Retour d'expérience des attentats de Paris - Pr. Pierre CARLI SAMU de Paris Hôpital Necker - LAST retour exp attentat 2018 Lyon
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous

Retour d’expérience des attentats
de Paris
Pr. Pierre CARLI
SAMU de Paris Hôpital Necker
Le 13 Novembre 2015 • Un attentat multisite multimodal • Le plus grave en France depuis la seconde guerre mondiale : 130 DCD plus de 410 blessés • Suivi d’une vague d’attentats sans précédent en Europe

Le SAMU de Paris
Les SAMU d’IDF en première ligne
19 ans après le dernier
attentat terroriste perpétré à
Paris en 1996
L’attentat terroriste Une crise particulièrement intense • Qu’avions nous préparé avant ? • Qu’avons nous fait pendant ? • Quels sont les leçons à l’usage de tous les responsables Un parcours de l’événement, de l’urgence à la résilience ….

Avant …
La menace terroriste n’est pas
une surprise complète
Attentats terroristes à Paris 1995 -1996

Attentat terroriste de Port Royal à Paris 1996 70 victimes (12 UA 58 UR) et plus de 400 personnels sur place : Rapport 1/4 ou plus … 17 hôpitaux reçoivent les victimes

Plan Rouge pré hospitalier
puis plan NOVI
T=O Site
SMUR
Réanimation
Triage
T = Minutes
SAMU
T = Heures (1-2) Régulation
PMA
Traitement définitif
UA UR H
SAU 1
H REA 1
H REA 2
H REA N SAU N
H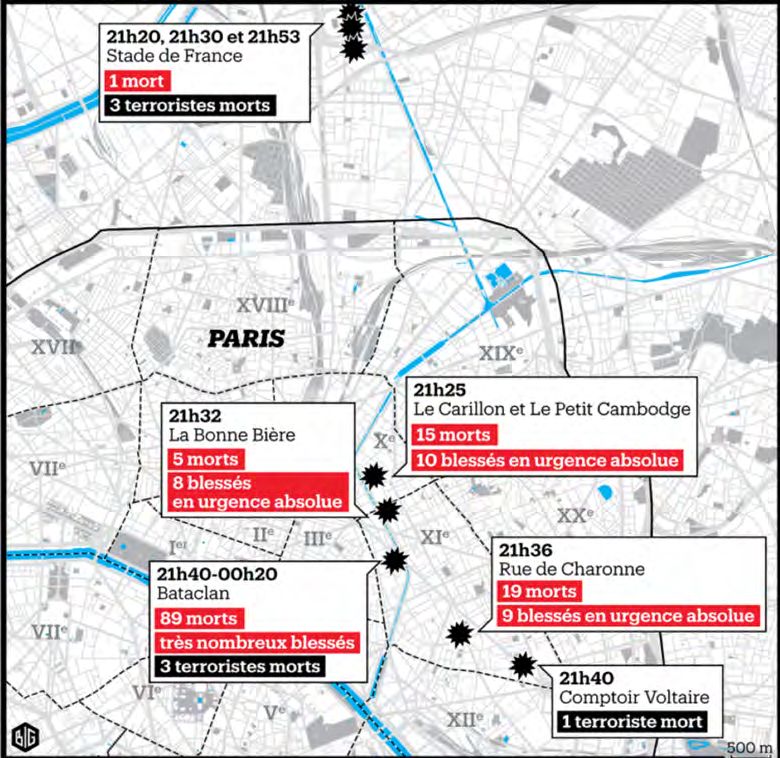
Plan Blanc hospitalier
• Une obligation réglementaire
pour tous les établissement
de santé
– Réponse à un afflux de victimes
– Ou une situation sanitaire
exceptionnelle
L’hyper terrorisme et les attentats
multi sites
• New York 2001
•Madrid 2004
• Londres 2005
• Bombay 2008Bombay 2008 : attentat multisite et multimodal
• 10 sites d’attaques avec fusillades,
explosions et prises d’otages :
– gare, métro, restaurants, Police, hôtels
de luxe, hôpital …
• 10 terroristes , plusieurs commandos
• 188 DCD 312 blessésUn double enjeu • Adapter nos techniques de soins aux victimes de fusillades – Principes du « Damage control » • Mettre en œuvre une stratégie qui permette aux équipes médicales de « couvrir » l’ensemble des sites et de s’adapter à l’évolution de la crise – Le plan attentats multi sites « camembert » du SAMU – Articulé avec le Plan Rouge Alpha de la BSPP
« Damage Control » pré hospitalier
Tourtier JP and Carli P , AFAR , 2013, 520 - 6
• Traitements simplifiés
– Hémorragie externe = Garrot /
compression
– Hypotension permissive = Objectif
conscience +
– Acide tranexamique = 1g / 20 min
– Prévention de l’hypothermie
– O2 et pas d’intubation exsuflation PNO /
ventilation mécanique
– Analgésie limitée
• Evacuation vers Bloc pour hémostase dans
les 60 minChaine Médicale de l’Avant
modifiée pour le « Damage Control »
Impliqués CUMP
H
Grande Noria
Evacuation
H
TRI
secouriste
PRV TRI PMA
Médicalisation Petite Noria
De l’avant Ramassage
Priorité à l’hémostase chirurgicale des UA instables Bloc
2 exercices de terrain en 2013 et 2014 pour Réveil
préparer une fusillade
Carli P et Al JEUR 2017Renfort
SAMU 95
SAMU 93
Vers le 93
le 92
Vers SA
MU
94
2 Ve
SAM U9 rs
le
9 4
Stratégie en cas
Renfort
SAMU 78
d’attaque multisite Renfort
SAMU 77 91J a n vi er 2 0 1 5
1 p oli ci er bl ess é
p ar b all e U R V P
1 P oli ci er e n A C R
+ 2 P oli ci er s U R V P
11 DC D 4 U A
1 d a m a g e c o ntr ol
1 U R all o n g é e
s ur l e s ol
T o urti er J P … C arli P et Al A m J E m er g M e d 2 0 1 5Double prise d’otages 9 janvier 2015
• Un type d’intervention
différent des fusillades
• Le premier multisite IDF
17Pendant …
Le jour de l’attaque
La préparation à l’épreuve des
faitsLe 13 Novembre 2015
L’attaque terroriste multisite et
multimodale de ParisExercice «Tireurs dans la ville » Samu Zonal le
matin du Vendredi 13 Novembre 2015 à 9h30
Une répétition 12h avant …Les sites d’attentat du 13 novembre 2015
■ 21h20 Stade de France : 3
Kamikazes.
