COVID-19 ET THROMBOEMBOLIE VEINEUSE JEUDI 18 JUIN 2020 - Dr PIERRE LA ROCHELLE - AMUQ
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous
COVID-19
ET THROMBOEMBOLIE
VEINEUSE
Dr PIERRE LA ROCHELLE
JEUDI 18 JUIN 2020
2020-06-18
COVID-19 et thromboembolie veineuse
Visioconférence du Dr Pierre La Rochelle
Jeudi 18 juin 2020, 20 h à 21 h
1
Vous avez des questions ? Vous pouvez :
• Ouvrir la fenêtre de clavardage pour poser une question écrite
ou ;
• Utiliser la fenêtre « Q&A ».
SURVEILLEZ VOS COURRIELS :
Vous en recevrez un pour évaluer la visioconférence.
2
1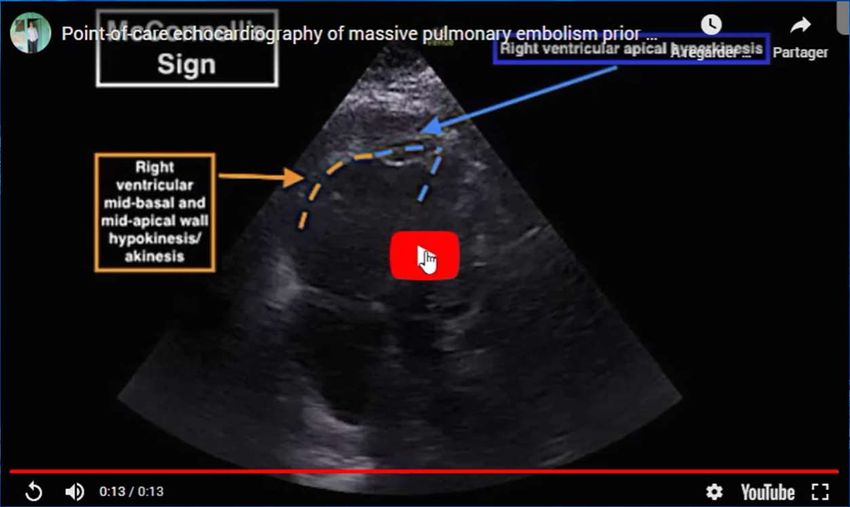
2020-06-18
Déclaration de conflits d’intérêts potentiels
Auteur du guide de l’INESSS sur l’anticoagulothérapie
orale
Auteur guide du diagnostic et prise en charge de l’embolie
pulmonaire de l’AMUQ
3
Gestion des conflits d’intérêts potentiels
Tous les honoraires des conférencières et des conférenciers
sont assumés par
l’Association des médecins d’urgence du Québec (AMUQ).
Le contenu de la présentation a été validé et approuvé
par le comité scientifique de l’activité.
Le comité scientifique de l’AMUQ applique une procédure afin
d’éviter
toute situation de conflits d’intérêts réels, potentiels ou apparents
et pour éviter toute apparence d’ingérence d’un commanditaire
dans le contenu scientifique de ses activités de DPC.
4
2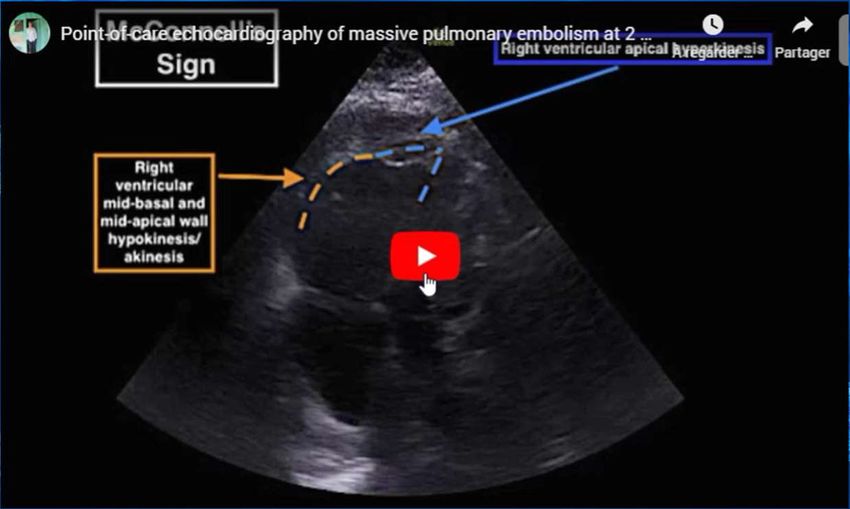
2020-06-18
Objectifs
▸ 1. Identifier les preuves dans la littérature scientifique de la prévalence de
la MTE chez les patients atteint de la COVID-19
▸ 2. Discuter de l’investigation de la MTE chez les patients atteints de la
COVID-19
▸ 3. Décrire les préventions de la MTE possible chez les patients COVID-19
hospitalisés
5
5
Physiopathologie
▸ Perturbation du bilan sanguin
▹ CRP élevée
▹ Lymphocytopénie
▹ Légère thrombocytopénie
▹ Temps de prothrombine prolongée
▹ D-dimers élevés
▹ Fibrinogène élevé au début
6
6
3
2020-06-18
Les D-dimers et le COVID-19
▸ Bon marqueur pronostic en cours
d’hospitalisation, Wuhan Chine
▸ Bon prédicteur de mortalité à
l’admission, pour un seuil de D-
dimers à 2000 HR:51.5,
(95%CI:12.9-206.7; P
2020-06-18
Association COVID-19 et TEV
▸ Autopsies prospectives de 12 patients décédés de COVID-
19 (Allemagne, 52 à 87 ans, 8 hommes 5 femmes, 10
hospitalisés) [3]
▸ 7 sur 12 présentaient une EP
