Infection VHB: actualités + cas cliniques - Dr Karine Lacombe, INSERM UMR-S1136, IPLESP
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous

DESC « Pathologie Infectieuse et Tropicale »
Séminaire 1 – module 1: VIH et hépatites virales B et C
Infection VHB: actualités
+ cas cliniques
Dr Karine Lacombe,
INSERM UMR-S1136, IPLESP
SMIT St Antoine, AP-HP
Université Pierre et Marie Curie, Paris VI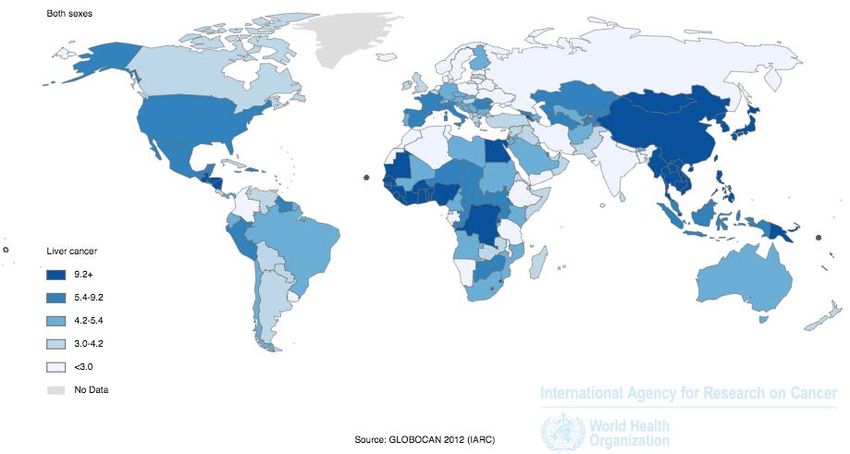
PLAN 1- Eléments d’épidémiologie 2- Histoire naturelle 3- Outils de diagnostic et de suivi 4- Principes thérapeutiques et recommandations de prise en charge 5- Prévention de l’acquisition du VHB 6- Prévention de la transmission du VHB 7- Spécificités de la co-infection avec le VIH
Éléments d’épidémiologie
L’infection VHB dans le monde
• 2 milliards de patients en contact avec le VHB
• 300-400 millions avec infection chronique
• 25%-40% décès par cirrhose ou CHC
– 300 000 cas/an de CHC lié au VHB
– Le VHB est le second carcinogène après le tabac
World Health Organization. Fact sheet. Available at: http://www.who.int. Accessed January 31,
2006. Centers for Disease Control. Fact sheet. Available at: http://www.cdc.gov. Accessed
January 31, 2006. Lai CL, et al. Lancet. 2003;362:2089-2094.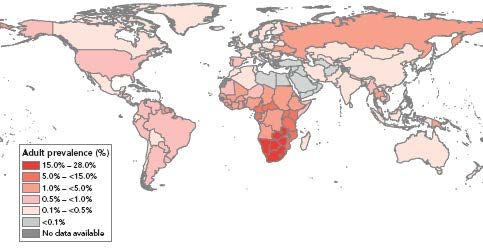
Nombre de décès attribuables, 2010 • « Global Burden of Diseases study »: cirrhose et cancer du foie au rangs 12 et 16 • Si regroupés: « top ten » des causes de décès, avant paludisme et tuberculose Lozzano, Lancet 2012

Incidence des cancers du foie
dans le monde, 2012
(From Globocan 2012 http://globocan.iarc.fr)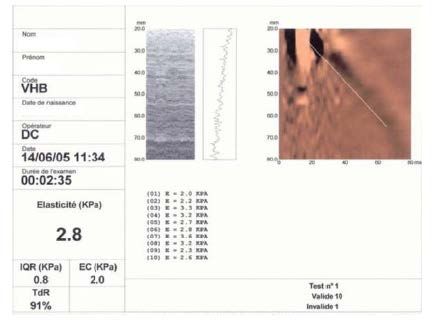
Epidémiologie de la co-infection VIH-VHB
Prévalence globale
Mêmes voies de transmission:
90% des patients VIH+ porteurs de marqueurs VHB (Ac
antiHBc) + 5-15% avec infection chronique (AgHBs+)1
VIH (33M) + VHB (400M) = 2-4M VIH-VHB2
Voies de transmission et âge à la transmission diffèrent
selon l’origine géographique et influencent l’histoire
naturelle du VHB:
HIV prevalence, 2013
Zones à faible endémicité VHB (8%)
- Afrique, Asie
- périnatal, jeune âge (injections, scarification)
- P(VIH-VHB) = 15%
1Alter M. J Hepatol 2006. 2WHO Report, 2013.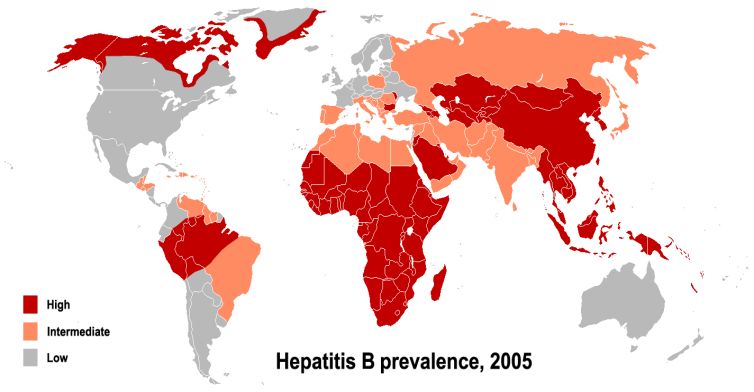
Histoire naturelle
Infection VHB chronique:
une maladie silencieuse
70% asymptomatic
30% symptomatic
Contamination Acute hepatitis 1% fulminant => hepatic transplantation
90-95% 5-10%
HBsAg+
HBsAg -
Cure Anti-HBs+ & HBc+
Chronic infection
70%
Chronic hepatitis 30%
20%
HCC Cirrhosis Inactive carrier
20%
(3-5%/year)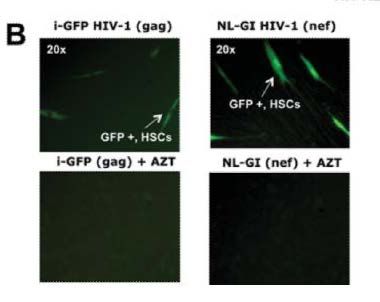
Les quatre phases de
l’infection VHB chronique
AgHBs
AgHBe Anti-HBe
ADN VHB
ALAT (mutants préC)
Immunotolérance Activité phase Immunité
Hepatitis B virus infection. Lee WM. N Engl J Med. 1997 Dec 11;337(24):1733-45.