■ 21h20 une première explosion
près de la porte D du Stade de
France Stade de France
■ 21h 30 deuxième explosion près
de la porte H
■ 21h53 troisième explosion
restaurant Mac Donald Le Petit cambodge
?
Casa Nostra
■ 21 h 25, une seconde équipe ouvre Bd Voltaire Bataclan
le feu sur un bar et un restaurant
angle rues Bichat et Alibert, dans le Rue de Charonne
10e arrondissement.
■ À 21 h 40, une troisième équipe
composée de trois hommes arrive
au Bataclan et tire sur les
spectateurs.
2
1Stade de France
• Secteur Nord du
camembert
• SAMU 93 engagé
• Aucune unité du
SAMU de Paris
Une attaque potentiellement majeure31 UR 21h20 Stade de France
2
2 1
3 DCD 6 UA 11 UR
• Explosion de 3 bombes
kamikaze
• Public 70 000 et VIP
21h17 • Dispositif de secours et de
1
soins pré positionné
• SAMU 93 BSPP sur place
21h45
3 3
1 DCD 1 UA 10 URStade de France • Les terroristes étaient en retard • Le match n’est pas interrompu • Le stade n’est pas évacué • Les bombes explosent loin de la foule Echec d’une attaque potentiellement majeure
Les sites « fusillades » = secteur EST
• Un commando mobile
• Des cibles au hasard
• Un bilan très lourd :
– 40 DCD 32 UA
• Une diversion … ?
25Rue Bichat et hôpital Saint Louis
■ Arrivées spontanées à ST Louis
■ Avant toute alerte !
■ Victimes portées par les témoins :
UA et UR
■ Brancardage depuis le site d’ UA
■ Adaptation et renforts
chirurgicaux ultérieursRue de Charonne ■ Transports à ST Antoine non médicalisés mais régulés depuis le terrain adapté au service d’orthopédie ■ UA envoyées à la Pitié ■ Mise en sécurité des impliqués dans la caserne de la BSPP
Les terraces : un
• Street cordoned off by Police and
Army
environnement
• Fire fight in thetrès
streets nearby the
sites
dangereux
• Difficult and dangerous access to
• Commando en mouvement
victims (bombs ?)
• Evacuation and escape routes
• Tirs dans les rues
blocked and unsafe
• Rue• barrée par la Police
Terrorist commando still firing and
moving in a car in the area ?
• Impossible de délimiter les zones dangereuse
• Pas le temps de formaliser des PMA : Points de rassemblement des
victimes PRVLe site du Bataclan Le point de vue médical
• 21h40 Les 3 kamikazes
Dans le Bataclan
gence
fusille la foule depuis la
scène 80 tués
• 22h Le comissaire de
garde entre et tue un STA
GE
terroriste
• 22h15 BRI RAID entre
dans le theatre
• Assaut final à 0h18
Extraction des
blessés par les
médecins BRI
RAID
1rst floor
Entrée
RAID AFMU 2016 DOI 10.1007/s13341-015-0601-4La zone rouge du Bataclan
des médecins d’intervention à l’intérieur du Bataclan
Comandement « Préfet de Police »
Extraction
Nid de
victimes
PRV
RAID AFMU 2016 DOI 10.1007/s13341-015-0601-4Le Bataclan : Le pire des scénarios • Un concert avec 1500 spectateurs • 21h40 : 3 terroristes – Ouvrent le feu devant puis à l’intérieur du théâtre – Exécutent froidement les spectateurs • 22h00 : – Fusillade avec la BAC : un terroriste tué – Intervention BRI et RAID • 0h18 : Assaut et neutralisation des 2 autres terroristes retranchés à l’étage
Le site du Bataclan
ZONE VERTE ZONE ORANGE ZONE ROUGE
n
ractio
Ext
NID DE VICTIMES
n
atio BATAC
Eva
cu LAN
PMA
UA
AMP
UR
Une adaptation de la chaîne médicale classiquePMA UR PMA UA Les PMA du Bataclan
Les PMA du Bataclan
Sécurité sur le terrain :
Danger y compris au PMA en zone protégée
3
6SAMU de Paris: La régulation des événements
en salle de crise zonale
Mise en œuvre des moyens
Alerte : Générale et Inter région (DGS)
Mobilisation : Rappel APHP et Zonal
Coordination avec la BSPP et La
préfecture de Police 3
7Répartition des urgences
absolues (UA) et relatives (UR)
dans les hôpitaux de l’APHP
Hôpitaux militaires:
Percy et Begin: 18 UA + 34 UR =
52 blessés
17 hôpitaux APHP et SSA
354 blessés Hospitalisés
Mortalité cohorte APHP à 1
mois : 1,3 %
Pas de transfert secondaire en
urgence
Hirsch M , Carli P et al., Lancet 2015Hôpital Saint Louis
• Dans une zone de fusillade
• Arrivée des premières victimes à pieds avant toute alerte
• Retour spontanné des personnels du “quartier”
• Plan blanc auto déclenché : UA en SSPI
• Augmentation majeure du potentiel chirurgical
• Renfort chirugical spécialisé plus tard
• Très forte activité mais pas de saturation: 26 victimes, 11 UA, 15 UR
Haug C, NEJM , 5/12/2015
39Hôpital Pitié Salpêtrière
• Un des 7 Trauma Center IDF
• Activation très rapide du plan blanc : première
arrivée spontanée
• Retriage à l’arrivée:
• Admission immédiate des UA en SSPI
• Pour chaque UA 1 équipe chirurgien
anesthésiste
• 10 blocs activés en simultanné : pas de
sturation
• Total: 53 victimes, 28 UA, 25 URAprès … Les leçons, les progrès
Impact médiatique et politique immédiat et très intense !
L’attentat terroriste le plus grave