▸ 4 sur 12 cause directe du décès
▸ Autopsies 10 patients décédés du COVID-19 au Brésil
(biopsies transthoraciques) [4]
▹ 5 hommes, 5 femmes, de 33 à 83 ans
▹ 8 sur 10 présentaient des micro-thrombis 9
9
Association COVID-19 et TEV
▸ Autopsies prospectives de 80 premiers patients décédés de COVID-19
(Hambourg Allemagne, 52 à 96 ans, 46 hommes/34 femmes, 51
hospitalisés(17 USI, 36 étages)/13 résidences personnes âgées/12
maison/1 hôtel) [3.1]
▸ Dans 8 cas la pneumonie était accompagnée d’une EP fulminante
▸ 9 autres cas avaient des EP périphériques
▸ Autopsies 10 afro-américains New-Orleans USA,
10/10 avaint des petits thrombus dans les artères pulmonaires
10
10
5
2020-06-18
Question 1
▸ Quel rôle les D-dimers peuvent jouer dans le diagnostic de la
MTE
▹ A) en éliminant les patient avec un D-dimer bas (ex < 500)
▹ B) en établissant un seuil pour une investigation
systématique
▹ C) ne peuvent n’être utilisés d’aucune manière
▹ D) peuvent apporter une aide globale à la décision
11
11
Angioscan pulmonaire et D-dimers
COVID-19 Non COVID-19
Angioscan Angioscan D-dimers D-dimers
positif négatif EP pas EP
Poyiadi, 72 (22%) 256 9330 2540 6 (11%) 48
(USA) [7]
Léonard- 32 (30%) 74 15359 1940
Laurent
(France) [6]
Helms, 25 (25%) 75
(France) [5]
12
12
6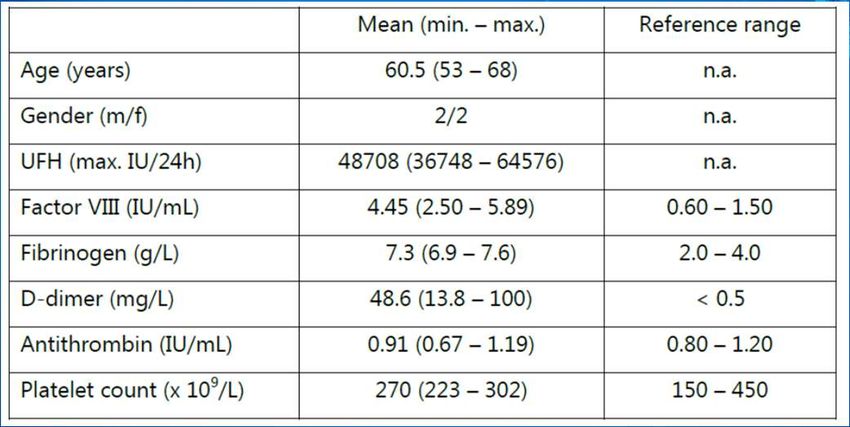
2020-06-18
[6]
[25]
13
13
[27]
14
14
7
2020-06-18
Question 2
▸ Une thromboprophylaxie exclut à toutes fins pratiques une
MTE
▹ A) vrai
▹ B) faux
15
Anticoagulation et TEV dans les USI
Thérapeutique Prophylactique Hémorragies Décès
Klok, (Pays-Bas) [8] 3/17 (18%) 65/167 (39%) 41/184 (22%)
Helms, ARDS 45 105 4/150 (3%) 13/150 (9%)
(France) [5]
27 TEVs/150 (18%)
Middledrop, (Pays- 0/7 (0%) 35/68 (51%) 14/75 (19%)
Bas) [9]
Llitjios, ventilation 10/18 (56%) 8/8 (100%) 3/18 (17%)
mécanique (France)
[10]
Lodigiani, (Italie) [11] 0/2 (0%) 4/59 (7%)
Thomas, (Royaume- 6/63 (10%) 10/63 (16%)
Uni) [13]
Ren, (Chine) [12] 40/47 (85%) 15/48 (31%)
DVT screening
In epidemiological studies, the incidence of VTE was three- to four-fold lower in Chinese compared to Caucasian 16
individuals, while the VTE risk in African Americans appears to be higher than that in Caucasians [13,1]
16
8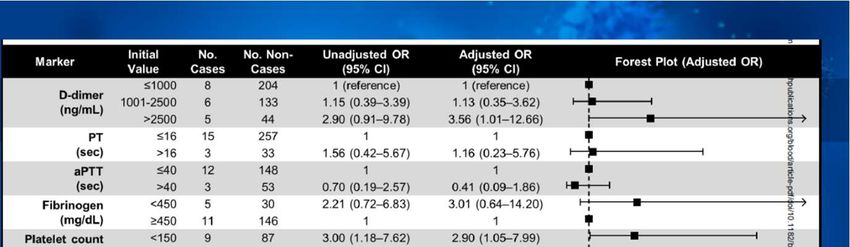
2020-06-18
Question 3
▸ Quel serait le site hémorragique le plus fréquent
des patients hospitalisés pour la COVID-19?
