AVANTAGE ENDO : L'ADOPTION DE LA CHIRURGIE ENDODONTIQUE - UN PILIER PRÉVISIBLE POUR VOTRE PRATIQUE DOCTEUR PETER TAWIL
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous

AVANTAGE ENDO :
L’ADOPTION DE LA CHIRURGIE
ENDODONTIQUE – UN PILIER PRÉVISIBLE POUR
VOTRE PRATIQUE
DOCTEUR PETER TAWIL
LE DIMANCHE 26 MAI 2019 DE 8 H 30 À 15 H 30
Salle 510A
AVIS DE NON-RESPONSABILITÉ ET DE NON-ENDOSSEMENT
Les JDIQ et l’ODQ consacrent tous les efforts possibles afin de vous présenter des
conférenciers de haut niveau dans chacun des domaines de la médecine dentaire. La
présentation de ces conférences ne signifie en aucun cas que les JDIQ ou l’ODQ
endossent les opinions, les produits, les techniques, les services ou le matériel
présentés dans le cadre de ces conférences ou ateliers et ils déclinent toute
responsabilité à cet égard.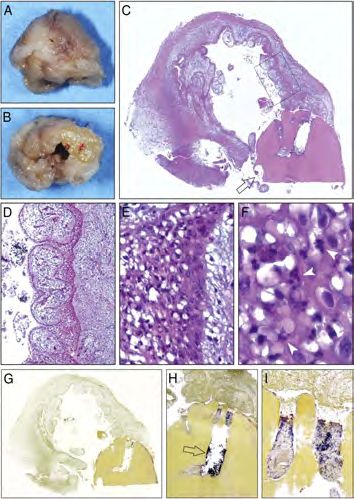
L’Adoption de la Chirurgie Endodontique
Un pilier prévisible pour votre pratique Interdiction:
• d’être debout dans les allées ou devant les portes.
• d'enregistrer la conférence (audio ou vidéo).
• de fumer ou de consommer nourriture ou breuvages.
N’oubliez pas:
• de faire scanner votre porte-nom pour vos unités de
formation continue.
• de mettre vos appareils en mode silencieux.
Peter Zahi Tawil DMD, MS, FRCD(C),
Diplomate, American Board of Endodontics • de remplir les formulaires d'évaluation.
Olmsted Family Distinguished Professor
Graduate Program Director - UNC Endodontics
1 2
AM Cours 8h30-10h30am
La Gestion des Complications Endodontiques
Guardez votre calme et continuez
AM Pratique 10h30-11h30am
Hands-On: Instrumentation CM
Pause Lunch 11h30am-12h30pm
PM Cours 12h30-2h30pm
L’Adoption de la Chirurgie Endodontique
Un pilier prévisible pour votre pratique
PM Pratique 2h30-3h30pm
Hands-On: Reparation de perforation et obturation rétro
3 4
L’Adoption de la Chirurgie Endodontique Embracing Endodontic Surgery
Etiologie, Diagnostic & Options de traitement Etiologie, Diagnostic & Options de traitement
Styles de lambeaux gingival Styles de lambeaux gingival
Accès osseux, curettage & biopsie Accès osseux, curettage & biopsie
Hémostase Hémostase
Gestion de l'extrémité radiculaire Gestion de l'extrémité radiculaire
Résection radiculaire Résection radiculaire
Préparation rétrograde Préparation rétrograde
Obturation rétrograde Obturation rétrograde
Régénération parodontale Régénération parodontale
Sutures Sutures
Soins Post-op Soins Post-op
5 6
Avantage Endo PM - May 15, 2019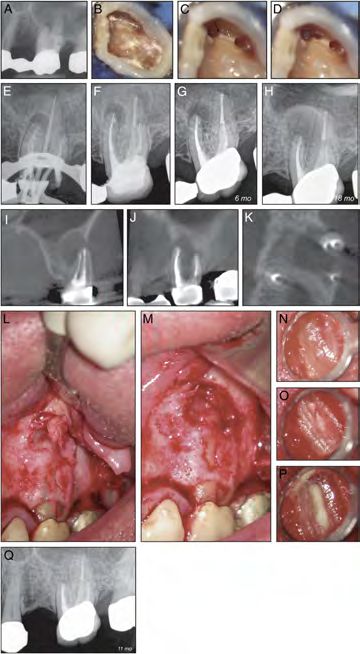
Quand les retreatments endo vous déçoit…
Succès Endodontique vue par GC
7 8
Problèmes où une approche chirurgicale est préférable
Fracture et fêlures radiculaires Testori & al 1993, Tamse & al 1999, Tawil et al 2015 2013 (JOE)