survenu en FrancePour les services impliqués :
Une situation à très haut risque
médiatique et social
Héros De plus en plus déconnectée
d’une évaluation objective de
Victimes la réalité technique et
professionnelle
Incompétents
Malhonnêtes
Coupables !Les facteurs perturbants
• L’émotion:
– Des victimes et de leur proches
– De tout le monde : stupeur suivi du refus de la
réalité
• Les pseudo – experts médiatiques animateurs
de controverses
• Les professionnels jaloux, concurrents …
– Tout ceux qui veulent être sur la photo !
• Les justiciers et les donneurs de leçons
– Y compris ceux qui n’ont pas faits leur travailViewpoint
De nombreux autres rapports et
The medical response to multisite terrorist attacks in Paris
Martin Hirsch, Pierre Carli, Rémy Nizard, Bruno Riou, Barouyr Baroudjian, Thierry Baubet, Vibol Chhor, Charlotte Chollet-Xemard,
Nicolas Dantchev, Nadia Fleury, Jean-Paul Fontaine, Youri Yordanov, Maurice Raphael, Catherine Paugam Burtz, Antoine Lafont, on behalf of the
health professionals of Assistance Publique-Hôpitaux de Paris (APHP)
Introduction participated, especially in recent months, in exercises or Published Online
November 24, 2015
articles publiés
Friday, Nov 13, 2015. It’s 2130 h when the Assistance in updating emergency plans.
http://dx.doi.org/10.1016/
Publique-Hôpitaux de Paris (APHP) is alerted to the In this report, we present the prehospital and hospital S0140-6736(15)01063-6
explosions that have just occurred at the Stade de France, management of this unprecedented multisite attack in
Assistance Publique-Hôpitaux
a stadium in Saint-Denis just outside Paris. Within Paris from the viewpoint of the emergency physician, the de Paris, Paris, France
20 min, there are shootings at four sites and three bloody trauma surgeon, and the anaesthesiologist. This is a (M Hirsch MsC); SAMU de Paris,
testimony on behalf of the health professionals involved
NEW ENGLA ND JOURNA L MEDICINE
explosions in the capital. At 2140 h, a massacre takes Hôpital Necker-Enfants
place and hundreds of people are held hostage for 3 h in in the night of Nov 13. The
Malades, University
Paris-Descartes Paris, France
of
Bataclan concert hall (figure). (Prof P Carli MD); Hôpital
The emergency medical services (service d’aide médicale The emergency physician’s perspective Lariboisière, University
d’urgence, SAMU) are immediately mobilised and the Triage and prehospital care were the duty of SAMU. In Paris-Diderot, Paris, France
(Prof R Nizard MD); Hôpital de
crisis cell at the APHP is opened. The APHP crisis unit the minutes that followed the suicide bombing at the la Pitié Salpétrière, University
is able to coordinate 40 hospitals, the biggest entity in Stade de France, the Paris SAMU unit regulatory crisis Pierre & Marie Curie, Paris,
Europe with a total of 100 000 health professionals, a team began to send out medical workers to the emergency France (Prof B Riou MD);
capacity of 22 000 beds, and 200 operating rooms. It is sites from all eight units of SAMU in the Paris region and Hôpital Saint-Louis, Paris,
France (B Baroudjian MD,
very quickly confirmed that the attacks are multiple and from the Paris fire brigade (Brigade de sapeurs-pompiers J-P Fontaine MD); Hôpital
that the situation is highly scalable and progressing de Paris), alongside rescue workers and police. The Avicenne, University Paris 13,
dangerously. These facts led to a first decision: the regulatory crisis team was composed of 15 individuals to Paris, France
Perspective
activation of the “White Plan” (by the APHP Director answer the calls, and five physicians. Their mission was (Prof T Baubet MD); Hôpital
Européen Georges Pompidou,
General) at 2234 h—mobilising all hospitals, recalling to organise triage and dispatch mobile units (composed Paris, France (V Chhor MD);
staff, and releasing beds to cope with a large influx of of a physician, a nurse, and a driver) to the wounded and Hôpital Henri Mondor, Créteil,
wounded people. The concept of the White Plan was to the most appropriate hospitals. As part of the White France (C Chollet-Xemard);
developed 20 years ago, but this is the first time that the Plan and ORSAN (organisation de la réponse du système de Hôtel Dieu, Paris, France
(N Dantchev MD); Hôpital de la
plan has been activated. It is a big decision, and timing is santé en situations sanitaires exceptionnelles), 45 medical Pitié Salpétrière, Paris, France
key: it would lose its effectiveness if taken too late. On the teams from SAMU and the fire brigade were divided (N Fleury MsC); Hôpital
night of Friday Nov 13 to Saturday Nov 14, the activation between the sites (figure) and 15 were kept in reserve, Saint-Antoine, Paris, France
(Y Yordanov MD), Hôpital