▹ A) pulmonaire
▹ B) cérébral
▹ C) ORL
▹ D) gastro-intestinal
▹ E) rétropéritonéal 17
17
COVID-19 et risque hémorragique
▸ Risque mal documenté à ce jour
▹ CS Thaïlande, 41 cas non détaillés, aucun décès [17]
▹ CS 2 hémorragies digestives sous HFPM(1 prophylactique, 1
thérapeutique) embolisées, aucun décès [14]
▹ CS hémorragies cérébrales patients sous ECMO [16]
▹ CS Italie, 4 hémorragies nécessitant une embolisation, 3 sous HFPM,
aucun décès [15]
18
18
92020-06-18
COVID-19 et risque hémorragique
▹ RCS: 19 (4,8%) pts saignement /400 pts hospitalisés, [28]
▹ 5 thérapeutiques/9 prophylactiques, 2 warfarine, 1 clopidogrel, 1 nil
▹ 9 sévères/ 10 non sévères
▹ Site le plus fréquent: 8 G-I dont 5 des 9 sévères
▹ 4 cas de plaquettes < 50 000 x 109 , 1 cas < 25 000 x 109
19
19
[28]
20
20
102020-06-18
[31]
21
21
Résistance à l’héparine [24]
▸ 69 pts COVID-19 admis USI, UK
▸ 15 pts avec anticoagulation thérapeutique
▹ 5 pts HFPM (daltéparine) (4 PE, 1 Line thrombosis)
▹ Activité anti-Xa sous optimale 5/5
▹ 10 pts perf héparine (9 hemofiltration clotting, 1 PE)
8 pts perf > 35 000/jr (critère)
3 pts perf > 50 000/jr
22
22
112020-06-18
4 cas avec résistance à l’héparine / 75
cas de COVID-19 avec TEV aux USI [26]
23
23
24
24
122020-06-18
COVID-19 and Thrombotic or Thromboembolic
Disease: Implications for Prevention,
Antithrombotic Therapy, and Follow-up
JACC 2020 [20]
▸ Index of suspicion VTE should be high in the case
typical DVT symptoms, hypoxemia disproportionate to
known respiratory pathologies, or acute unexplained
right ventricular dysfunction
25
25
ISTH interim guidance
[19]
26
26
132020-06-18
Diagnostic de la TEV
▸ Pas d’investigation de routine basée sur les D-dimers (ACC,
ISTH)
▸ L’angioscan pulmonaire et la scintigraphie V/Q sont limitées
par les risques de contagiosité et/ou l’instabilité des patients,
la position ventrale
▸ Le doppler veineux des 2 MIs, POCUS (ETT ou ETO) (Fonction
ventriculaire droite, caillots) peuvent, en partie, suppléer
27
27
Diagnostic de la TEV
▸ Diagnostic empirique de TEV ??? À éviter mais …
▹ Cas d’exception, suspicion de TEV élevée, risque
d’anticoagulation faible, investigation pas ou très
difficilement accessible (ex ASH COVID-19 and Pulmonary
Embolism: Frequently Asked Questions (Version 2.0; last updated
May 18, 2020)
▹ Anticoagulation thérapeutique minimale de 3 mois
https://www.hematology.org/search-
results#?cludoquery=covid&cludopage=1&cludorefurl=https%3A%2F%2Fwww.hematology.org%2Feducation&cl
udorefpt=Education%20-%20Hematology.org 28
28
142020-06-18
29
29
Dysfonction ventriculaire droite
(1 USI New-York) [21]
DVD Normale Valeur P
Échocardiographie 32 73
Anticoagulation 12 (38%) 30 (39%) 0,83
thérapeutique
Angioscan pulm 5 EPs/10
Mortalité 13 (41%) 8 (11%) 0,001
30
30
152020-06-18
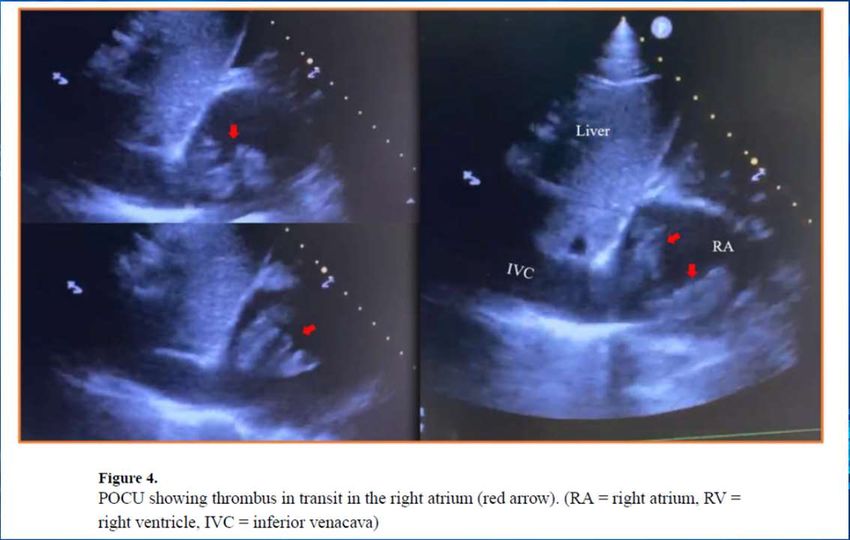
Cas rapporté [23]
▸ Pt 58 ans
▸ ATCD HTA, DLP, DM2, Tabagisme
▸ Arrive en ambulance,
