who were
translocation divided
technique has intoLV 2 groups
damage due to myocardial isc
based on patient age at initial repair: Group A (n = 52, age 1 year).
modern Following
procedure for mostrepair,
patients.systolic
In LV andisMV
ALCAPA associated with a range of p
cases of an exceptional distance of the left coronary ostium from as endocardial and subendocardial
function improved significantly (P < 0.01) in both groups. Patient age at the time of initial surgery had no significant influence on the
the aorta, the transpulmonary baffling (Takeuchi) procedure is a muscles, myocardial necrosis and vent
improvement of LV function. Early mortality (within 30 days) was 10%valid (n =alternative.
8). No 30-day mortality
This study showed thatwastoreported in the past
date, long-term 20 years. MV incompetence dev
consequence,
Survival at 20 years following ALCAPA repair was 86 ± 4%. results after initial repair are excellent. In our study, overall sur- cases [23]. In our study, 65% of patients
vival at 10 and 20 years was 86 ± 4%. No early deaths occurred function and 60% of patients present
CONCLUSIONS: Following ALCAPA repair, LV function significantly improved,
among theregardless
37 patients of
whoage at the time
underwent repair of repair.
after In addition,
1995. Among preoper-
more before ALCAPA repair. Systolic f
ative functional MV regurgitation decreased over time. Concomitant mitral valve surgery at the time of ALCAPA repair is required
patients repaired after 1995, freedom from death at 20 years cantly after in
repair and remained no
post-repair was 97± 3%. This long-term results of the study (up There was no significant difference in
patients with structural abnormalities of the MV.
to 40 years postoperatively) in a large patient population are function whether patients had unde
unique and have not been published by other investigators. before or beyond 1 year of age.
Keywords: Anomalous left coronary artery from the pulmonary artery repair • Left ventricular function • Coronary collateralization
Naimo et al. [14] recently reported 98% survival in 42 patients at The mechanisms for an age-indepe
20 years following ALCAPA repair. Survival rates after 10 years function remain speculative [24]. Withi
have been described by different authors
EuropeantoJournal
rangeofbetween 82% Surgery
Cardio-Thoracic mammalian hearts are able to regenera
0 (2017) 1–8
and 100% [15, 21]. doi:10.1093/ejcts/ezx407 tion of cardiac geometry after resectio
INTRODUCTION ischaemia may promote sudden death due to [25].
In all, 84% (Group A) and 79% (Group B) of our patients exhib-
ventricular
This capability is lost with incr
arrhythmia
ited [5]. at the final follow-up,
normal LV function with
Cite this article as: no difference
Lange Bergmann
R, Cleuziou J, Krane M, EwertetP,al. [26]von
Pabst showed
Ohain J,cardiomy
Beran E e
in outcomes whether ALCAPA hadpulmonary artery repair:before
been corrected a 40-year
orsingle-centre
1% inexperience. Eur J Cardiothorac
young probands, whichSurg 2017;
also dec1 F 67 Chest pain/Palpitations (AF)/HF ID 33
2 F 47 Palpitations (VT) II 44
3 F 41 Palpitations (VF) II 40
4 M 33 Chest pain II 62
5 M 70 Chest pain/Palpitations (AF, VT)/HF/syncope IV 30
Anomalous Origin of the Left Coronary Artery
6
7
M
M
36
25
Chest pain Palpitations (AF)
HF
II
IV
60
42
From the Pulmonary Artery Presenting in
8
9
F
M
27
16
Chest pain
Chest pain/Palpitations (JT)
ID
IV
60
69
Adulthood: a French Nationwide Retrospective
10
11
F
F
25
31
Chest pain
Chest pain/Palpitations (AF)
II 55
CONGENITAL – ANOMALOUS ORIGIN OF THE LEFTIIII: 55%
CORONARY ARTERY 57
Study All patients F: 64% 38 ± 17 Chest pain: 73%
Palpitations: 64% III-IV: Le
27%
50 ± 13
Berre
et
al.
2017
Sem
Thoc
Cardiovasc
Surg
Heart failure: 36% (ID: 18%)
N
=
11
Laura Le Berre, MD,* Alban-Elouen
Table 1. Patients Characteristics at Diagnosis Baruteau,
Syncope: 9% MD, †,‡
Alain Fraisse, MD, PhD,§,‖
1980-‐2014
Dominique
PatientforBoulmier,
Values all patientsGender MD,as
are expressed
¶
AgeMaria
mean Jimenez,
at ± standard deviation
Symptoms MD,# Bruno Gallet, MD, PhD,**
or percentage. NYHA Class LVEF (%)
AF, atrial fibrillation; F, female; HF, heart
†† failure; ID, indeterminate ; JT, junctional tachycardia; LVEF, left ventricular ejection fraction; M, male; NYHA,††
Karine New
Warin Fresse, MD, Jacques
Diagnosis (y) Mansourati,
York Heart Association; VF, ventricular fibrillation; VT, ventricular tachycardia.