of the White Plan had a critical effect. At no time during since we did not know how and when this nightmare
Bicêtre, Paris, France
the emergency was there a shortage of personnel. During would end. This approach avoided early saturation of (M Raphael MD); Hôpital
these hours, as the number of victims increased, with a services—often, in emergency situations, all the resources Beaujon, University
sharp increase after the assault was launched inside
the Bataclan, we were able to reassure the public and
are focused on the first crisis site, leaving a shortage for
Report from Paris
Paris-Diderot, Paris, France
government that our abilities matched the demand. And Stade de France Charlotte J. Haug, M.D., Ph.D.
when we felt that it might be necessary to deal with an (Saint-Denis)
“Wea can
influx of severely injured people, two further “reservoir” 8 medical teams
capacities were prepared: other hospitals in the area were meet after my lecture, at a table, over asked her what was happening,
put on alert, together with some university hospitals, Casa Nostra drink,” Carl Ogereau told me — that’s and told her that if there was
more distant from Paris, but with the ability to mobilise 4 medical teams
Le Petit Cambodge, shooting and people were wound-
ten helicopters to organise the transport of the wounded. “the French way to fight terrorism,” he explained:
Le Carillon
ed, the police and the Services
9 medical teams
These other two reservoirs have not been used, and we La Comptoir Voltaire refusing to be intimidated. So on Friday evening, d’Aide Médicale Urgente (SAMU),
believe that despite this unprecedented number of 3 medical teams the medical emergency service,
wounded, the available services were far from being Bataclan
saturated. While hospitals were receiving and directing 15 one
medicalweek after the Paris terrorist It started as an ordinary Friday would arrive soon. But she
teams
patients to specific institutions based on capacity and
attack that left 130 dead and night, the emergency department wouldn’t calm down.
La Belle Equipe
specialty, a psychological support centre was set up. hundreds injured, Ogereau arrived full of patients. Saint Louis is a “The situation was odd, but
medical
6 on
35 psychiatrists, together with psychologists, nurses, and his
teams motorbike at Café Clochette specialized hospital, known for its she was so insistent that in the
volunteers were gathered in a central Paris hospital, across the street from the Hôpi- hematology, oncology, urology, end I just gave her a stretcher,”
Hôtel Dieu. Most of them had played a similar role tal Saint Louis. Nearby, we saw and nephrology services. It treats Ogereau said. Neighbors or friends
during the attacks against Charlie Hebdo. Most of the candles and flowers outside Le burns and does transplantations, brought in the first victim. The
emergency workers and health professionals working on Carillon and Le Petit Cambodge, skin surgery, and plastic and second came on a stretcher. “And
the evening of Nov 13 had already been involved in the restaurants where more than maxillofacial surgery. It has in- after that, stretchers, stretchers,
serious crises, were used to working together, and had Figure: Map of Paris attacks and prehospital emergency response
a dozen young people had been ternal medicine and support ser- stretchers, patients, patients, pa-
killed and many more severely in- vices, plus emergency depart- tients.” The first patient was a
www.thelancet.com Published online November 24, 2015 http://dx.doi.org/10.1016/S0140-6736(15)01063-6 jured 1the previous week. The res- ment and intensive care units. But young man who didn’t know he’d
taurants are so close to the hospi- it is not a trauma center. There is been shot. “He said, ‘I felt some-
tal that wounded people escaping no neurosurgery or orthopedic, thing bizarre. I have pain. I can’t
from the massacre walked to the thoracic, or vascular surgery. walk.’ He had two bullets, one in
emergency department or were Some time around 9:30 p.m., the back and one in the leg. The
brought there by bystanders. a colleague ran into the emergen- second patient was a grandmother
Ogereau, the assistant head cy department, shouting breath- who had been leaning over her
of the emergency department at lessly that there was shooting grandson to protect him.”
the Hôpital Saint Louis, was in outside and she needed a stretcher. When the third patient ar-
charge on Friday, November 13. Ogereau tried to calm her down, rived, the emergency physicians
n engl j med nejm.org 1
The New England Journal of Medicine
Downloaded from nejm.org on December 5, 2015. For personal use only. No other uses without permission.