▸ Syncope il y a 1 heure alors qu’il était au toilette précédé
d’étourdissement et de dyspnée
▸ Chirurgie à la hanche il y a 2 semaines et une douleur derrière le
genou gauche
31
31
BBD
S1
Q3T3
32
32
162020-06-18
33
33
34
34
172020-06-18
35
35
36
36
182020-06-18
37
37
38
38
192020-06-18
[2]
39
39
[22] 40
40
202020-06-18
Principes généraux pour le
choix de l’anticoagulation
▸ Vérifier d’abord les politiques de votre établissement
▸ Doit minimiser les visites du patient et du personnel
▹ HFPMs (ex enoxaparine 0,5 mg/kg) ou NACOs (attention
aux interactions Rx) ou HNF patients instables aux USI
▸ Le dosage doit bien couvrir les patients avec un IMC > 30
▸ Les doses de prévention intermédiaire ou thérapeutique
doivent être généralement réservées aux études cliniques
41
41
Patients hospitalisés avec CIVD
selon ACC [20]
▸ https://www.mdcalc.com/isth-criteria-disseminated-
intravascular-coagulation-dic
▸ Si aucun saignements évidents, prescrire la dose
d’anticoagulant prophylactique
▸ Si aucun saignement évident et le patient est sous
anticoagulation chronique, considérer réduire la dose
d’anticoagulant selon le risque thrombotique.
42
42
212020-06-18
CHEST Guidelines 2020 [29] (attention créatinine et plaquettes)
COVID-19 hospitalisé prévention TEV COVID-19 hospitalisé avec EP ou TPP prox
Étage USI Libération Étage USI Libération
Si pas de CIs: Si pas de CIs: Initial: HFPM (ou ((HFPM vs Si pas
(HFPM vs HFPM > HNF > HNF) fondaparinu d’intéraction Rx:
fondaparinux) > (fondaparinux Si pas d’intéraction x) > HNF) > NOACs sinon
HNF > NAOCs vs NOACs) Rx: apixaban ou thérapie Coumadin >
rivaroxaban orale HFPM
Seulement si Par la suite:
CIs Thpx Rx: dabigatran ou Minimum 3
Thpx edoxaban ou mois
mécanique coumadin
Dose Thpx > Dose Thpx > Dose Nil >Thpx
(Inter ou Thér) (Inter ou Thér)
Pas de
screening TPP
Pas antiplaquet Pas antiplaquet 43
43
Messages à retenir
▸ L’anticoagulation prophylactique doit être administrée à tous
les patients admis si pas de CIs
▸ Plus l’état du patient est sévère (ex USI), plus les D-dimers sont
élevés, plus la prévalence de la TEV est importante.
▸ L’investigation de la TEV repose d’abord sur les symptômes et
signes cliniques, et ce, même en présence d’anticoagulation
▸ Le POCUS peut contribuer à compenser l’accès difficile à
l’angio-scan pulmonaire et informer sur le pronostic
44
44
222020-06-18
Vous avez des questions ? Vous pouvez :
• Ouvrir la fenêtre de clavardage pour poser une question écrite
ou ;
• Utiliser la fenêtre « Q&A ».
SURVEILLEZ VOS COURRIELS :
Vous en recevrez un pour évaluer la visioconférence.
45
Références
[1] Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of
adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet.
2020;395(10229):1054-62.
[2] Yin S, Huang M, Li D, Tang N. Difference of coagulation features between severe pneumonia
induced by SARS-CoV2 and non-SARS-CoV2. J Thromb Thrombolysis. 2020.