MD,* and Patrice Guerin, MD, PhD
1 F 67 Chest pain/Palpitations (AF)/HF ID 33
Anomalous 2 origin of the F left coronary 47 artery from the pulmonary
Palpitations (VT) artery (ALCAPA) II 44
is a rarediagnosis (all 4 tests
3congenital heart F
were disease
necessary in 1 patient, 2 orPalpitations
41 usually diagnosed
3 in 6 pa- during collaterals.
(VF) theAll patients
first monthswere found to II
have perfusion abnormali-
40
tients,
of life. Without
4 and surgical
1 in 4 patients).
M treatment, 33 ALCAPA carries Chest pain a high ties,mortality
mainly in therisk,anteroseptal
and and anterolateral
II territories.
62
Coronary angiography
disease 5presentation revealed70
in adulthood
M theis presence
rare. of We giant arteries
describe
Chest in the diagnosis
pain/Palpitations and man-
(AF, VT)/HF/syncope IV 30
the
6 right coronary system,
M which
agement of patients presenting with ALCAPA in adulthood. irrigated
36 the left system,
Chest as well
pain Patient
Palpitations Management
(AF)
This multicenter II 60
as
7 in several collateral
French nationwide M arteries. MRI
retrospective allowedincluded
25study analyzing HFthe myo-patients
adult Ten (91%)
diagnosedpatients underwent
from surgery
IV (Table 2). The 42 mean
8
cardial perfusion. FAnomalous origin 27 of the left coronary
1980 to 2014. Eleven adult patients (mean age: 38 ± 17 years) were ana- Chest pain was EuroSCORE was 8 ± 7. One patient ID
was denied surgery 60
because
9
confirmed, and M ventricular function
left 16 was assessed.ChestLack pain/Palpitations
of of age (JT)years old) and comorbidities.
(70 IV In 6 patients out 69 of 10
lyzed. All patients were symptomatic, presenting with chest pain, palpitations,
10
collaterals F was25 reported (in 2 cases,Chest pain II 55on the
heart failure,
11 ororsyncope.
their localization
F Electrocardiogram
31
collaterals
was
Chest abnormal operatedin
pain/Palpitations
(60%),
(AF) 8 (73%)the left coronary
pa- system
II
was reimplanted
57
were present in the anterior
tients. Echocardiogram showedterritory). No pericardial abnormali- ascending aorta. The other patients underwent closure of the anom-
All patients F: 64% 38 a ± 17 mildly depressed
Chest pain: left 73% ventricular ejection II: 55% 50 ± 13
ty was found. Non-compaction
fraction of 50 ± 13%, kinetic abnormalities in of the left myocardium was found
5 (45%)64% patients, ofand
alous origin the coronary
signifi-artery by a pericardium patch and a
Palpitations: III-IV: 27%
in 1 patient. Myocardial
cant mitral regurgitation in 8 (73%) patients.scintigraphy (exercise myocardial perfu-
Coronary single coronary artery bypass grafting (the left anterior descending
Heart failure: 36% angiography was (ID: 18%)
performedsion inimaging)
10 (91%) was alsopatients
used to assess andmyocardial
confirmed irrigation
the by
Syncope: 9% coronaryComputerized
diagnosis. by either internal mammary artery in 3 patients or
tomographyValues forscan, magnetic
all patients are expressed resonance
as mean ± standard imaging,
deviation or and myocardial scintigra-
percentage.
phy were AF, performed
atrial fibrillation; F, when
female; HF, deemed
heart
Table 2. Patients Characteristics After Surgery failure; ID,necessary.
indeterminate ; Ten
JT, patients
junctional tachycardia;underwent
LVEF, left ventricular ejection
CT scanfraction;
showingM,abnormal
male; NYHA,
origin of the left coronary
New York Heart
reconstructive Association;
surgery, but VF,
1 ventricular
patient fibrillation;
was VT, ventricular
not operated tachycardia.
because of age. Four artery from the pulmonary artery (white arrow).
Patient Time From EuroSCORE Surgery Complications NYHA Class LVEF at Follow-up
patients experienced postoperative
Diagnosis to complications Procedure including of Surgerycardiogenic shock, at Last Visit Last Visit Period (mo)
diagnosis
heart failure, (all 4Surgery
renal tests were
failure, (d)
necessary
or additionalin 1 patient, 2
surgery.or 3 in 6
Afterpa- a collaterals.
median All patients were
follow-up offound Central
to have perfusion
Messageabnormali-
2.5 years,tients,
alland 101 in 4 patients). patients were alive and asymptomatic,
operated ties, mainly in theand anteroseptal
the andALCAPAanterolateral territories.