Copyright © 2015 Massachusetts Medical Society. All rights reserved.
Commission d’enquête parlementaire , enquête judiciaire en cours …Adapter la réponse
d’urgence
et
Favoriser la résilienceThe French emergency medical services after
Insufficient expertise on war weapons
French actions
(Continued from previous column)
French actions
the Paris and the Nice attacks: what have learnt?
Expertise transfer from the Military Medical service Ongoing Terrorist attacks in an area with insufficient medical resources
Training of EMS personels and physicians Done Early activation of distant resources Done (regional and
(ie, regional, national,7 or international) national); to be
Basic teaching to all medical students To be implemented
implemented
Advanced teaching for anaesthesiologists, surgeons, To be implemented (international)
and emergency physicians during their fellowships
French actions French actions
Identification of the victims
Prehospital
fficient expertisedamage
on war control
weapons
4
(Continued from previous column)
New standard operating procedures for victim Done
Equipment
ise transfer (tourniquet
from andMedical
the Military dressings) and
service Done
Ongoing Terrorist attacks in an area with insufficient medical resources
identification
prehospital administration of tranexamic acid Done Early activation of
ng of EMS personels and physicians Reconciliation ofdistant resources
the prehospital and hospital Done (regional and
Done
Expertise (ie,admission
regional, national, or international) national); to be
to alltransfer from the military medical service
To be Ongoing
7
eaching medical students implemented identification number
(not to apply to every type of trauma5) implemented
ced teaching for anaesthesiologists, surgeons, To be implemented Care of the psychological victims (international)
General
mergency public teaching
physicians during their fellowships Pilot programme
Improve our ability
Identification of theto care for a high number of
victims Ongoing
Children
spital damageas victims
controlof ballistic trauma victims over operating
a longer period to prevent
forPTSD
4
New standard procedures victim Done
mentExpertise transfer
(tourniquet andfrom adult to paediatric
dressings) and physicians
Done Ongoing Conduct clinical trials to test therapeutic
identification Ongoing
spitalfor
administration
specific trainingof tranexamic
(ballistic trauma,acid
CBRNE) interventionsoftothe
alleviate and suppress PTSD
Reconciliation prehospital and hospital Done
ise transfer from
Expertise the military
transfer from themedical service
paediatric to the Ongoing
Ongoing symptoms
admission identification number
o apply to physicians
adult every type(in
of case
trauma 5
)
of excess capacity of International
Care medical network
of the psychological on terrorist attacks
victims
paediatric
al public hospitals)
teaching Pilot programme
Expertour
Improve meetings
abilitytoto
share
careexperience
for a highand
number of Ongoing
Ongoing
en as victims ofbetween
Cooperation ballisticadult
trauma
and paediatric centres Ongoing victims over a longer
implementation period
of new to prevent
measures: PTSD
UK, Spain,
ise transfer
Chemicalfrom adult to paediatric physicians
weapons Ongoing Belgium,
Conduct Germany,
clinical trialsDenmark, Israel , USA, and Japan
to test therapeutic Ongoing
ecific training (ballistic trauma, CBRNE) interventions
Improve our global preparedness Ongoing Unexpectedtoterrorist
alleviate and suppress PTSD
innovation
tise transfer from the paediatric to the Ongoing symptoms
Upgrade ofcase
EMS of
equipment Ongoing To be prepared to be surprised 8
Never enough
physicians (in excess capacity of International medical network on terrorist attacks
atric Health-care
hospitals) facilities as target prepared
Expert meetings to share experience and Ongoing
ration between adult andinpaediatric centres plans,
Ongoing The plans “used as a tools box” should authorise Never enough
Include this possibility the mass casualties Ongoing implementation of new measures: UK, Spain,
sufficient local or regional autonomy prepared
both at the prehospital and hospital levels
ical weapons Belgium, Germany, Denmark, Israel , USA, and Japan
Encourage terrorist
Unexpected innovationinnovation Never enough
Secure
ve our intervention
global of medical responders “under
preparedness fire”
Ongoing
prepared
de ofCooperation
EMS equipment Ongoing
between all emergency responders Done To be prepared to be surprised8 Never enough
(police, rescuers, and medical responders) 6 prepared
h-care facilities as target PTSD=post-traumatic stress disorder. EMS=Emergency Medical System.
Triage on scene andmass
at thecasualties
arrival of plans,
the hospital The plans “used asbiological,
CBRNE=chemical, a tools box” shouldnuclear,
radiological, authorise Never enough
and explosives.
e this possibility in the Ongoing
sufficient local or regional autonomy prepared
t theExpertise
prehospital and hospital levels
transfer from the military medical Ongoing Table: Identified
Encourage weaknesses during the recent FrenchNever
innovation terrorist attacks1,3
enough
e intervention of medical
service to civilian ones responders “under fire”
in Europe and proposed solutions prepared
ration betweenexercises
Simulation all emergency responders
to improve Done Ongoing
the whole process
e, rescuers, and medical responders)6 PTSD=post-traumatic stress disorder. EMS=Emergency Medical System.
