Jongler avec le poids et les antirétroviraux - Rachel Therrien Pharmacienne Clinique des maladies virales chroniques CIVC - CHUM - PNMVH
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous
Jongler avec le poids
et les antirétroviraux
Rachel Therrien Pharmacienne
Clinique des maladies virales
chroniques CIVC - CHUM
SYMPOSIUM QUÉBEC PNMV, 28 MAI 2020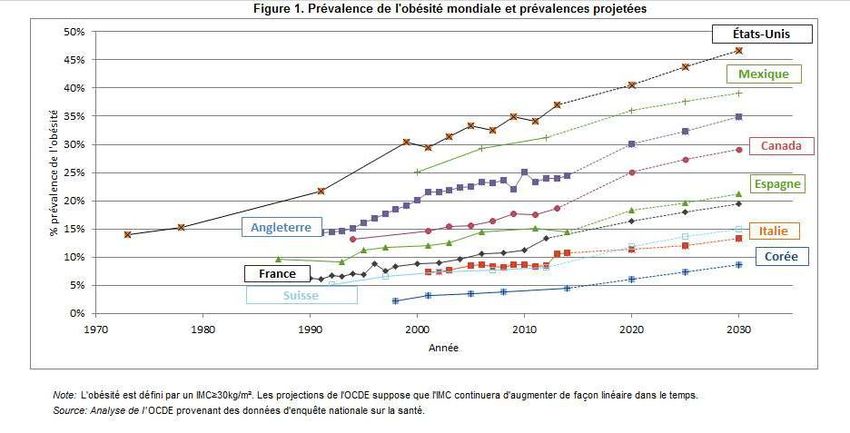
Conflits potentiels Conférencière-consultante Subventions • Gilead • Merck • ViiVHealthcare
Objectifs
• Connaître les principales données reliées à la prise de poids avec les
antirétroviraux
• Tenter de répondre aux questions
Quels antirétroviraux ?
Facteurs de risques ?
Mécanisme ?
Risques ?
On dit quoi ?
On fait quoi ?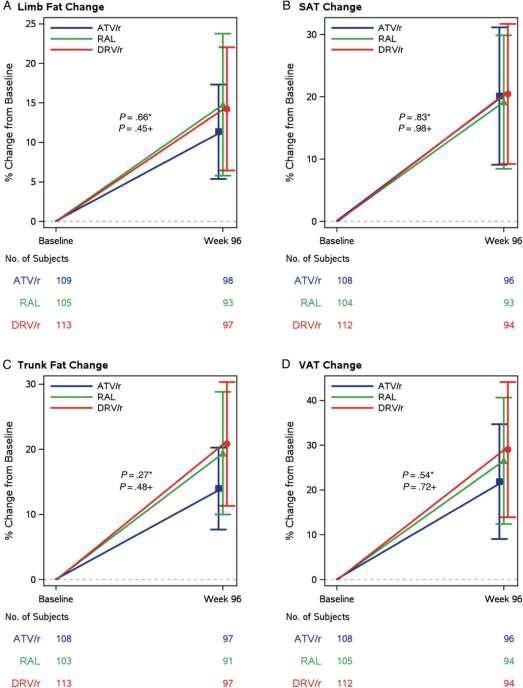
Introduction Among individuals on
suppressive ART, wasting
has become less common
and recent studies from both
upper- and lower-income
countries report weight gain
irrespective of ART type.
Recent studies have shown that (INSTI)-based regimens have recently been
initiating ARV therapy leads to associated with greater weight gain compared
weight gain, from a few with protease inhibitor (PI)-based1or non-
kilograms to >20% of original nucleoside reverse transcriptase inhibitor
bodyweight,especially within the (NNRTI)-based regimens
first year
Greater risk of weight gain in There have been reports of increased
females compared with males weight gain with TAF use in
antiretroviral therapy (ART)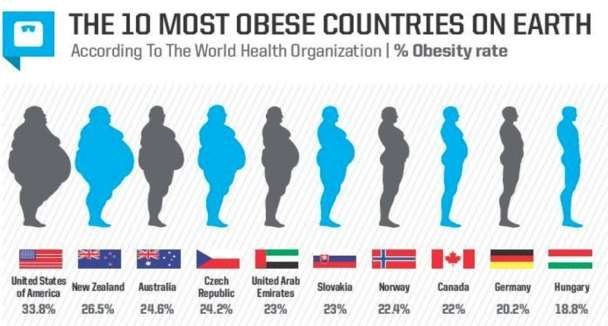
Intro : mesure du poids
Poids : Kg
IMC : poids et taille
< 18,5 ou > 25 augmente le risque de
développer des problèmes de santé
**L’IMC ne fait toutefois pas de distinction entre le gras
ou les muscles, ce qui peut influencer l’estimation du
risque chez certains adultes**
Tour de taille : > 94 cm chez l’homme et > 80
cm chez la femme
**Une augmentation du tour de taille même sans surplus
de poids augmente le risque de développer des
problèmes de santé**
**VAT vs SAT : *
Magnetic resonance imaging and computed
Lake JE, Moser C, Johnston L, Magyar C, Nelson SD,
tomography (CT) remain the gold standard for Erlandson KM et al. CT Fat Density Accurately Reflects
Histologic Fat Quality in Adults With HIV On and Off
quantifying SAT and VAT Antiretroviral Therapy. J Clin Endocrinol Metab.