non-replicativeLes profils VHB
Patient Populations in Chronic Hepatitis B
Immune Inactive HBsAg HBeAg– CHB
Marker HBeAg+ CHB
Tolerant Carrier (Precore Mutant)
HBsAg + + + +
HBeAg + + – –
Anti-HBe – – + +
ALT Normal Normal
HBV DNA (UI/mL) > 107 > 100000 20000
Histology Normal/Mild Active Normal Active
Lai CL, et al. Lancet. 2003:362:2089-2094. Lok AS, et al. Gastroenterology. 2001;120:1828-
1853.Immunotolérance : définition • EASL 2012 Definition: – HBeAg positive (high titer) – Consistently normal ALT (
Immunotolérant: rupture de tolérance
Tolérance %
60%
0 10 20 30 40 50 60 70 mois
Hui et al, Hepatology 2007Phase active (rupture de tolérance)
AgHBs
AgHBe Anti-HBe
ADN VHB
Progression annuelle de fibrose
ALAT (mutants préC)
Immunotolérance Activité phase Immunité
Non-replicative
Hepatitis B virus infection. Lee WM. N Engl J Med. 1997 Dec 11;337(24):1733-45. Dienstag et al, N Engl J Med 99, Hui et al, Hepatology 2007Influence de la charge virale sur
l’incidence de la cirrhose: REVEAL
Cumulative Incidence of Liver Cirrhosis
All Subjects (n=3,582)
40
Baseline HBV DNA level, copies/mL 36.2%
≥106 (n=602)
Cumulative incidence of liver
105–Phase de séro-conversion HBe
AgHBs
AgHBe Anti-HBe
ADN VHB
ALAT (mutants préC)
Immunotolérance Activité phase Immunité
Non-replicative
Hepatitis B virus infection. Lee WM. N Engl J Med. 1997 Dec 11;337(24):1733-45. Dienstag et al, N Engl J Med 99, Hui et al, Hepatology 2007Portage inactif : peu de fibrose
100% 100%
n=56 n=80
50% 50%
0% 0%
Ishak ≤ 2 Ishak > 2 FPortage inactif : évolution
Réactivation (1) Survie (2)
100%
90%
80%Perte de l’Ag HBs chez les porteurs
inactifs: 30 ans de suivi
Country N % with HBsAg cleared
Italy 40 45%
(Gut 2008;57:84)
Taiwan 1965 44.7%
(Hepatol 2007;45:1187)Patients Hbe-: Portage inactif ou
1010
mutants préC?