[3] Wichmann, D., et al., Autopsy Findings and Venous Thromboembolism in Patients With
COVID-19: A Prospective Cohort Study. Ann Intern Med, 2020.
[3.1] Edler C, Schroder AS, Aepfelbacher M, Fitzek A, Heinemann A, Heinrich F, et al. Dying with
SARS-CoV-2 infection-an autopsy study of the first consecutive 80 cases in Hamburg, Germany. Int J
Legal Med. 2020.
[3.2] Fox SE, Akmatbekov A, Harbert JL, Li G, Quincy Brown J, Vander Heide RS. Pulmonary and
cardiac pathology in African American patients with COVID-19: an autopsy series from New Orleans.
Lancet Respir Med. 2020.
[4] Dolhnikoff M, Duarte-Neto AN, de Almeida Monteiro RA, Ferraz da Silva LF, Pierre de
Oliveira E, Nascimento Saldiva PH, et al. Pathological evidence of pulmonary thrombotic phenomena
in severe COVID-19. J Thromb Haemost. 2020.
46
46
232020-06-18
Références
[5] Helms J, Tacquard C, Severac F, Leonard-Lorant I, Ohana M, Delabranche X, et al. High
risk of thrombosis in patients with severe SARS-CoV-2 infection: a multicenter prospective cohort
study. Intensive Care Med. 2020.
[6] Leonard-Lorant I, Delabranche X, Severac F, Helms J, Pauzet C, Collange O, et al. Acute
Pulmonary Embolism in COVID-19 Patients on CT Angiography and Relationship to D-Dimer Levels.
Radiology. 2020:201561.
[7] Poyiadi N, Cormier P, Patel PY, Hadied MO, Bhargava P, Khanna K, et al. Acute
Pulmonary Embolism and COVID-19. Radiology. 2020:201955.
[8] Klok FA, Kruip M, van der Meer NJM, Arbous MS, Gommers D, Kant KM, et al.
Confirmation of the high cumulative incidence of thrombotic complications in critically ill ICU
patients with COVID-19: An updated analysis. Thromb Res. 2020.
[25] Stoneham SM, Milne KM, Nuttal E, Frew GH, Sturrock BR, Sivaloganathan H, et al.
Thrombotic risk in COVID-19: a case series and case-control study. Clin Med (Lond). 2020.
[26] Beun R, Kusadasi N, Sikma M, Westerink J, Huisman A. Thromboembolic events and
apparent heparin resistance in patients infected with SARS-CoV-2. Int J Lab Hematol. 2020.
[27] Cui S, Chen S, Li X, Liu S, Wang F. Prevalence of venous thromboembolism in patients
with severe novel coronavirus pneumonia. J Thromb Haemost. 2020. 47
47
Références
[9] Middeldorp S, Coppens M, van Haaps TF, Foppen M, Vlaar AP, Muller MCA, et al.
Incidence of venous thromboembolism in hospitalized patients with COVID-19. J Thromb Haemost.
2020.
[10] Llitjos JF, Leclerc M, Chochois C, Monsallier JM, Ramakers M, Auvray M, et al. High
incidence of venous thromboembolic events in anticoagulated severe COVID-19 patients. J Thromb
Haemost. 2020.
[11] Lodigiani C, Iapichino G, Carenzo L, Cecconi M, Ferrazzi P, Sebastian T, et al. Venous and
arterial thromboembolic complications in COVID-19 patients admitted to an academic hospital in
Milan, Italy. Thromb Res. 2020;191:9-14.
[12] Ren B, Yan F, Deng Z, Zhang S, Xiao L, Wu M, et al. Extremely High Incidence of Lower
Extremity Deep Venous Thrombosis in 48 Patients with Severe COVID-19 in Wuhan. Circulation.
2020.
[13] Thomas W, Varley J, Johnston A, Symington E, Robinson M, Sheares K, et al. Thrombotic
complications of patients admitted to intensive care with COVID-19 at a teaching hospital in the
United Kingdom. Thromb Res. 2020;191:76-7.
[13,1] Langer F, Kluge S, Klamroth R, Oldenburg J. Coagulopathy in COVID-19 and Its Implication
48
for Safe and Efficacious Thromboprophylaxis. Hamostaseologie. 2020.
48
242020-06-18
Références
[14] Bargellini I, Cervelli R, Lunardi A, Scandiffio R, Daviddi F, Giorgi L, et al. Spontaneous
Bleedings in COVID-19 Patients: An Emerging Complication. Cardiovasc Intervent Radiol. 2020
[15] Conti CB, Henchi S, Coppeta GP, Testa S, Grassia R. Bleeding in COVID-19 severe
pneumonia: The other side of abnormal coagulation pattern? Eur J Intern Med. 2020.
[28] Al-Samkari H, Karp Leaf RS, Dzik WH, Carlson JC, Fogerty AE, Waheed A, et al. COVID
and Coagulation: Bleeding and Thrombotic Manifestations of SARS-CoV2 Infection. Blood. 2020.