2019;104(10):4857–64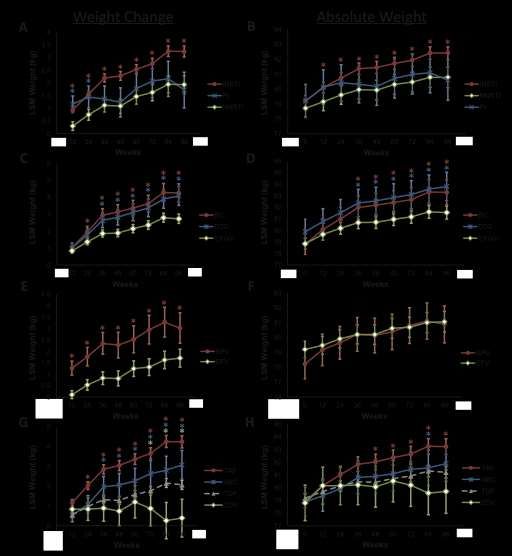
Intro : épidémie mondiale de l’obésité : ⇡ prévalence
Femme ➢ Homme dans certains pays
L’Organisation de coopération et de
développement économiques
(OCDE)
6
Obésité androïde Obésité gynoïde
Complications observées selon le type (abdomino-mésentérique- --------pomme) (fessio-crurale ------poire)
d’obésité Maladies cardio-vasculaires, coronaropathies Arthropathies
HTA, troubles du rythme gonarthrose
insuffisance cardiaque coxarthrose
accidents vasculaires cérébraux, (ischémiques et hémorragiques) dorsalgie
Complications respiratoires Veinopathies
insuffisance respiratoire varices, phlébite, thrombose
syndrome d’apnée du sommeil embolie (post-op.)
hypoventilation alvéolaire, HTAP 2 fois moins de complications
respiratoires
Complications métaboliques
4 fois moins de complications
insulino-résistance
métaboliques
baisse du cholestérol HDL
hypertriglycéridémie (VLDL)
diabète de type II
Complications cutanées : hypersudation, mycose, lymphœdème
Complications post-opératoires –
Pomme ou poire : discrimination;
Cancers : prostate, colon, œsophage, cardia
Cancers : sein, utérus
l’altération de l’image de soi et de la qualité
Atteintes hépato-digestives : stéatose, hépatite alcoolique, cirrhose,
Atteintes hépato-digestives : lithiase biliaire
de vie reflux gastro-œsophagien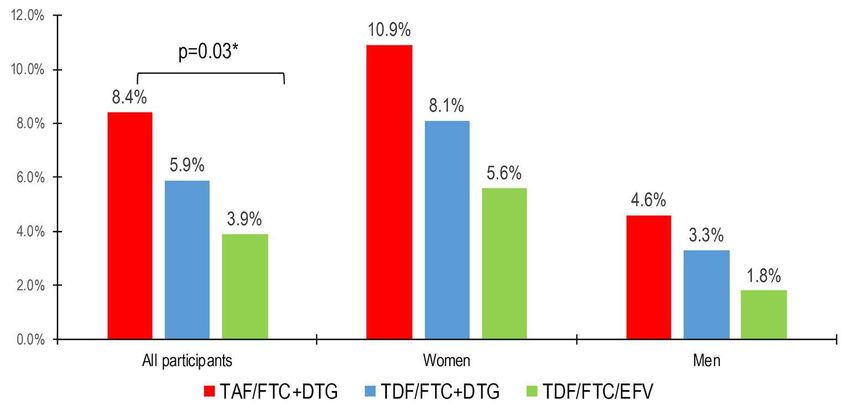
Jongler avec le poids D'où vient tout ce questionnement sur le poids ?