Infection persistante
Blockage du canal (Separated instruments, perforations, ledges, zips, strips, cements, etc)
Gorni & al 2004, Ray & al 1995, Tronstad & al 2000
Anatomie complex du canal (canal aberrations, bifurcations, isthmuses, lateral canals,
etc) Nair 2004, Nair & al 2005
Problèmes extra-radiculaires J. McIntyre
Infection extra-radiculaire Sundquvist & al 1980, Tronstad & al 1987, Sunde & al 2003, Ricucci & al 2008
11 months
Cysts Nair & al 1993, Simon 1998 Preop
Tumeur Simon 1998
Réaction à un matériel étranger Nair & al 1990, Nair 1998, Ricucci & al 1998
9 10
2015 (JOE)
2016 (JOE)
11 12
Avantage Endo PM - May 15, 2019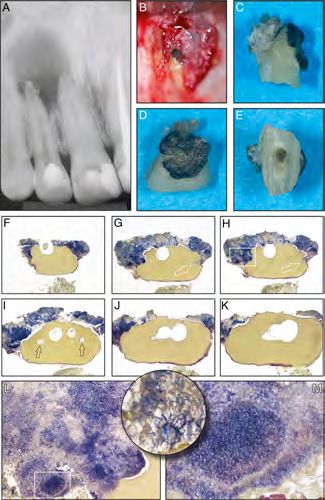
Techniques Modernes Micro-chirurgicales endo
VS
Techniques Traditionnelles
Apicoectomie: Résection de l’extrémité apicale de la racine
2013 (JOE)
Micro-chirurgie endo: Résection de l’extrémité apicale de
la racine, inspection de l’anatomie apicale, ablation des
fêlures/fractures, préparation ultrasonique et scellement
Le biofilm bactérien évolue avec le temps et devient plus biologique du système canalaire
resistant aux procédures traditionnel de désinfection endo
13 14
2006 (JOE)
2010 (JOE)
Difference significative due succès à 2 ans ✓ Meta-Analysis 1966-2009
✓ Micro-Sx: 94% succès
Techniques modern micro-sx: 91.1%
✓ Sx traditionnelles: 59% succès
Techniques traditionnelles: 44.2%
15 16
Histoire médicale qui risque Supplements “Naturelles”
d’affecter la guérison
Patients immunodéprimé: diabète, insuffisance rénale, etc
Marending et al 2005, Fouad 2003
INR > 3.5 (Aspirine, Plavix, Coumadin)
Aspirine à besoin de 10 jours
Herman 1997
Tabac peut retarder et affecter la guérison gingivale
Levin et al 2005
Hypertension et problèmes cardio-vasculaires
Wang CH 2011
Bisphosphonates
Karna H et al 2018, Soutome S et al 2018
17 18
Avantage Endo PM - May 15, 2019
Radiographie
Periapical radiographs:
2 PA minimum
Panoramique: Presurgical case planning to determine the exact
Pour les lésions extensives location of root apices and to evaluate the proximity of
adjacent vital anatomical structures
CBCT 3D: Identification of root canal system anomalies
Anatomie complex et structures vitales.
Assessment of endodontic treatment complications
Complex Diagnosis
19 20
Guides pour decider le traitement idéale
• Considérations du patient
• Considérations de la dent
Options de traitements
• Considérations du dentiste
• Considérations financières
21 22
Considération de la dent: No = Sx Considération de la dent: No = Sx
✓ Qualité de la couronne en place: Percolation? ✓ Qualité de la couronne en place: Percolation?
✓ Qualité du traitement de canal: Canal manqué? ✓ Qualité du traitement de canal: Canal manqué
✓ Anatomie osseuse: Risque de paresthésie?