[16] Heman-Ackah SM, Su YS, Spadola M, Petrov D, Chen HI, Schuster J, et al. Neurologically
Devastating Intraparenchymal Hemorrhage in COVID-19 Patients on Extracorporeal Membrane
Oxygenation: A Case Series. Neurosurgery. 2020.
[17] Joob B, Wiwanitkit V. Hemorrhagic Problem Among the Patients With COVID-19: 49
Clinical Summary of 41 Thai Infected Patients. Clin Appl Thromb Hemost. 2020;26:
49
Références
[24] White D, MacDonald S, Bull T, Hayman M, de Monteverde-Robb R, Sapsford D, et al.
Heparin resistance in COVID-19 patients in the intensive care unit. J Thromb Thrombolysis. 2020.
[18] Agnes Lee Md, Menaka Pai, Menno Huisman, Stephan Moll, and Walter Ageno. COVID-19
and Pulmonary Embolism: Frequently Asked Questions. 2020.
[19] Thachil J, Tang N, Gando S, Falanga A, Cattaneo M, Levi M, et al. ISTH interim guidance on
recognition and management of coagulopathy in COVID-19. J Thromb Haemost. 2020;18(5):1023-6.
[20] Bikdeli B, Madhavan MV, Jimenez D, Chuich T, Dreyfus I, Driggin E, et al. COVID-19 and
Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and
Follow-up. J Am Coll Cardiol. 2020.
[21] Argulian E, Sud K, Vogel B, Bohra C, Garg VP, Talebi S, et al. Right Ventricular Dilation in
Hospitalized Patients with COVID-19 Infection. JACC Cardiovasc Imaging. 2020. 50
50
252020-06-18
Références
[22] Tang N, Bai H, Chen X, Gong J, Li D, Sun Z. Anticoagulant treatment is associated with
decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J Thromb
Haemost. 2020;18(5):1094-9.
[23] Au A, Hsu P, McClure M, Cabrera G, Kalivoda EJ. Serial Point-of-care Echocardiography
Performed by an Emergency Physician to Guide Thrombolytic Management of Massive Pulmonary
Embolism. Cureus. 2020;12(4):e7771.
[29] Moores LK, Tritschler T, Brosnahan S, Carrier M, Collen JF, Doerschug K, et al. Prevention,
diagnosis and treatment of venous thromboembolism in patients with COVID-19: CHEST Guideline
and Expert Panel Report. Chest. 2020.
[30] Spyropoulos AC, Levy JH, Ageno W, Connors JM, Hunt BJ, Iba T, et al. Scientific and
Standardization Committee Communication: Clinical Guidance on the Diagnosis, Prevention and
Treatment of Venous Thromboembolism in Hospitalized Patients with COVID-19. J Thromb
Haemost. 2020.
[31] Patel P, Sengupta N. PPIs and Beyond: A Framework for Managing Anticoagulation-
51
Related Gastrointestinal Bleeding in the Era of COVID-19. Dig Dis Sci. 2020.
51
Scientific and Standardization Committee Communication: Clinical Guidance
on the Diagnosis, Prevention and Treatment of Venous Thromboembolism in
Hospitalized Patients with COVID-19 [30]
▸ Guidance Statement 1: Diagnosis of VTE in hospitalized COVID-19 patients:
▹ a. Practitioners should use standard-of-care objective testing (i.e., CTPA, V/Q
scan, MRI venography, Doppler ultrasonography) to diagnose VTE based on
clinical index of suspicion. A pragmatic approach (i.e., point-of-care bedside
ultrasonography or echocardiography) can also be combined with standard-of-
care objective testing (50% of respondents).
▹ b. Routine screening for VTE using bedside Doppler ultrasonography of the
lower extremities or based on elevated D-dimer levels is not recommended
52
52
262020-06-18
Scientific and Standardization Committee Communication: Clinical Guidance
on the Diagnosis, Prevention and Treatment of Venous Thromboembolism in
Hospitalized Patients with COVID-19 [30]
▸ Guidance Statement 2: VTE prophylaxis in non-ICU hospitalized COVID-19
patients:
▹ a) A universal strategy of routine thromboprophylaxis with standard-dose
UFH or LMWH should be used after careful assessment of bleed risk, with
LMWH as the preferred agent. Intermediate-dose LMWH may also be
considered (30% of respondents).
▹ b) VTE prophylaxis recommendations should be modified based on extremes
of body weight, severe thrombocytopenia (i.e. platelet counts of 50,000 x
109 per liter or 25,000 x 109 per liter) or deteriorating renal function.
53
53
Scientific and Standardization Committee Communication: Clinical Guidance
on the Diagnosis, Prevention and Treatment of Venous Thromboembolism in
Hospitalized Patients with COVID-19 [30]
▸ Guidance Statement 3: VTE prophylaxis in sick ICU Hospitalized COVID-19 patients:
▹ a) Routine thromboprophylaxis with prophylactic-dose UFH or LMWH should
be used after careful assessment of bleed risk. Intermediate-dose LMWH (50%
of respondents) can also be considered in high risk patients. Patients with
obesity as defined by actual body weight or BMI should be considered for a
50% increase in the dose of thromboprophylaxis. Treatment-dose heparin
should not be considered for primary prevention until the results of
randomized controlled trials are available.