1 18 8 P + CABG + HF + RF + dialysis is rarely
126diagnosed in adults, but sur-
nonoperated Coronarypatient angiography
had revealed
died at thethepresence
age of
ofgiant
70 arteries
from inCS
syncope related to
II
ven- gical
50
2 44 20 R RF II 61 correction168 in adulthood appears to be
tricular 3the right coronary system,
tachycardia. ALCAPA which irrigated the left system, as well in Patient Management
14 20 may beP +diagnosed CABG CS + RFadults. Although II associated
60 with 72favorable long-term outcome.
4as in several
complications may collateral
180occur arteries. 5MRI allowed analyzing
postoperatively, R long-termthe myo-Ooutcome Ten (91%) patients I underwent
is favorable in 55 (Table 2).
surgery 30 The mean
5cardial perfusion.
adult patients undergoing Anomalous
No surgery origin correction.
surgical of the left coronary Surgerywas shouldEuroSCORE bewas 8 ± 7.IVOne patientPerspective
discussed was38denied Statement
surgery
18 because
6confirmed,
as first-line therapy and IDleft
in ventricular
adults 4.6 function
with was assessed.
ALCAPA. P + CABG(V) Lack ofO of age (70 years old) and I comorbidities. In 6 patients
ALCAPA is a NA
50 out of 10
rare congenital heart disease
7collaterals or their 395localization was 1 reported (in 2CABG cases, collateralsO operated (60%), the leftII coronary system 45 was reimplanted
288 on the
usually diagnosed during the first months of life.
Semin Thoracic
8were present in Surg ■■:■■–■■
IDthe anterior territory).
6 No© 2017
pericardial
R Elsevier Inc.
abnormali-Additional Allsurgery
ascendingrights * The
aorta. reserved.
other
I patients underwent closureNA
60 surgical
Without of the anom-
treatment, mortality is high and
9ty was found. Non-compaction
ID 6of the left myocardium R was foundO alous origin of the coronary I artery by a76
pericardium
presentation 13patch andisa rare.
in adulthood
Keywords:10
ALCAPA, 32
Bland-White-Garland
3 R
syndrome, congenital heartI
in 1 patient. Myocardial scintigraphy (exercise myocardial perfu-O single coronary artery bypass graftingWe 55
describe
(the the2 management
left anterior descending of 11 adult pa-
disease,11myocardial 2 infarction, 6 congenital R heart disease O I tients54 with 11
ALCAPA. Although complications
sion imaging) was also used to assess myocardial irrigation by coronary by either internal mammary artery in 3 patients or
All patients 32 [2:395] 8±7 may55occur
± 10 postoperatively,
I-II: 91% 2.5 y [2.2:24]long-term outcome
is favorable, suggesting surgery should be con-
III-IV: 9%
Table for
2. Patients Characteristics After Surgery sidered as first-line therapy in adults with
Values all patients are expressed as median with range or mean ± standard deviation or percentage. ALCAPA.
*Brest University
*Patient Hospital,
Patient required TimeWestern
additional Brittany
Fromsurgery for leftUniversity,
EuroSCORE Brest,
coronary artery and France
Surgery pulmonary artery truncus stenosis with NYHA
Complications tricuspid regurgitation.
Class LVEF at Follow-up
†
Marie-Lannelongue Hospital, Paris-Sud University, Paris, France
CABG, coronary artery bypass grafting; CS, cardiogenic shock; HF, heart failure; NA, not available; P, pericardium patch; R, reimplantation onDiagnostic des formes « pièges » • Laurie, née le 13/11/95 • Aucun antécédent personnel • ETT normale à 4 ans pour souffle • Douleur thoracique rétro-sternale constrictive à l’effort depuis deux ans avec blockpnée, sans dyspnée ni orthopnée, ni syncope, ni palpitation • Majoration récente des douleurs (sport+++) • Epreuve d’effort au centre de l’asthme!!
ECG de surface et EE V4
Echographie avec VG normal!!
Echographie ALCAPA avec sténose de l’ostium gauche Rôle de la sténose de l’ostium gauche dans la bonne tolérance : évite le vol diastolique dans l’AP?
Scanner coronaire CD très dilatée et la CG sténosée dans l’AP (gicleur)
Piège numéro 2
Lucie née le 4/12/2002
Echographie pour souffle
Fonction VG normal, coronaire gauche bien vue et flux
« bizarre » dans l’AP
ARCAPADiagnostic?
IVC
LA
Ao RA
PA
RV
RV
Coronary LV
veins
Coronary
veins
Legendre A, Houyel L, Serraf A. N Engl J Med 2006 ; 355 : 631-633Vous pouvez aussi lire