109
108 Hépatite chronique AgHBe -
107
106
105
104
103
102
10 Portage inactif
Années 1 2 3 4 5Survie des patients VHB
100
Inactive CHB
Survival probability (%)
80
60 HBeAg-/HBV DNA+
or HBeAg reversion
40
HBeAg+ persistence
20
0
0 5 10 15 20 25
Time (years)
Fattovich et al. Gut 2008Risque de CHC en fonction
du statut HBe
REVEAL study: Taiwan 1991−1992; Invited: 47,079 men HBsAg+ HBeAg+ RR 60.2
(30−65 years); Enrolled: 11,893
HBsAg+ HBeAg- RR 13.5
HBsAg- RR 1.0
Yang et al. NEJM 2002Outils de diagnostic et de suivi
Outils de screening (1)
• HBV Elisa tests1:
– Méthode immuno-enzymatique
– Stratégie de dépistage : rechercher en même temps
Ag HBs, Ac antiHBs et Ac antiHBc (méthode la plus
coût-efficace1)
– Si dépistage phase aigue, recherche d’Ac antiHBc
IgM,mais peu fiable
1 HAS Recommandations 2011Outils de screening (2)
• Tests rapides VHB
– Effectués sur plasma ou sang total
– Excellente spécificité: Très peu de faux positifs
– Très bonne sensibilité
– Faux négatifs concernent essentiellement patients
à titre AgHBs et CV VHB faibles, au stade de
portage chronique inactif
Bottero, J Hepatol 2012Outil d’évaluation virologique
• Quantification ADN-VHB
– 2 techniques de biologie moléculaire: : amplification de
cible (PCR) et amplification de signal (branched DNA
assay), avec une augmentation de la sensibilité si PCR
temps réel
– Utilisé pour confirmer le caractère réplicatif du VHB
– Fenêtre sérologique: 1 – 3 semainesScreening pour autres causes
d’hépatite chronique
• VHA (pour vacciner si non immunisé), VHC,
VHD
• Hépatite auto-immune : Ac anti-noyau, anti-
LKM1, anti muscle lisse, antimitochondrie
• NASH: intolérance au glucose, syndrome
métabolique
• Hémochromatose secondaire : ferritine
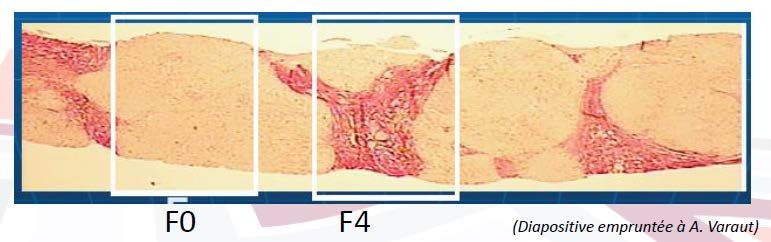
• Vascularite: auto-Ac (PAN)Evaluation de la fibrose hépatique (1)
• Biopsie hépatique
– Considérée comme le « gold standard »
l’évaluation de la fibrose pendant très longtemps
– Encore très importante chez les patients VIH+
(NASH, OH, toxicité ARV, etc.)
– Nombreux inconvénients: coûts, complications
vitales, variabilité d’échantillonÉvaluation de la fibrose hépatique (2)
• Scores biochimiques
– Basés sur la combinaison de marqueurs prédictifs avec une
équation prédisant le risque
– Influencé par étiologie de la fibrose (différent seuils)
- Meilleurs tests: combinaison de marqueurs de la
dégradation de la matrice extracellulaire (Fibrotest,
fibrometre)
- Tests simples comme APRI = très bonne performance dans
la détection de la cirrhose (WHO 2014)Évaluation de la fibrose hépatique (3)
• Elastométrie impulsionnelle
– Mesure de la dureté du foie
(kPa)
– Mediane et IQR avec au moins
10 mesures valides
– Doit être effectué à jeun
– Seuils:
• F2: 7,2
• F3: 9,4
• F4: 14,5Screening des maladies
terminales du foie
• Recherche de complications de cirrhose telles
que le VHC ou la cirrhose décompensée
• Basée sur l’écho doppler / 6 mois
• Dosage αFP = intéressant uniquement chez les
patients VIH+
• Si doute sur nodule hépatique : TDM ou IRM
hépatique
• Gastroscopie pour recherche de VO / 2 ansPrincipes thérapeutiques et recommandations de prise en charge
Objectifs du traitement
• Atteindre une suppression durable de la réplication de
l’ADN-VHB
– Diminution d’au moins > 1 log à 12 semaines
– Indétectabilité à 24 semaines
• Contrôler l’évolution de la maladie hépatique
– normalisation des ALAT
– régression de l’nflammation
– Prevention de la cirrhose et du CHC
– séroconversion HBeAg et HBsAg à long terme ?
AASLD guidelines, Hepatology,2007: 45: 439Développement des traitements
antiVHB
IFN Adefovir Entecavir Tenofovir
1983 2003 2006 2008
Lamivudine Peg IFN Telbivudine
1999 2005 2007Concepts thérapeutiques et VHB
Traitements Traitements
antiviraux immunomodulateurs
Lamivudine Interféron-α
Adefovir Vaccinothérapie
Entecavir
Transfert passif
Tenofovir
d'immunité
Telbivudine
Immunostimulation
Thymosine
GM-CSF
Polyadenur
Interleukine 12Concepts thérapeutiques et VHB
Traitements Traitements
antiviraux immunomodulateurs
« Add on »
Nuc+ PEG:
« un peu
Lamivudine
« Add on » inefficace » Interféron-α
Adefovir Vaccinothérapie
de Nuc: Inefficace
Entecavir
presqu’ Transfert passif
Tenofovir
inefficace Restreint à
d'immunité
Telbivudine l’allogreffe
de moëlle Immunostimulation
Thymosine
GM-CSF
Inefficaces
Polyadenur
Interleukine 12Recommandations thérapeutiques
Traitements
antiviraux
Lamivudine Interféron-α
Adefovir
Entecavir
Tenofovir
Telbivudine - A>1 F>1
- ADN VHB > 2000 UI/mL
&/ou ALT aN
European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of chronic hepatitis