D'où vient tout ce questionnement du poids ?
ADVANCE : (Afrique du Sud)
Caractéristiques de bas
DTG + FTC/TAF DTG + FTC/TDF EFV/FTC/TDF
DTG + FTC/TAF n=351 n=351 n=351
Naïfs Age moyen 33 ± 8 32 ± 8 33 ± 7
VL ≥500 c/mL
DTG + FTC/TDF Femme 61% 59% 57%
(N=1,053)
Noir 99% 100% 100%
Poids moyen (kg)
EFV/FTC/TDF • Homme 67.9 67.1 67.3
• Femmme 68.8 69.5 70.2
IMC, mean (kg/m2)
48 weeks 96 weeks 192 weeks • Homme 21.7 21.6 21.8
• Femmme 25.6 26.1 26.1
BL CV ≥100,000 -
500,000 c/mL
19% 18% 21%
CD4+, cells/mm3 349 ± 225 323 ± 234 337 ± 222
1. Venter W, et al. IAS 2019. Mexico City, Mexico. Oral WEAB0405LB
2. Venter W, et al. N Engl J Med 2019; epub 24 July
3. Venter F, et al. AIDS 2020. Oral OAXLB0104 9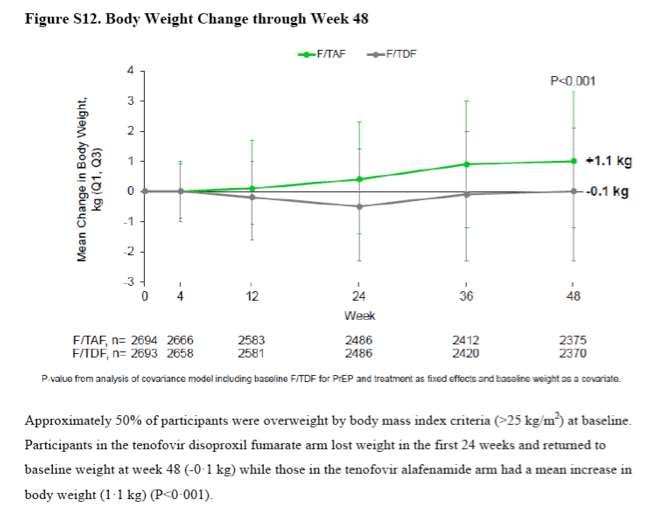
Jongler avec le poids AVANT ---------- ADVANCE ?-----------APRÈS Études randomisées/cohorte Patients naïfs /switch Patients VIH+/VIH-
NA-ACCORD
Avant ADVANCE N: 14,000 USA + CANADA (1998-2010)
Patient obèse : 9% à 18%
En 3 ans (IMC)
22% Normal à overweight
18% Overweight à obèse
A greater weight gain was also associated with a
lower pretreatment CD4 + T cell count and higher
viral load ( p < 0.001 for both),
Conclusion : Weight remains desirable, though this
view needs to be balanced against the potential
health risks of excess adiposity. While further research
is needed to understand the metabolic and
cardiovascular consequences of comorbid HIV and
Koethe JR et al. Rising Obesity Prevalence and Weight obesity, the management of weight-related health
Gain Among Adults Starting Antiretroviral Therapy in
conditions will be a priority and challenge for the care of
the United States and Canada. AIDS Res Hum
Retroviruses. 2016;32(1):50–8.
contemporary HIV-infected individualsACTG 5260s (RAL vs IP/r)
sous étude 5257
Hommes
Le reste semblable
ADVANCETruvada + DRV/r ou ATZ/r vs RAL Our study showed an overall increase in BMI after 96 weeks of ART in a mildly overweight population. The increase in BMI after ART was perceived as a favorable consequence of virological control, or “return-to-health,”However, in the current era of universal ART for HIV infection, it is likely that this increase in BMI surpasses what is expected from return-to-health and may have unfavorable consequences on health. For the first time in a large randomized ART-initiation trial, we showed that central and peripheral fat changes were not different after 96 weeks of treatment with 2 boosted PIs or with the integrase inhibitor RAL.