Analyse existing database (research)
on scene and at the arrival of the hospital
Ongoing CARLI P , PONS F, et Al The Lancet 2017
CBRNE=chemical, biological, radiological, nuclear, and explosives.
During and after the Paris and Nice attacks, many
ise transfer from the military medical Ongoing http://dx.doi.org/10.1016/S0140-6736(17)31590-8
(Table continues in next column)
individuals
Table: Identified required
weaknessespsychological
during the recentcare,
Frenchirrespective of
terrorist attacks 1,3
e to civilian ones
inwhether
Europe andthey
proposed
hadsolutions
been wounded physically. Theseand paediatric teams); and second to ident
Major terrorist attacks in additional preserved resources such as local
available hospitals because of the evo
Europe since 11/2015 unpredictable nature of terrorist attacks.
strategy is needed, coordinated by experien
Manchester
May 22, 2017
23 dead
Stockholm
April 7, 2017
• Vague d’attentats
care professionals, not only on scene but
regional or state level.7
119 injured 5 dead
14 injured • Touchant l’Europe
Emergency services must also be prepar
very different scenarios, including attacks wit
London
March 22, 2017
• 8 attaques
weapons (such as sarin, mustard gas, or c
recently used in the Middle East), and attac
6 dead
>49 injured
Berlin
December 19, 2016
majeures depuis
at iconic victims such as children or emer
responders. There is no reason to think tha
will become less violent. However, the rec
Brussels
March 22, 2016
12 dead
56 injured Paris
suggest that simple means (such as h
weapons and trucks) can result in a very high
London
June 3, 2017
35 dead
340 injured • Multiples attaques
victims.1,3 Protecting hospitals against an atta
11 dead new challenge for health-care authorities. H
48 injured
mineures
facilities are no longer sanctuaries but soft
terrorists.13 Professionals must be responsib
Paris
November 13, 2015
• Des milliers de
own security; in view of this, timely updated
emphasising protection of hospitals have b
cibles possibles
137 dead
413 injured duced in France.14
Exsanguination remains a major problem
attacks using high-velocity war weapons. Eq
all rescuers with tourniquet and haemostat
Nice might be a simple and efficient solution for som
July 14, 2016 and a rapid transfer to hospital for immedi
87 dead
458 injured
is another important issue requiring a v
cooperation between actors. We should also b
Barcelona Cambrils,
Alcanar to observe early deaths due to exsanguination
Aug 17-18 2017
CARLI P , PONS F, etourAl efforts
The Lancet Published
and this online
must be 7 25, to car
explained
Dead 24 (16+8) 2017 http://dx.doi.org/10.1016/S0140-6736(17)31590-8
and the population. This does not preclu
152 injuredLe terrorisme n’est pas une simple catastrophe
• Il a des cibles précises
• Une stratégie élaborée
• Kamikaze : Pas de négociation
Il faut opposer à une stratégie terroriste une autre stratégie
conçue à sauver le plus possible de victimesAttaques Terroristes:
XXX ?
un large spectre depuis
les attaques “Low Cost” NRBC
jusqu’aux mega
scénarios avec tueries Multimodal multisite
Camion bélier
de masse Fusils d’assaut
Bombe Kamikaze
Armes de poing
Bombe artisanale
Plaie par Voiture bélier
arme
blanche
Vous n’aurez jamais
le plan parfait !S’adapter rapidement
• Ne pas essayer d’appliquer à toute
nouvelle circonstance le plan issu du
RETEX de l’événement réel ou simulé
antérieur qu’on a pas su traiter !
• Aucun plan ne sera parfaitement adapté
à l’attentat terroriste auquel il faut faire
face
52Attention à la dictature du plan !
CAUTION
Construire une stratégie et apporter une
réponse opérationnelleL’adaptabilité est essentielle ! • Les plans ne sont pas la Bible mais la boite à outils de la stratégie à opposer à l’attaque terroriste • Pendant la crise il est nécessaire de prendre des décisions opérationnelles et de les faire appliquer
Dispositif ORSAN
Décrets, arrêtés, circulaires
TEXTES GÉNÉRAUX
MINISTÈRE DES AFFAIRES SOCIALES ET DE LA SANTÉ
Décret no 2016-1327 du 6 octobre 2016 relatif à l’organisation de la réponse du système de santé
(dispositif « ORSAN ») et au réseau national des cellules d’urgence médico-psychologique pour
la gestion des situations sanitaires exceptionnelles
Une coordination et une complémentarité étroiteNOR : AFSP1617819D
– ORSAN
Publics AMAVI
concernés : agences dede la
régionales Santé
santé, professionnels de santé, établissements de santé, services de
l’Etat.
– :ORSEC
Objet NOVI de
modalités d’élaboration, laduSécurité
contenu dispositif ORSANCivile
et son articulation avec le plan départemental de
mobilisation.
Entrée en vigueur : le texte entre en vigueur le lendemain de sa publication.1. Kotz D. After double checking records, 2QwMjfM13). story/2013/04/boston-medical-mecca-
injury toll from bombs reduced to 264. Bos- 3. Kragh JF Jr, Littrel ML, Jones JA, et al. equipped-for-mass-trauma-90228.html).
Importance de la préparation
ton Globe. April 24, 2013:B3.
2. Gawande A. Why Boston’s hospitals were
ready. The New Yorker. April 17, 2013 (http://
Battle casualty survival with emergency tour-
niquet use to stop limb bleeding. J Emerg
Med 2011;41:590-7.