B virus infection. J Hepatol. 2012;57:167–85.IFN PEG alpha 2a dans l’Hep B AgHBe+
Efficacité 6 mois après l’arrêt du traitement
80
60
41%
Malades (%)
40
32% 32%
20 14%
3%
0
ALAT N Seroconv ADN VHB ADN VHB- AgHBs-
HBe < 100 000 PCR
Lau et al. NEJM 2005IFN PEG alpha 2a dans l’Hep B AgHBe-
Efficacité 6 mois après l’arrêt du traitement
80
59%
60
42%
Malades (%)
40
20 17%
4%
0
ALAT N ADN VHB ADN VHB- AgHBs-
< 20 000 PCR
Marcellin et al. NEJM 2004Réponse virologique sous ETV
(Virgil cohort)
•Virological response was 99%
estimated by KM analysis 100
in 243 NA-naïve patients HBeAg-negative P< 90%
89% 0.001
80
•Virological response was
defined as HBV DNANucs (Tenofovir): suivi à 4 ans
100 On-Treatment Analysis 99%
96%
90
80
TDF-TDF
70
Percentage %
ADV-TDF
60
n=266
50
40
On/After week 72, patients with confirmed HBV DNA ≥400 copies/mL were eligible
to add FTC in a fixed dose combination tablet
30 Randomized
Double-blind 39 patients who were eligible to add FTC, 34 added and 5 did not
20
10
Open-label TDF
0
0 4 8 12 16 20 24 28 32 36 40 44 48 56 64 72 80 88 96 108 120 132 144 156 168 180 192
*HBV DNA < 400 copies/mL Weeks on Study
Illustration includes 19 patients who added FTC and had HBV DNACombinaison ETV + TDF en cas d’échec
HBV DNA Viremia Undetectable HBV DNA
1011
1
1010
HBV DNA [IU/ml]
1009 Δ 3 log10 c/mL reduction 0.8
1008 P=0.0001
1007 0.6
1006
1005
1004 0.4 Entire cohort (N=52)
1003 LLoD
1002 0.2 ADV resistance (n=18)
10 6
0
Baseline 3 6 9 12 15 18 21 24 0 3 6 9 12 15 18
Months Time (months)
LLoD=Lower Limit of Detection
Rescue therapy with ETV + TDF in CHB patients with advanced liver disease and complex viral resistance
patterns or showing partial antiviral responses to preceeding therapies (Virgil network)
Petersen J, et al. J Hepatol 2012.Le choix entre interféron et Nucs
Undetectable HBV DNA Over Time in HBeAg-
Negative Patients
Not head-to-head trials; different patient populations and trial designs
Extended Treatment With Nucleos(t)ide Analogues vs
Limited Duration (1 Yr) Peginterferon Treatment
100 93 96 100*
90 91 87
Undetectable HBV DNA (%)
80 Entecavir
63 Tenofovir
60 Peginterferon
40
20 15 16
NA
0
*Single center study. 1 Yr 2 Yrs 3 Yrs
Lok AS, et al. Hepatology. 2009;50:661-662. Marcellin P, et al. AASLD 2008. Abstract 146. Marcellin P, et al. AASLD 2009. Abstract 481.
Marcellin P, et al. Gastroenterology. 2009;136:2169-2179. Baqai S, et al. AASLD 2009. Abstract 476. Lai CL,
et al. Hong Kong International Liver Congress 2006.Tolérance des Nucs (1)
ETV has a generally favourable open-label safety
100
profile up to 380 Weeks* (n=1051)
80
Proportion of subjects (%)
Median ETV exposure 184 ± 2.8 weeks (range: 1.9–380 weeks)
60
40
20 14
4
1 1
0
Drug-related Discontinuation due Confirmed creatinine Grade 3–4 lipase
Grade 3–4 AEs to AEs increase (>0.5 mg/dL from elevation
baseline)
Adverse events
*49% patients enrolled in ETV-901 had >5 years total ETV treatment (including treatment time in parent protocols).
Patients in the ETV-901 rollover study received 1-mg ETV.
1. Adapted from Manns M, et al. 45th EASL, 2010. Poster 1016. http://www.natap.org/2010/EASL/EASL_39.htm [Accessed Mar. 2011].Tolérance des Nucs (2)
100
TDF has a generally favourable clinical trial safety
profile up to 192 Weeks*
80
Proportion of subjects (%)
HBeAg–ve: TDF-TDF (n=235) HBeAg–ve: ADV-TDF (n=112)
60 HBeAg+ve: TDF-TDF (n=154) HBeAg+ve:ADV-TDF (n=84)
40
20 15 16 16 17
1 2 2 1Clinical Focus: Impact of HBV Therapy on Liver Fibrosis/Cirrhosis
clinicaloptions.com/hepatitis
Successful Hepatitis B Treatment Reduces
Clinical Endpoints
HBV suppression with nucleos(t)ide analogue therapy reduces risk of hepatic
decompensation and HCC in pts with advanced fibrosis or cirrhosis[6]
25
Pts With Disease Progression (%)
n = 43
20 Placebo
15 P = .001
n = 173
10 Lamivudine
n = 198 n = 122
5 n = 385
n = 417
0
0 6 12 18 24 30 36
Kaplan-Meier Estimate of Time to Disease Progression in Asians With CHB (Mos)
6. Liaw YF, et al. N Engl J Med. 2004;351:1521-1531.Clinical Focus: Impact of HBV Therapy on Liver Fibrosis/Cirrhosis
clinicaloptions.com/hepatitis
96% of Pts Treated With Tenofovir Had
Stable or Improved Fibrosis at Yr 5
Pts with Ishak score ≥ 4: 38% at baseline, 12% at Yr 5
Pts with cirrhosis (Ishak score ≥ 5): 28% at baseline, 8% at Yr 5 (n=96)
P < .001
P < .001 Ishak Fibrosis
100 Scores
12% 6
80 38% 5
Patients (%)
4
60
3
40 2
63% 1
20 39% 0
0
Baseline Yr 1 Yr 5
N = 348 matched biopsies