ACTG 5257 : 96 SEM
Tour de taille moyen : 90,6 cm
↑ moyenne à 96 semaines de 3,4 cm
RAL > DRV /r (P = .0130)
RAL > ATV /r femmes vs hommes (P = .0065)
RAL > DRV/r noirs vs non noirs (P = .0043)
CV initiale plus élevée et faible CD4
étaient associés au tour de taille plus élevé
Référence santé canada
Tour de taille : > 94 cm chez l’homme et > 80 cm femmeÉtudes pts naïfs
randomisées/cohorte
Gilead 1489-90 (BIC VS DLG +ABC/3TC ou TDF/TAF)
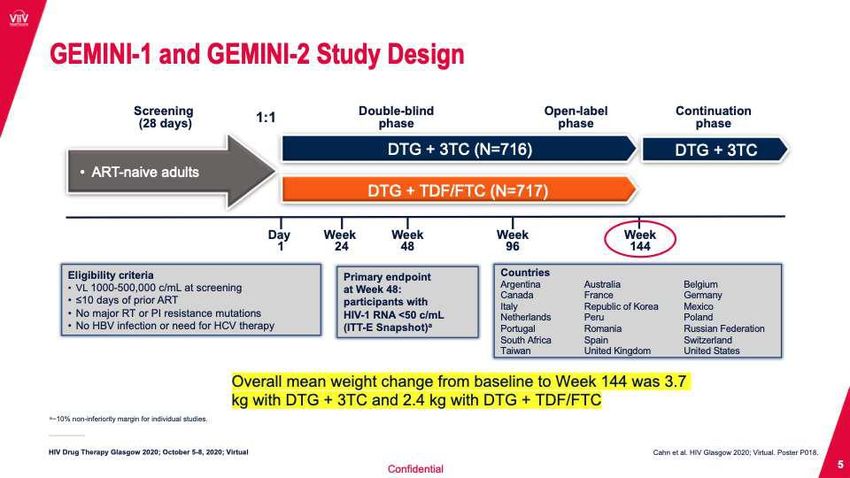
GEMINI 1-2 (DLG+3TC) vs (DLG+TDF/FTC)
NA-ACCORD (Canada et USA - 17 sites)
Études poolées (8 études)
Étude avec doravirinePooled 1489 & 1490: B/F/TAF in ART-Naïve Adults Orkin C, et al. EACS 2019. Basel, Switzerland. PE3/14
Changement de poids à 144 sem
Study 1489 Study 1490
Median Weight Change,
kg (Q1, Q3)
+5.0 kg
+4.1 kg +4.4 kg
+3.5 kg
Week Week
Study 1489 Study 1490
B/F/TAF DTG/ABC/3TC B/F/TAF DTG + F/TAF
Participants, % n=314 n=315 n=320 n=325
≥5% weight gain 52 48 53 55
≥10% weight gain 29 25 30 32
Weight loss or no change from baseline 24 26 21 22
Conclusion : changement de poids similaire BIC = DLG
⅓ augmentation de plus de 10% poids
Perdre 10% de son poids ( si surpoids non désiré) = une bonne année d’effort 17Ténofovir DF : empêche prise de poids ?
NA-ACCORD (Canada -USA)
N : 22 972 (janvier 2007- dec 2016)
Analyse multivariée linéaire mixte Atripla
87% hommes, 41% blanc
IMC : 25kg/m2
ARV départ (49% INNTI, 31% IP et 20% INsTI)
TDF : presque à 100%
CD4 : 308 cell/mm3
*Ajusté : âge, race, site, année acquisition VIH,année début ARV, poids départ, CV et CD4
Résultat gain pondéral sur 5 ans
INSTI 5.9 kg (4.9, 2 ans) Résultat gain pondéral sur 2 ans
IP : 5.5 kg (4.9, 2 ans) DLG : 7.2 kg
INNTI : 3.7 kg (3.1, 2 ans) RAL : 5.8 kg
EVG : 4.1 kg
DLG>RAL>EVG
INSTI>IP>INNTI
Résultat à 2 ans : femmes, patients avec CD4 bas et sur
INsTI ont plus de chance d’avoir une augmentation de
plus de 10% de leur poids.