▹ b) Multi-modal thromboprophylaxis with mechanical methods (i.e.,
intermittent pneumonic compression devices) should be considered (60% of54
54 respondents)
272020-06-18
Scientific and Standardization Committee Communication: Clinical Guidance
on the Diagnosis, Prevention and Treatment of Venous Thromboembolism in
Hospitalized Patients with COVID-19 [30]
▸ Guidance Statement 4: Duration of VTE prophylaxis for hospitalized COVID-19
patients:
▹ a) Either LMWH (30%) or a DOAC (i.e., rivaroxaban or betrixaban 30% of
respondents) can be used for extended-duration thromboprophylaxis.
▹ b) Extended post-discharge thromboprophylaxis should be considered for
all hospitalized patients with COVID-19 that meet high VTE risk criteria.
The duration of post-discharge thromboprophylaxis can be approximately
14 days at least (50% of respondents), and up to 30 days (20% of
respondents).
55
55
Scientific and Standardization Committee Communication: Clinical Guidance
on the Diagnosis, Prevention and Treatment of Venous Thromboembolism in
Hospitalized Patients with COVID-19 [30]
▸ Guidance Statement 5: VTE treatment in hospitalized COVID-19 patients:
▹ a) Established guidelines should be used to treat patients with confirmed
VTE, with advantages of LMWH in the inpatient setting and DOACs in the
post-hospital discharge setting. A change from treatment-dose DOAC or
VKA to in-hospital LMWH should be considered especially for patients in
critical care settings or with relevant concomitant medications, and
dependent on renal function and platelet counts. Anticoagulant regimens
should not change based solely on D-dimer levels.
56
56
282020-06-18
Scientific and Standardization Committee Communication: Clinical Guidance
on the Diagnosis, Prevention and Treatment of Venous Thromboembolism in
Hospitalized Patients with COVID-19 [30]
▸ Guidance Statement 5: VTE treatment in hospitalized COVID-19 patients:
▹ b) A change of anticoagulant regimen (i.e.,from prophylactic or
intermediate-dose to treatment-dose regimen) can be considered in
patients without established VTE but deteriorating pulmonary status or
ARDS (50% of respondents).
▹ c) The duration of treatment should be at least 3 months (50% of
respondents).
57
57
ASH COVID-19 and Pulmonary Embolism: Frequently Asked
Questions (Version 2.0; last updated May 18, 2020
▸ In cases where there are no contraindications for therapeutic anticoagulation
and there is no possibility of performing imaging studies to diagnose PE or DVT,
empiric anticoagulation has been proposed in the following scenarios:
▹ 1. Intubated patients who develop sudden clinical and laboratory findings
highly consistent with PE, such as desaturation, tachycardia, increased CVP or
PA wedge pressure, or evidence of right heart strain on echocardiogram,
especially when CXR and/or markers of inflammation are stable or improving.
▹ 2. Patients with physical findings consistent with thrombosis, such as
superficial thrombophlebitis, peripheral ischemia or cyanosis, thrombosis of
dialysis filters, tubing or catheters, or retiform purpura (branching lesions
caused by thrombosis in the dermal and subcutaneous vasculature).
58
58
292020-06-18
ASH COVID-19 and Pulmonary Embolism: Frequently Asked
Questions (Version 2.0; last updated May 18, 2020
▸ In cases where there are no contraindications for therapeutic
anticoagulation and there is no possibility of performing imaging
studies to diagnose PE or DVT, empiric anticoagulation has been
proposed in the following scenarios:
▹ 3. Patients with respiratory failure, particularly when D-dimer
and/or fibrinogen levels are very high, in whom PE or
microvascular thrombosis is highly suspected and other causes
are not identified (e.g., ARDS, fluid overload).
59
59
CHEST Guidelines 2020 [29]
▸ 1. In the absence of contraindications, in acutely ill hospitalized patients
with COVID- 19, we suggest anticoagulant thromboprophylaxis over no
anticoagulant thromboprophylaxis.
▸ 2. In the absence of contraindications, in critically ill patients with
COVID-19, we recommend anticoagulant thromboprophylaxis over no
anticoagulant thromboprophylaxis
60
302020-06-18
CHEST Guidelines 2020 [29]
▸ 3. In acutely ill hospitalized patients with COVID-19, we suggest
anticoagulant thromboprophylaxis with LMWH or fondaparinux over
anticoagulant thromboprophylaxis with UFH; and we recommend
anticoagulant thromboprophylaxis with LMWH, fondaparinux or UFH
over anticoagulant thromboprophylaxis with a DOAC.
61
CHEST Guidelines 2020 [29]
▸ 4. In critically ill patients with COVID-19, we suggest anticoagulant
thromboprophylaxiswith LMWH over anticoagulant
thromboprophylaxis with UFH; and we recommend anticoagulant
thromboprophylaxis with LMWH or UFH over anticoagulant
thromboprophylaxis with fondaparinux or a DOAC.