17. Marcellin P, et al. Lancet. 2013;381:468-475.Clinical Focus: Impact of HBV Therapy on Liver Fibrosis/Cirrhosis
clinicaloptions.com/hepatitis
All Patients Treated With Long-term
Entecavir Had Stable or Improved Fibrosis
All patients with advanced fibrosis/cirrhosis (Ishak fibrosis score ≥ 4) at
baseline demonstrated at least a 1-point reduction (median change: -1.5)
Subjects with baseline advanced fibrosis/cirrhosis n = 10
60 Ishak Fibrosis Score
6
50 5
Patients (n)
40 4
3
30
2
20
1
10 0
0 Missing
Baseline Wk 48 Long
Term
N = 57 matched biopsies
27. Chang TT, et al. Hepatology. 2010;52:886-893.Indications thérapeutiques
au cours du VHB chronique
• Obtenir un bénéfice clinique par une viro-suppression optimale
au cours des hépatopathies au moins A2 F2 et/ou
aux transaminases élevées et/ou
ayant une charge virale > 2000 UI/mL*
• Ne pas traiter:
- les immuno-tolérants
- les porteurs inactifs (sans infection par un mutant pré-C aux
anomalies fluctuantes)
- les hépatites chroniques « minimes »
• Situations particulières:
-Traitements pré-emptifs
- Prévention de la TMI in utero * CPG EASL J Hepatol 2012Premières lignes thérapeutiques
• Young patients with
– Low viral load
– Limited to moderate fibrosis
– Increased ALT levels
– Genotype A Pegylated IFN
• Older patients or
cirrhotics (compensated or not)
dialysis patients or kidney recipients
severe reactivations or cholestatic fibrosis
pre-emptive therapies
Analogues
Lamivudine, adefovir, entecavir, tenofovir, telbivudine
CPG EASL J Hepatol 2012Prévention de la transmission du VHB
Vaccination anti-VHB (1)
Recommandations de vaccination:
• chez les personnes exposées non immunisées et après dépistage :
- personnes nées, ayant résidé ou étant amenées à résider dans des pays ou zones à risque
d’exposition au VHB;
- entourage d’une personne présentant une infection à VHB (famille vivant sous le même toit) ;
- partenaires sexuels d’une personne présentant une infection à VHB ;
- patients susceptibles de recevoir des transfusions massives et/ou itératives (hémophiles,
dialysés, insuffisants rénaux, candidats à une greffe d’organe, etc.) ;
- usagers de drogues par voie intraveineuse ou intra-nasale ;
- personnes qui séjournent ou ont séjourné en milieu carcéral ;
- personnes séropositives pour le VIH, le VHC ou avec une IST en cours ou récente ;
- personnes ayant des relations sexuelles avec des partenaires différents ;
- adultes accueillis dans les institutions psychiatriques ;
- personnes adeptes du tatouage avec effraction cutanée ou du piercing (à l’exception du perçage
d’oreille) ;
- voyageurs dans les pays ou zones à risque d’exposition au VHB (risque à évaluer au cas par cas)
• chez les personnes qui, dans le cadre d’activités professionnelles ou bénévoles, sont susceptibles d’être en
contact direct avec des patients et/ou d’être exposées au sang et autres produits biologiques,Vaccination anti-VHB (2)
• Vaccin recombinant adsorbé
• Schéma classique: J0, M1 et M6
• Possibilité de schéma accéléré: 3 injections en
21 jours + rappel à 1 an
• Pour personnel exposé au risque d’infection,
immunisation obligatoire
– Si production d’une sérologie même ancienne
avec Ac antiHBs > 100UI, pas de dosage ultérieur
ni rappelPrévention de la transmission
marterno-foetale du VHB
• Recommandations: associer HBIg +séro-
vaccination à la naissance chez les enfants nés de
mères AgHBs+
• Mais risque résiduel de transmission du VHB
d’autant plus important que l’ADN-VHB est élevé
• Essais d’efficacité de la lamivudine comme moyen
de PTME-VHB: en faveur du traitement en Asie
• Essais en cours sur l’intérêt d’utiliser le TDF
(Thaïlande)
• Autre moyen: s’assurer de la vaccination à la
naissance et pas seulement à S6 dans le cadre du
PEV…« Treatment as prevention » du VHB
Cohorte VIH Amsterdam, 2942
patients1
871 « HBV susceptible »
35 infections VHB au cours du
suivi
Traiter des patients
susceptibles par TDF a prévenu
l’infection aigue
Mêmes résultats dans une
autre étude Gatanaga2
Le TDF peut-il être utilisé comme moyen de prévention du VHB ?
1Heuft M, et al. CROI 2013. 2Gatanaga, Clin Infect Dis 2013Prévention de la réactivation du VHB
Qu’est-ce que la réactivation ?
AgHBs+, AgHBe+ AcHBe- (sauvage)
UI/ml 108
CV Elevées Immunotolérance
107
AgHBs+, AgHBe+ AcHBe- (sauvage)
106 AgHBs+, AgHBe- AcHBe+ (mutant)
CV Intermédiaires
105
Immunoélimination
104 Réactivation
AgHBs+, AgHBe- AcHBe+
103
CV Basses
Portage inactif
102
AgHBs-, AcHBc+, AcHBs+
10 CV Indétectables AcHBc+, AcHBs-
“Guérison”
Yim et al. Hepatology1 2006Quand observe-t-on
une réactivation virale B ?