Adjusted odds ratio = 1.37, 95% confidence interval: 1.20 to 1.56N : 1152 Patients Naïfs ARV
Suivi : janvier 2007-janvier 2016
Vanderbilt Comprehensive Care Clinic (Nashville)
Analyse multivariée linéaire mixte
86% Hommes
49% Blanc
IMC : 25.1kg/m2
Âge : 35 ans
INSTI : 30.5%, IP : 39.4% et INNTI : 30.1%
TDF : presque à 100%
(p〈 .05)
CD4 : 318 cell/mm3
Résultat gain pondéral sur 18 mois :
DLG : 6 kg vs INNTI : 2.6 kg (p〈 .05)
et EVG : 0.5 kg (p〈 .05)
VS IP : 4.1 kg, vs RTG : 3.4 kg
Bourgi K et al.Greater Weight Gain in Treatment-naive Persons Starting
Dolutegravir-based Antiretroviral Therapy.
Clinical Infectious Diseases, 2020;70(7) : 1267–1274.Mean Weight Change at Week 48
2003 à 2019
Analyse poolée de 8 études
randomisées
>5000 participants
et 10 000 personne suivi-année
Suivi : 96-144 sem (résultat à
48 sem)FEMME > HOMME
NOIRE > BLANC
Femmes noires > femmes
blanches
DTG-BIC>EGV Hommes noires > hommes blancs
INSTI>IP>INNTI
Participants taking INSTIs experienced the TAF>TDF et ABC
most weight gain (mean: 3.24 kg) Mean weight gain: TAF = 4.25
kg; ABC = 3.08 kg DF= 2.07kg
Prise>10% plus avec TAFVariable OR (95% CI) P Value
CD4 count (Changes in weight and BMI with first-line doravirine based therapy
Jongler avec le poids Qu’est ce qui explique tout cela ? Retour à la santé ?
Modification du poids : historique
Historique Arrivée des traitements pour le VIH Arrivée des combinaisons ARV Étude ADVANCE
hautement efficaces
Patients avec faible CD4, CV élevée et INTI + IP
faible IMC
Prise de poids (type) Modification du poids suite au contrôle de Modification des graisses suite à Modification du poids suite à la
la maladie et retour de la santé. la prise des antirétroviraux : prise d’antirétroviraux :
lipodystrophie : redistribution des Gain masse grasse > maigre
graisses
Quels agents Toute combinaison d’antirétroviraux Lipoatrophie : INTI Associée récemment aux
Lipoaccumulation : IP (?) inhibiteurs de l’intégrase (INSTI)
et ténofovir AF
femmes, noires
Mécanisme Retour à la santé INTI : toxicité mitochondriale ? Retour santé ?
Contrôle inflammation et hypercatabolisme IP : rôle et mécanisme
Leptine
Contrôle IO et atteintes intestinales marqueurs inflammatoire-leptine-
melanocortin
adiponectine ?
Risque sur la santé Vu comme positif Associé risque de maladies Risque cardiovasculaire et
cardiovasculaires métabolique ?
Diminution estime de soi (image) Estime de soi ?MÉCANISME ? Obesity Reviews. 2021;22(S2):e13189.
Kaiser Permanente (US)
‡
BMI Change Over time Between PLWH and HIV-
Negative Individuals
Retrospective matched cohort study of 8,256 PLWH initiating ART and 129,966 HIV-negative individuals (2006-2016)
PLWH HIV-Neg Change in BMI by HIV Status
Baseline Characteristics
(n=8,256) (n=129,966)
▪ PLWH had lower BMI at the
Mean age, years 41 42
Uninfected (N=129,966)
start and increased at 3-
Male, % 88 87 times the rate of HIV-
PWH (N=8,256)
negative individuals
0.06 kg/m2 per year (reference) 29.4
Ethnicity/Race, %
White 36 40 28.7 ▪ By 12 years, PLWH and
Black 26 26 HIV-negative individuals had
Alcohol use disorder, % 11 7
similar BMIs
Substance use disorder, % 16 6
28.4 ▪ Limitations: some patient
characteristics may change
Smoking, ever 47 37 after baseline (e.g. smoking
Baseline BMI (Kg/m²), %
0.22 kg/m2 per year (PJongler avec le poids Qu’est ce qui explique tout cela ? Antirétroviraux ? Études avec patients naïfs 1. INsTI +/- Taf : accélèrent prise de poids par un mécanisme inconnu? 2. Toxicité Ténofovir DF et éfavirenz qui empêchent la reprise de poids ?