DOI: 10.1056/NEJMp1305480
Copyright © 2013 Massachusetts Medical Society.
NEJM 2013 368;21
We Fight Like We Train
Eric Goralnick, M.D., and Jonathan Gates, M.D.
A s we say in the U.S. Navy, charge of Alpha Pod (one of four The Boston Public Health
“We train like we fight, and separate 14-bed pods, all within Commission’s Medical Informa-
we fight like we train.” In Bos- the larger emergency department tion Center called; BWH would
ton, we do the same. [ED]) conducted a scan of our be receiving 8 patients from the
That was never more evident 55-bed ED. It was full: 47 patients scene. The team initiated Code
La devise de la Navy s’applique aux attentats terroristes
than at 2:50 p.m. on April 15, in beds, 6 in the hallway, 6 in the Amber, our hospital-wide disaster
when two explosive devices abrupt- waiting room, and 4 in the tri- response.
• Connaissance organisationnelle et médicale
ly shattered the 117th Boston age area. A senior EM resident who had
hospitalière et préhospitalière
Marathon. On Patriot’s Day, the One floor below the ED, our attended a disaster-management
day we commemorate the open- perioperative nurse administrator training session in October 2012
• Partage d’informations entre les services de l’état
ing battle of the Revolutionary reviewed his caseload: 30 of 42 reminded the team to consider
War in Lexington and Concord, operating rooms (ORs) were ac- the possibility of a hazardous-
• Réalisation d’exercices communs
Boston was under attack. tive, with 8 more available for material (HAZMAT) threat.
Over the past 8 years, Brigham the 4 patients waiting in the pre- As reports trickled in — thatLa nécessité d’utiliser
l’expérience militaire
et la transposer au
contexte de soins civils
• S : Stop the burning
process
• A : assess the scene
• F : Free danger from you
• E : Evaluate “ABC”Combat Casualty Care
et Soins en Situation d’insécurité
• M Massive bleeding control
• A Airways
• R Respiration
• C Shock
• H Head / hypothermia
• E Evacuation
Extraction de victimes par
des groupes spécialisés
Tourtier JP et Carli P Injury 2016 , 47 , 784
58Exercice de
Simulation
Scénario
interactif
commun
Importance de la
coordination opérationnelle
interservicesImportance de la coordination
opérationnelle
• Police
• Armée
• SAMU
• Pompiers , Secouristes
Souvent organisation complexe avec des
services « menants » et « concourants »
qui changentComité de rédaction Coordination scientifique Pr Pierre CARLI Pr François PONS Coordination de la rédaction Dr Alain PUIDUPIN Dr Jean-Marc PHILIPPE Dr Sergio ALBARELLO Comité de lecture Pr Jean-Pierre AUFFRAY Pr Paul BALANDRAUD Dr Laurent CAUMON
VIEWPOINT
Preparing for the Next Terrorism Attack
Lessons From Paris, Brussels, and Boston
JAMA Surg. Online 2017 Jan 25
Eric Goralnick, MD, MS The most recent spate of brutal terrorist attacks in Prevention is a critical tool we have in our arsenal
Brigham and Women’s Nice, Bangladesh, Baghdad, Istanbul, and Orlando high- against terrorism—but we need a revolution, not an
Hospital, Boston, lights the need for a more global concerted effort to evolution in our preparedness strategy.
Massachusetts;
gather and share lessons from these events among First, we must ensure that valuable lessons from
Harvard Medical
School, Boston, health care professionals. In June 2016, only a few days each attack, including interdisciplinary practices, prob-
Massachusetts; and after the mass shooting in Orlando, health care leaders lems, and recommendations, are captured and dissemi-
Harvard T. H. Chan from Paris, Brussels, and Boston gathered to discuss our nated in a rapid, standardized, academically rigorous af-
School of Public Health,
Boston, Massachusetts.
experiences in emergency preparation, response, and ter-action reporting system. Although there is consensus
recovery from each city’s recent terrorist attacks. A con- in the medical community on the value of sharing best
Frank Van Trimpont, ference jointly organized by the Paris Descartes Faculty practices and areas for improvement, the improve-
MD of Medicine and Harvard Medical School, followed by ment of our tactics based on lessons learned is not keep-
European Council of focus groups in Paris and Brussels, highlighted the par- ing pace with the increasing need for such information
Disaster Medicine,
Belgium; and Centre ticular health care challenges of responding to a multi- sharing. There remain numerous report formats that are
Hospitalier de Wallonie site terrorist attack; the need for a timely, standard- tailored to specific organizations and are not amenable
Picarde, Tournai, ized, academically rigorous approach to after-action to systematic comparison of practices and their
Belgium.
reporting; and the critical role of public engagement. implications.1 As a result, largely descriptive, anecdotal
• “ Pour vaincre le réseau terroriste en Afghanistan nous avons
The lessons gleaned from these attacks are cru- reports published through various outlets render com-
Pierre Carli, MD
Urgente de Paris construit un réseau” General S. McChrystal
cial, and our understanding of them continues to pilation of lessons learned impractical. In the aftermath
Hôpital Necker–Enfants evolve. What is certain is the need for greater invest- of terrorist events, affected communities are busy bal-
Malades, Paris France;
Assistance Publique
• Pour réduire la mortalité évitable des victimes nous devons faire
ment, integration, and standardization of disaster ancing media inquiries with VIP visits and maintaining
medicine curricula and the need to focus on translating daily operations. They are too busy to adequately di-
Hôpitaux de Paris, de même en médecine
military medical knowledge into civilian practice. gest experiences and assess better future response.