Spontanée Arrêt du traitement Déficit immunitaire
(compliance)
Iatrogène : Pathologique :
• Chimiothérapie • VIH
• Greffe d’organes • DICV
• Immunosuppression • Autres troubles
(corticoïdes, AC MC) acquis…Facteurs de risque de réactivation
Facteurs Ag HBs positif Ag HBs négatif
Lié à l’hôte • Lymphome
• Maladie hématologique
• Hémopathie maligne
• Greffe de moelle ou cellules
• Pathologie hépatique souches
préexistante
• Age jeune
• Sexe masculin
Lié au virus • Charge virale élevée
• Statut Ag HBe positif
• Présence d’ac Anti HBc
• Baisse des ac Anti HBs ?
Lié au traitement • Dose élevée de • Rituximab
chimiothérapie
• Corticothérapie
En pratique, toute modification du statut immunitaire d’un porteur
chronique du VHB (Cushing, switch d’immunosuppression) ou forte
immunosuppression d’un sujet exposé au VHB justifie un traitement
pré-emptifTraitement pré-emptif
et recommandations EASL
Surveillance
Traitement pré-emptif par tout analogue, ALAT et
au mieuxTénofovir ou Entecavir sérologie VHB
AgHBs – et AgHBs – et
AgHBs + et AgHBs + et
Ac antiHBs – et Ac antiHBs + et
ADN-VHB + ADN-VHB –
Ac antiHBc + Ac antiHBc +
Risque de réactivation
CPG EASL. J Hepatol 2012Le Ténofovir réduit la mortalité des
patients avec réactivation virale B
• Étude contrôlée randomisée :
27 patients avec une réactivation virale aiguë sévère ++ du VHB :
Ténofovir : 14 patients ; placebo : 13 patients
Réduction de l’ADN VHB Survie en fonction de la réduction
de l’ADN VHB à S2 sous TDF
J0 J15 J90 Décès Vivants
p = 0,01
10 10
ADN VHB (Log médian)
p = 0,001
Nombre de patients
8 8
p = 0,01 p = 0,003
6 6 Vivants = 8/9
Vivants = 0 (89 %)
4 7
6,64 4
6,81
Décès = 5/5
2 4,22 4,07 2 (100 %)
3,04
Décès = 1/9 (11 %)
0
Placebo Ténofovir < 2 log > 2 log
Hitendra K.et al. AASLD 2009 , Abstract 11Spécificités de la co-infection VIH-VHB
HBV in HIV patients:
the continuum of care
Prevention
Hepatitis Natural/cART
Treatment Delta history
DiagnosisEfficacy of
immunization ?
Isolated
HBcAb ?
Prevention
Hepatitis Natural/cART
Treatment Delta history
DiagnosisHBV immunization in HIV
• Unsufficient HBV vaccine coverage and
vaccine response1:
- 32% of eligible patients were vaccinated
- in those with one injection, immunization
course completed in 57%
- achivement of protective Ab titer in 37%
1Tedaldi EM, Clin Infect Dis 2004Increasing HBV immunization
2 options:
• increasing the dosing (40µg instead of 20µg)
• increasing the number of injections (4 instead of 3)
Confirmed by a meta-analysis of
5 trials (883 patients):
OR = 1,82 (1,47 – 2,61) of higher
HBsAb titer in 4-doses v. 3-doses
schedule
Ni JD, et al. Int J STD AIDS 2013
Launay O. et al, JAMA 2011Management of isolated HBcAb
SHOULD WE TREAT? SHOULD WE IMMUNIZE?
• Frequency of occult HBV • In 40 patients vaccinated with
1 to 6 vaccine doses4:
differing regarding – anamnestic response: 32%
geographical origin:Prevention Liver
outcomes?
Hepatitis Natural/cART
Treatment Delta history
Diagnosis OLT?HBV infection and mortality risk (1)
multicenter cohort + meta-
analysis of 12 382 patients,
either HIV+ or HIV/HBV
36% excess risk of dying (all
cause) if HBs pos. compared
to HBs neg.
Higher mortality risk in HIV-HBV compared to HIV patients
between 1992 and 2007
Nikolopoulos G, Clin Infect Dis 2009HBV infection and mortality risk (2)
MACS cohort: (337HBs+ - 343
HCV+) of whom 452 HIV+ 6728
person-years of F/U, 293 deaths
RR=2,2 [1,1 – 4,5] of dying of liver-related cause when HBs pos. V. HCV pos.