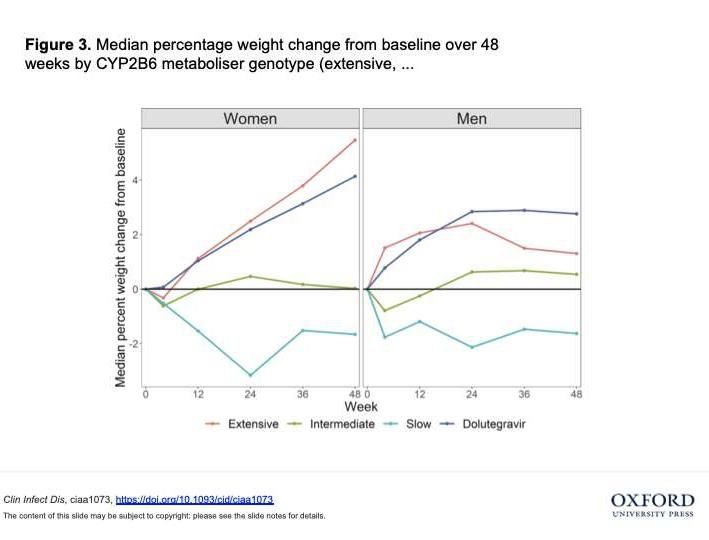
Sous analyse de l’étude ADVANCE.
N : 324 DLG 168 EFV
We found that CYP2B6 metaboliser genotype was strongly associated with weight
gain over 48 weeks in the efavirenz arm: extensive metabolizers gained the most
weight, whereas slow metabolizers lost weight.
CYP2B6 extensive metabolizers in the efavirenz arm had similar weight gain to
participants in the dolutegravir arm.
Conclusions. CYP2B6 metaboliser genotype was associated with
weight gain in PLWH starting efavirenz-based ART.
Weight gain was similar between CYP2B6 extensive metabolizers
in the efavirenz arm and in the dolutegravir arm, suggesting that
impaired weight gain among CYP2B6 slow or intermediate
metabolizers could explain the increased weight gain on
dolutegravir compared with efavirenz observed in ADVANCE and
other studies.Ténofovir TAF vs Ténofovir DF (utilisation en prévention PrEP- VIH-) Mayer et al. Lancet 2020
Weight gain before and after switch from TDF to TAF in a U.S. cohort
study
OPERA
n: 107,308
84 cliniques USA
2010-2019
Poids : 60 mois
avant switch et
12 mois après
Mallon PWG et al. Journal of the
International AIDS Society 2021,
24:e25702Poids (Kg) : avant , 0-9 mois et plus 9 mois
An early and pronounced weight gain was observed shortly after a switch
from TDF to TAF, both in PLWH who maintained all other ARVs and in
those who also switched to an InSTI-based regimen, followed by a
flattening of the curve after nine months of TAF use. Such patterns of
weight gain were observed regardless of the specific InSTI agent used.
These results, suggesting an independent effect of TAF on weight, are of
clinical importance as increases in weight can impact long-term clinical
outcomes such as cardiovascular diseases, diabetes, fatty liver or other
disorders. The potential long-term clinical impact of the early, rapid, but
transient increase in weight observed with TAF remains to be explored.Jongler avec le poids Quels sont les risques ?
Risques ?
Obesity itself is a pro-inflammatory Mauvais contrôle du VIH est aussi associé à
condition, and is associated with processus inflammatoire
increased circulating inflammatory
markers in both PWH and HIV-negative
Herrin M, et al. Weight Gain and Incident Diabetes
Among HIV-Infected Veterans Initiating Antiretroviral
Excess adiposity weight gain in PWH Therapy Compared With Uninfected Individuals. J Acquir
confers greater risk of metabolic Immune Defic Syndr. 2016;73(2):228–36
disease compared with HIV-negative Achhra AC, Sabin C, Ryom L, Hatleberg C, Antonella
individuals d’Aminio M, de Wit S et al. Body Mass Index and the
Risk of Serious Non-AIDS Events and All-Cause
Mortality in Treated HIV-Positive Individuals: D: A: D
Cohort Analysis. J Acquir Immune Defic Syndr.
Metabolic diseases including : 2018;78(5):579–88.
diabetes mellitus, neurocognitive
McCutchan J et al. Role of obesity, metabolic variables, and diabetes
impairment, liver disease, and in HIV-associated neurocognitive disorder. Neurology.