▸ 5. In critically ill or acutely ill hospitalized patients with COVID-19, we
recommend against the use of antiplatelet agents for VTE prevention.
62
312020-06-18
CHEST Guidelines 2020 [29]
▸ 6. In acutely ill hospitalized patients with COVID-19, we recommend
current standard dose anticoagulant thromboprophylaxis over
intermediate (LMWH BID or increased weight-based dosing) or full
treatment dosing, per existing guidelines
63
CHEST Guidelines 2020 [29]
▸ 7. In critically ill patients with COVID-19, we suggest current standard
dose anticoagulant thromboprophylaxis over intermediate (LMWH BID
or increased weight-based dosing) or full treatment dosing, per existing
guidelines
▸ 8. In patients with COVID-19, we recommend inpatient
thromboprophylaxis only over inpatient plus extended
thromboprophylaxis after hospital discharge.
64
322020-06-18
CHEST Guidelines 2020 [29]
▸ 9. In critically ill patients with COVID-19, we suggest against the
addition of mechanical thromboprophylaxis to pharmacological
thromboprophylaxis.
▸ 10. In critically ill patients with COVID-19 who have a contraindication
to pharmacological thromboprophylaxis, we suggest the use of
mechanical thromboprophylaxis
▸ 11. In critically ill COVID-19 patients, we suggest against routine
ultrasound screening for the detection of asymptomatic DVT.
65
CHEST Guidelines 2020 [29]
▸ 12. For acutely ill hospitalized COVID-19 patients with proximal DVT or
PE, we suggest initial parenteral anticoagulation with therapeutic
weight adjusted LMWH or intravenous UFH. The use of LWMH will limit
staff exposure and avoid the potential for heparin pseudo-resistance. In
patients without any drug-to-drug interactions, we suggest initial oral
anticoagulation with apixaban or rivaroxaban. Dabigatran and
edoxaban can be used after initial parenteral anticoagulation. Vitamin K
antagonist therapy can be used after overlap with initial parenteral
anticoagulation.
66
332020-06-18
CHEST Guidelines 2020 [29]
▸ 14. In critically ill COVID-19 patients with proximal DVT or PE, we suggest
parenteral over oral anticoagulant therapy. In critically ill COVID-19
patients with proximal DVT or PE who are treated with parenteral
anticoagulation, we suggest LMWH or fondaparinux over UFH.
▸ 15. For COVID 19 patients with proximal DVT or PE, we recommend
anticoagulation therapy for a minimum duration of three months
67
CHEST Guidelines 2020 [29]
▸ 16. In most patients with COVID-19 and acute, objectively confirmed PE
not associated with hypotension (systolic blood pressure < 90 mm Hg or
blood pressure drop of >=40 mm Hg lasting longer than 15 minutes), we
recommend against systemic thrombolytic therapy.
68
342020-06-18
CHEST Guidelines 2020 [29]
▸ 17. In patients with COVID-19 and both acute, objectively confirmed PE
and hypotension (systolic blood pressure < 90 mm Hg) or signs of
obstructive shock due to PE, and who are not at high risk of bleeding,
we suggest systemically administered thrombolytics over no such
therapy.
69
CHEST Guidelines 2020 [29]
▸ 18. In patients with COVID-19 and acute PE with cardiopulmonary
deterioration due to PE (progressive increase in heart rate, a decrease
in systolic BP which remains >90 mm Hg, an increase in jugular venous
pressure, worsening gas exchange, signs of shock (eg, cold sweaty skin,
reduced urine output, confusion), progressive right heart dysfunction
on echocardiography, or an increase in cardiac biomarkers) after
initiation of anticoagulant therapy who have not yet developed
hypotension and who have a low risk of bleeding, we suggest systemic
thrombolytic therapy over no such therapy.
70
352020-06-18
CHEST Guidelines 2020 [29]
▸ 19. We recommend against the use of any advanced therapies (systemic
thrombolysis, catheter-directed thrombolysis or thrombectomy) for
most patients without objectively confirmed VTE.
▸ 20. In those patients with COVID-19 receiving thrombolytic therapy, we
suggest systemict hrombolysis using a peripheral vein over catheter
directed thrombolysis
71
CHEST Guidelines 2020 [29]
▸ 21. In patients with COVID-19 and recurrent VTE despite
anticoagulation with therapeutic weight adjusted LMWH (and
documented compliance), we suggest increasing the dose of LMWH by
25 to 30%.
▸ 22. In patients with COVID-19 and recurrent VTE despite
anticoagulation with apixaban, dabigatran, rivaroxaban or edoxaban
(and documented compliance), or vitamin K antagonist therapy (in the
therapeutic range) we suggest switching treatment to therapeutic
weight-adjusted LMWH.
72
36Vous pouvez aussi lire

















