No difference between HCV and HBV regarding all cause deaths
Falade-Nwulia O, et al. Clin Infect Dis 2012Rôle intriqué du VIH et du VHB (1)
• Tropisme VIH pour les HSC et les hépatocytes
– Effet cytopathique direct du VIH sur le tissu hépatique par fixation
aux co-récepteurs CCR5 et CXCR4 exprimés à la surface des
hépatocytes et des HSC, et déclenchement de l’apoptose
cellulaire1
– Infection des HSC par les récepteurs CCR5 et promotion de la
differenciation myofibroblastique, conduisant à l’accélération du
processus fibrosant2
1Babu CK, PLoS One 2009. 2Tuyama A. Hepatology 2010Rôle intriqué du VIH et du VHB (2)
• Altération de la réponse immune innée et adaptative
(VHB)
– Réponse immune suboptimale dans le contexte du VIH (
frequence de séroconversion HBs and HBe)
• Dégradation de la réponse T CD8+ anti-VHBévolution chronique3
– Origine multifactorielle:
• Modification de l’expression des TLRs ( pathogen-recognition
receptors) par le VIH1 et le VHB2 cascade de signalisation por-
infammatoire fibrose
1Thibault S, Rettrovirology 2009. 2Jun W, Hepatology 2009. 3Chang JJ, J Virol 2009Impact of cART on
liver-related deaths
• Eurosida cohort: 12069
patients included in
analysis
Kowalska, et al. AIDS 2012Clinical outcomes in the era of cART
• 92 patients, 82% treated with FTC/TDFmedian f/u=39 months1
• I(death): 2,2 / 100 p.y
• I(liver dec.) 2,9 / 100 p.y
Close to what is observed in HIV general
population
• liver fibrosis stability in 75% of patients
Martin-Carbonero, et al. AIDS 2011Survival rate in transplanted patients:
data from France
• 13 patients (1HDV+, 2 HCV+, 4 HCV-HDV+)
• Indication for OLT: decompensated cirrhosis (10) and
HCC (3)
• Treatment after OLT: combination of TDF / 3TC + HBIg
• Overall survival rate at 32months: 100%
– No mitochondrial toxicity
– Controled HBV-DNA, HDV-RNA, HIV-RNA
– Successful treatment with PR in 1/3 HCV-RNA+
Tatteo, et al. AIDS 2009Survival rate in transplanted patients:
data from the USA
• 22 patients (2 HCV+) matched with 20 HBV mono-
infected patients
• Indication for OLT: decompensated cirrhosis (19),
HCC (2), fulminant (1)
• Overall survival: 85% in HIV-HBV, 100% in HBV
(p=0,09)
– 3 deaths due to causes unrelated to HBV
– Persistent low replicating HBV-DNA in 6/7patients with
available HBV-DNA after OLT
Coffin, et al. Am J Transplant, 2010Prevention
Hepatitis Natural/cART
Treatment Delta history
Diagnosis/
evaluation
Rapid
Fibrosis ?
tests?Increasing screening in HIV patients
120
100
80 * * *
60
*
* 2005
2008
*
40
2012
20
0
EPI-B studies, 2005, 2008, 2012 (AIDS 2007, Liver Int 2012)Can rapid tests increase
screening efficacy (1)?
Performance of 3 HBsAg rapid tests on capillar blood in the community1
In African rural settings2, performance of Determine test:
Se=96% / Sp=100%
Are rapid tests reliable in the HIV settings?
- YES3 κ correlation coefficient = 1 / Se=100% and
Sp=100% in study done in Liverpool on 300 sera from HIV+
patients from Malawi (CD4 = 175)
1Bottero J, et al. J Hepatol 2013. 2Franseck FC, et al. PlosOne 2013. 3Davies J, et al. Trans R Soc Med Hyg 2010Can rapid tests increase
screening efficacy (2)?
Rapid tests Elisa tests
163 Patients included 162
163 Tests performed 115
163 Results deliveres 104
18/20 Pos. Patients starting F/U 15/18
AND patients knowing their status
+ 143/143 + 89/144
98,8% Optimal management 62,4%
Bottero et al. EASL 2014Non invasive Fibrosis Evaluation:
still challenging
134 patients, 11 scores tested1 57 patients, elastmetry2
scores AUC Cut-offs (HCV)
Fibrometer®
-≤ F2 0,74 0,46 0,5
- ≤ F3 0,83 0,69
- F4 0,89 0,83
Fibrotest®
-≤ F2 0,77 0,43 0,49
- ≤ F3 0,80 0,59 0,59
- F4 0,87 0,74 0,75
1Bottero J. J Hepatol, 2009. 2Miailhes P. J Viral Hepat 2010Persistence of
low replication?
Prevention
Hepatitis Natural/cART
Impact? Treatment Delta history
Tolerance
(bone, kidney)?
DiagnosisTreatment algorithms EACS Guidelines Nov 2014
Treatment efficacy with TDF
• 102 patients (61% HBeAg+) with a • 120 patients (63% HBeAg +) with a minimum
median 5 years of follow-up of 1 year of TDF and a median 6 years (3 – 8) of
follow-up
1.00
Cumulative probability HBV-VLRole of Peg-IFN in TDF-treated patients
EMVIPEG: pilot study evaluating the addition of Peg-IFN to TDF in HIV-HBV
patients 1
No benefit of adding Peg-IFN regarding antiHBe seroconversion or
HBs loss rate
1 Miailhes P, et al. J Hepatol 2014Persistent HBV replication
• MAGNITUDE: 5 to 10% of patients on TDF after > 3 years1,2
• PATTERNS: blips, persistent viremia, rebound2,3
• CAUSES: - suboptimal adherence: YES2,3
- suboptimal treatment: NO4 (maybe in pre-treated patients)3
- resistant strains: NO2,3,5
- failing immunological control?