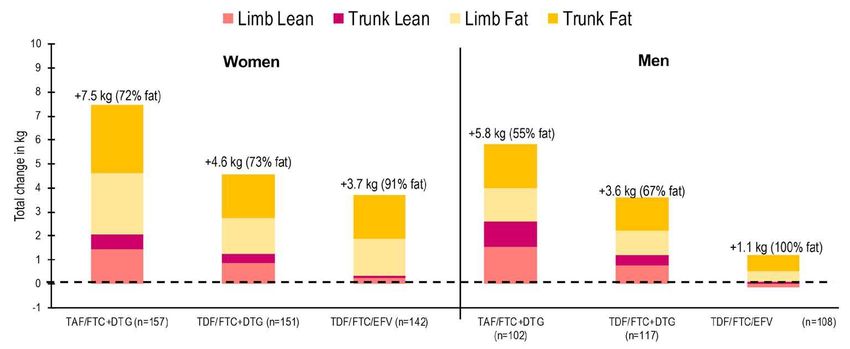
cardiovascular disease 2012;78(7):485–92.Changement de la composition corporelle à 96 semaines
• Prise de poids était principalement en masse adipeuse et était répartie au n/v tronculaire
et au n/v des membres.
• Gain en gras était plus significatif chez les femmes vs homms (pSyndrome métabolique: Advance semaine 96
• *Statistiquement significatif
• Venter et al. AIDS 2020; Virtual. Slides OAXLB0104.
For Reactive Use OnlyAll 3 PWH had modestly elevated HbA1c values at baseline; however, they had rapid development of severe hyperglycemia and ketoacidosis, suggesting that INSTI use may be associated with rapid acceleration of dysglycemia and that these agents may contribute to beta-cell dysfunction and/or insulin resistance independent of weight gain. The presence of ketoacidosis supports the possibility of impaired beta-cell function in addition to increased insulin resistance. Although insulin requirements declined after a switch in ART, this can be seen after resolution of glucose toxicity and does not demonstrate that INSTIs directly impair beta-cell function. It is also not clear whether impaired glycemic control completely resolves with discontinuation of the offending INSTI.
UGANDA
16 (0·47%) / 3417 DLG
VS 1 (0·03%) / 3230 Groupe control
(p=0·0004, Fisher’s exact)
Correspondance : thelancet
Hyperglycémie a été sévère pour 15 des 16
patients
La majorité précédé par une perte de poids
Le temps moyen début symptômes : 4 mois (2·5–
4·5)
.
Findings were reported to the Uganda Ministry of Health, the
National Drug Authority in Uganda, and the manufacturer of
dolutegravir. We show an association between
hyperglycaemia and dolutegravir initiation and
describe a clinical phenotype at risk for severe hyperglycaemia.
If patients with a long history of ART are to be switched to a
dolutegravir-containing regimen, a monitoring plan for
hyperglycaemia should be part of the clinical care packageDiabète (Boston)
Étude de cohorte rétrospective 2007-2017 (Boston)
Début thérapie ARV ( depuis 18 mois et plus)
N : 123 InSTI
N :489 non-InSTI
Résultats :
Analyse multivariée
Ajustement années début Tx, ethnicité, INTI, âge, CD4, CV
↑ significative poids femmes après 24 mois
+10.62% femmes blanche et 11.02% femmes non blanches
3x plus de risque de diabète après 18 mois.
Déterminé par ICD codes (adjusted hazard ratio 3.29, P = 0.014).
Asundi A, Olson A, Jiang W, et al. Risk factors and metabolic implications of integrase
inhibitor associated weight gain. IDWeek 2020, October 22-25, 2020. Abstract 946.Incidence of diabetes in HIV-infected patients treated
Diabète : France with first-line integrase strand transfer inhibitors: a
French multicentre retrospective study
Objectives
To assess if an INSTI as a third agent is statistically associated with new-onset diabetes mellitus compared
with an NNRTI or a PI.
Patients and methods
Patients undergoing first-line combined ART (cART) without diabetes at baseline were retrospectively
Journal of Antimicrobial Chemotherapy,
Volume 75, Issue 11, November 2020, included from the Dat’AIDS French cohort study . Incident diabetes mellitus was defined as a notification of new
Pages 3344–3348 diabetes in the medical history, a glycated haemoglobin (HbA1c) level superior to 7.5% or the start of a diabetes
therapy following the initiation of ART.
Results
From 2009 to 2017, 19 462 patients were included, among which 265 cases of diabetes mellitus occurred.
Multivariate and survival analyses did not highlight an increase in new-onset diabetes in patients
Did not link body mass index
undergoing cART with an INSTI as a third agent compared with an NNRTI or a PI. BMI >30 kg/m2, age
above 30 kg/m2 (obesity) to
new-onset diabetes. >37 years old (in survival analysis), black race or Hispanic ethnicity, arterial hypertension and AIDS were
associated with a higher proportion of incident diabetes.