Paris, France; and Paris
Descartes University,
Paris, France. Partageons sans frontière les expériences
Although much has been made of the comparison
between the European prehospital philosophy of
On the other hand, Israel conducts a structured after-
action review after each mass casualty incident to sup-
d’événements rares et graves !
“stay and play” vs the United States “scoop and run”
approach, similar themes arose from Boston, Brussels,
port timely, standardized knowledge dissemination.2
A US standard of reporting and analysis is not withoutAnticipation des risques
et bench marking
• Partage international des expériences
– Utiliser toutes les sources possibles
• Partage des critères d’évaluation
– Basés sur les résultats médicaux (mortalité,
morbidité)
– Indépendants des systèmes d’urgence
• Création de référentiels adaptésFusillade au Mercy Hospital de Chicago
le 19 /11/2018
Sécurisation du
SAU et des abordsProfiter de l’afflux d’ambulance …
Attentats Terroristes Chimiques
• Le trio gagnant est dans le contexte
des conflits au moyen orient est
• Le chlore
• Le sarin
• L’ypérite
• A disposition des terroristes ou
réalisables sur place
66La réponse médicale
favorise la résilience
• La Santé est un des premiers facteurs de Résilience
• Elle s’oppose directement à l’objectif du terrorisme,
répandre la peur et panique , par :
• La résistance des services d’urgence à la
désorganisation malgré l’agression et la violence
• Le maintien de la qualité et de la sécurité des soins
malgré l’afflux de victimes et l’effet de surprise
• Le maintien des principes éthiques
67Triage and terrorism
PAPER
Second thoughts about who is first: the medical
triage of violent perpetrators and their victims
Azgad Gold,1 Rael D Strous1,2
1
Beer Yaakov Mental Health ABSTRACT dictionary becomes more specific: ‘the assignment
Center, Beer Yaakov, Israel Extreme intentional and deliberate violence against of degrees of urgency to wounds or illnesses to
2
Sackler Faculty of Medicine, Tel
Aviv University, Israel
innocent people, including acts of terror and school decide the order of treatment of a large number of
shootings, poses various ethical challenges, some related patients or casualties’. This definition implicitly
Correspondence to
to the practice of medicine. We discuss a dilemma illustrates the dominance of the conventional
Dr Azgad Gold, Psychiatry, Law relating to deliberate violence, in this case the aftermath approach according to which medical attention in
and Ethics Unit, Beer Yaakov of a terror attack, in which there are multiple injured emergency situations should be determined based
Mental Health Center, PO Box individuals, including the terror perpetrator. Normally, on the degree of urgency (the ‘worst-first’
1, Beer Yaakov 70350, Israel; the priority of medical treatment is determined based on approach).
azgad.gold@moh.health.gov.il
• Triage et attentat terroriste : Priorité au terroriste
Received 25 February 2016
need. However, in the case of a terror attack, there is
reason to question this. Should the perpetrator of
It seems to be current consensus that in medical
emergency situations those with remote or no pro-
Revised 21 July 2016
Accepted 8 August 2016
ou à la victime ? Pas de vengeance!
extreme violence receive medical treatment on the scene
before the victims if he or she is designated as the most
spects of survival are ‘triaged out’ and only those at
the second stage of severity, with a reasonable like-
29 August 2016 • Le maintien de notre éthique est essentiel !
Published Online First seriously injured? Or rather, should victims receive
medical care priority if they are also in some life-
lihood of survival despite their life-threatening
status, are prioritised for medical attention. Among
– Le plus grave d’abord même si cela peut bénéficier
threatening danger, although not at the same level of
severity as the perpetrator? We present two opposing
this group, the conventional approach holds that
priority to medical treatment is determined solely
parfois aux terroristes /victimes
approaches: the conventional ‘no-exceptions’ approach, based on need, namely, the level of injury.
which gives priority to the terrorist, and the justice- The conventional approach (which may be char-
oriented ‘victim first’ approach, which gives priority to acterised as universal and impersonal) would stateLa résilience médicale favorise
celle du public
• L’action des Services de Santé diffuse une image positive,
non violente qui privilégie l’individu
• Elle se substitue à l’engrenage de l’agression et de la
répression Don de sang le 16/11/2015
• La société soigne les
victimes (mais aussi
les terroristes)
• Elle incite le public à
s’impliquer pour
sauver les victimes
69Favoriser la résilience du public • En l’informant : – Réseau sociaux – Nouveaux média – Applications
Favoriser la résilience du public • En le formant • Pour apprendre les premiers gestes en cas d’attaque
Formation et matériel à la disposition du public aux USA en cas de fusillade
Transformer le public
« cible molle » et victime
potentielle, en un acteur
de la réponse et de la
résilience
Application pour
• Localiser
• Guider
• Connecter
les volontairesLes fleurs ne suffisent pas … Il faut une réponse médicale forte : • Pour sauver plus de vies • Pour favoriser la résilience
Vous pouvez aussi lire