• IMPACT: - no Hbe or HBs loss in patients w/ persistent replication, no
clinical event6
• MANAGEMENT: - confliting results regarding addition of ETV7,8,9
- check adherence10
- stay on same therapy if regular decrease > 1 year10
- add ETV only long-term stagnation of HBV-DNA 10
- reconsider after 6 months10
1de Vriis Sluijt 2010. 2Boyd 2009. 3Matthews 2013. 4Matthews 2008. 5Childs, AIDS 2013. 6Boyd, Hepatology 2014.
7Luetkemeyer, JAIDS 2011. 8Ratcliffe, AIDS 2011. 9Mikulska, J Med Virol 2012. 10EACS/EASL Guidelines 2012 and 2013Long term tolerance of TDF
Figure 1: MDRD clearance over time
120.00
240 patients with a 3year-time follow-up, normal
MDRD Creatinine Clearance (mL/min)
110.00 eGFR at baseline1: no difference with other NUC
100.00
Available data on renal and bone impairment over
time in HIV-infected patients on long-term use of
90.00
TDF (> 6 years)
80.00 TDF- associated tubular nephropathy very rarely
described in HBV-infected patients2,3
0 6 12 18 24 30 36
Duration of treatment (months)
NRTI-based therapy
with TDF without TDF
MANAGEMENT:
• Check the imputability of TDF in alteration of renal Cl. (send to kidney specialist
and biopsy)
• Decrease TDF dosage(1cp/2-3 days)
• No place for ADV
• Add probenecide ?
• Switch for ETV if no previous exposure to 3TC?
1Lacombe K, EASL 2008. 2Si-Ahmed SN, Antiviral Res 2011. 3Gish RG, Clin Gastroenterol Hepatol 2012Emergence of treatment
and immune escape mutants
% of patients with incident
mutations
numerous
TDF±LAM/FTC switchs
Groups of mutations % (n) % (n)
Alkyl phosphonate-associated pol-gene (n=49) (n=15)
6.1% 6.7%
Immune-associated S-gene (n=73) (n=18)
1.4% 5.6%
L-nucleoside-associated pol- (n=64) (n=15)
gene/antiviral-associated S-gene 9.4% 33.3%
Emergence of antiviral-associated S mutations conferring
resistance to current NUCs and potential vaccine escape strains1
Lacombe K, Hepatology 2013Prevention
Hepatitis Natural/cART
Treatment Delta history
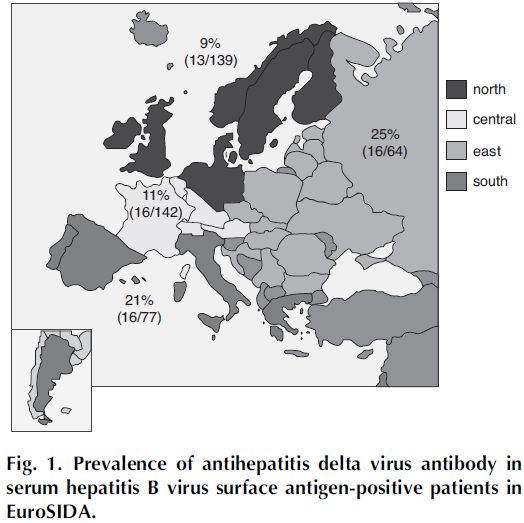
DiagnosisPrevalence of HDV markers in HIV
Manesis EK. EASL Monothematic Conference
Delta Hepatitis. Sept 2010. Istanbul
Soriano V. et al. AIDS 2011
P(HDV/HIV-HBV) = x2 (P(HDV/HBV)Increased fibrosis in
HDV-infected patients
Predictors of clinical outcomes in HDV-
Risk of liver fibrosis ≥ F3
infected patients, EUROSIDA
12
OR = 7,73 OR = 8,54 Clinical outcomes IRR (95%CI)
10
Progression to death 2,23 (1,17-4,28)
8
Progression to liver related 4,44 (1,46-13,55)
6 events
4 Progression to AIDS 1,60 (0,56-4,56)
OR = 1 OR = 1,76
2 Progression to AIDS or death 2,17 (1,22-3,87)
0
HIV-HBV HIV-HBV- HIV-HBV- HIV-HBV-
HCV HDV HCV-HDV
Lacombe K, et al. AIDS 2007 Soriano V, et al. AIDS 2011Treatment options for HDV in HIV
Persistent HDV-DNA replication in all 17 patients
(including those treated with Peg-IFN + TDF after Peg-
IFN interruption
Sequential treatment with Peg-IFN ? (normalisation of
transaminases, stabilization of liver fibrosis?)
Boyd A, et al. AIDS Res Hum Retroviruses 2013Prevention
Hepatitis Natural/cART
Treatment Delta history
Diagnosis
Future:
Can we think of cure?HBs loss with current treatment
Studies Duration of F/U Hbe loss HBs loss
Treatment experienced
De Vriis Sluijt, 2010 (n=102) 5 years 46% 12%
Maylin, 2013 (n=143, Hbe+=67%) 3 years 43% 4%
Treatment naive
Matthews, 2013 (n=47, Hbe+=57%) 2 years 48% 13%
HBs loss is low with NUCs, HBs
seroconversion is even lower…
Maylin S. AIDS 2012New therapeutic strategies
Drugs targeting virus or host1
New targets for « functional cure »2
1Zoulim F, Expert Opin Emerg Drugs 2013. 2Zoulim F. Antivir Res 2012Vous pouvez aussi lire