Conclusions
INSTIs were not statistically associated with new-onset diabetes. However, clinicians should remain aware
of this possible metabolic comorbidity, particularly in patients with a high BMI and older patients.Diabète : FDA Adverse Event Reporting System (FAERS) Analyzed FAERS data (2007-2019), using the Standardized MedDRA Query (SMQ) for hyperglycemia or new-onset diabetes mellitus (H/DM). They defined weight gain as increased weight or body mass index analyzed as a separate event. To explore associations between medications and these two grou ps of adverse events, the investigators calculated reporting odds ratios (ROR) and 95% confidence intervals (CI) for the entire integrase inhibitor class and for individual integrase inhibitors . The researchers adjusted the analysis for gender, age, type of reporter (for example, patient or provider), specific integrase inhibitor, and SMQ terminology for the adverse event of interest. Sorting through more than 10.1 million FAERS reports disclosed 732,591 cases of H/DM (7.2%) and 109,556 reports of weight gain (1.1%). Nearly half of these reports (49%) came from consumers, while physicians provided one quarter (23%). Patient age averaged 57 years (standard deviation 17), and 63% were women. Countries with the most reports were the United States, the United Kingdom, and Japan. The researchers counted 7840 reports for dolutegravir, 5551 for raltegravir, 4034 for elvitegravir, 1414 for bictegravir, and 18,400 for any integrase inhibitor. Statistical analysis independently linked each of these integrase inhibitors, and the entire class, to greater odds of weight gain: Greater odds of weight gain: -- Any integrase inhibitor: ROR 2.16, 95% CI 1.96 to 2.38 -- Bictegravir: ROR 6.82, 95% CI 5.50 to 8.41 -- Raltegravir: ROR 3.29, 95% CI 2.77 to 3.91 -- Dolutegravir: ROR 1.86, 95% CI 1.58 to 2.18 -- Elvitegravir: ROR 1.63, 95% CI 1.37 to 1.92 Integrase inhibitors as a class, bictegravir, and dolutegravir independently upped odds of metabolic events recorded as H/DM: Greater odds of metabolic adverse events: -- Any integrase inhibitor: ROR 1.20, 95% CI 1.15 to 1.27 -- Bictegravir: ROR 1.23, 95% CI 1.10 to 1.37 -- Dolutegravir: ROR 1.28, 95% CI 1.19 to 1.39 Avec les limites de cette analyse : ils concluent que tous les inhibiteurs de l’intégrase sont associés à un gain de poids. Dolutégravir et bictégravir sont associés avec un d’hyperglycémie et nouveau diagnostic de diabète. Ce risque potentiel d’effet métabolique doit être considéré en pratique lors de la prescription d’un inhibiteur de l’intégrase.
Jongler avec le poids Quels sont les solutions ? Modification de la thérapie ARV ? Étude Doravirine (DRIVE-SHIFT) Etude TANGO (DLG+ 3TC) ****Etude en cours avec Doravirine***
Jongler avec le poids Quels sont les solutions ? Médicaments pour la perte de poids ? Liraglutide (Saxenda)* Naltrexone/Bupropion (Contrave) Orlistat (Xenical)
Jongler avec le poids
Quels sont les solutions ?
● Reconnaître que la prise de poids avec
les ARV est possible.
Faire enseignement
Suivre plus étroitement surtout 1er année
Identifier hyperphagie
Conseils (alimentaires-exercices etc)
****10 kg, ou une perte de 10 % du poids, c’est souvent un an d’effort !****
Weight Loss Interventions Medical Weight Loss Interventions Behavioral interventions through caloric
restriction and physical exercise are effective in promoting weight loss in PWH, including adipose tissue loss in
subcutaneous and visceral compartmentsConclusion Tenter de répondre aux questions Quels antirétroviraux ? INsTI, TAF Facteurs de risques ? Femmes, noires, CD4 bas, CV élevée Mécanisme ? Fat overshoot (retour santé pas santé), toxicité TDF, EFV, TAF et INsTI (mécanisme) ?? Risques ? Hyperglycénie, diabète autres troubles métaboliques ? Estime de soi. On dit quoi ? La vérité. Ce que l’on connaît ad présent On fait quoi ? Suivi plus étroit (éviter rapidement prise de poids). Et attend la suite de l’histoire. La médication actuelle reste la meilleure qu’on a eu jusqu’à présent.
Vous pouvez aussi lire