23 24
Avantage Endo PM - May 15, 2019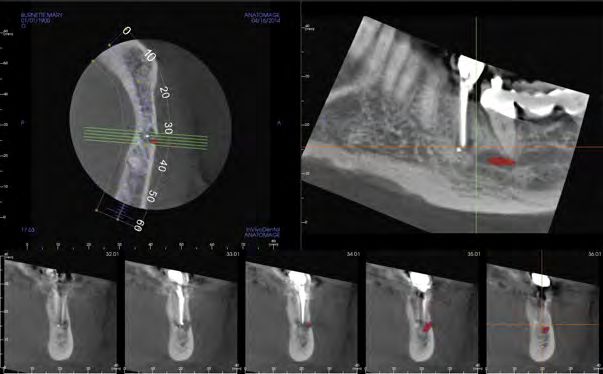
Considération de la dent: No = Sx
✓ Qualité de la couronne en place: Percolation?
✓ Qualité du traitement de canal: Canal manqué “We might as well retreat attitude”
✓ Anatomie osseuse: Risque de paresthésie?
✓ Conditions parodontales: Mobilité sévère?
25 26
JOE 2018
1980
La majorité des patients avec un fracture radiculaire son asymptotiques
•47 dents retx VS 48 SX traditionelles
•Suivi de 10.1 years
•Fractures radiculaires étaient plus fréquentes dans les dents
qui on rescue le retreatment de canal,
2001
4.5 années pour que la fracture radiculaire joigne la couronne de l’apex
27 28
JOE 2018
Les retraitements
de canal peuvent
causer des fêlures
radiculaires
•Les dents ave une histoire de
retraitement on plus de fêlure
radiculaires (p < 0.001)
•Odds ratio was 6.9 (95% confidence
interval)
•Multivariate regression model showed no La chirurgie endo est l’option la plus économique pour une durée de 5 ans
significance for: age, gender, tooth location
& treatment
Kim & Solomon 2010, JOE
29 30
Avantage Endo PM - May 15, 2019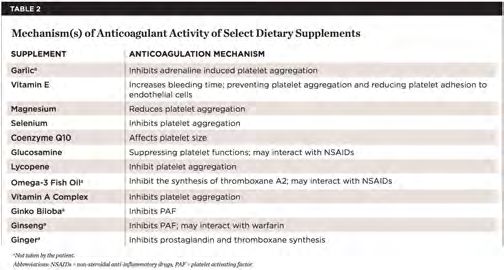
Replantation Intentionelle
Pour les molaires mandibulaires avec racine fusionnées
On ne touche pas la crypte osseuses après l’extraction
Guarder la dent dans du Hank’s balanced solution (Save-A- Tooth)
Option Chirurgicale alternative #1 Resection radiculaire et obturation rétrograde dans la solution
Replantation Intentionelle
“Splinting” est rarement nécessaire
Ajuster l’occlusion
RX Anti-inflammatoires et peridex
Niemczyk SP 2001, Kratchman S. 1997
31 32
Physics Forceps (GoldenDent)
Periotomes, Separators & Physics Forceps (GoldenDent)
33 34
Physics Forceps (GoldenDent) 3.7
Initial root canal therapy Retreat
Kirakozova A
35 36
Avantage Endo PM - May 15, 2019
Suivi
Post-op 1.5 ans
Kirakozova A Kirakozova A
37 38
Autotransplantation
Autotransplantation est parfois effectuée en ortho
On peut considérer l’utilization d’une dent de sagesse pour remplacer un première molaire
Pour les jeunes patients l’implant n’est pas une option due a la croissance osseuse
Option Chirurgicale alternative #2
Auto-transplantation Formation de la racine 1/3 à 2/3 (Foramen apical >1mm)
Extraction 1.6 Extraction 1.8
3rd molar in HBSS
Distal releasing incision
Yamauchi N
Yamauchi N
43 44
Dimensions de 1.8 pour ajuster site 1.6 Adjustments & placement final
Apex >1mm
Yamauchi N Yamauchi N
45 46
Post-op 3 months
Occlusion
Splint
EPT (-), Cold (+/-), Palpation (-), Percussion (-), Probing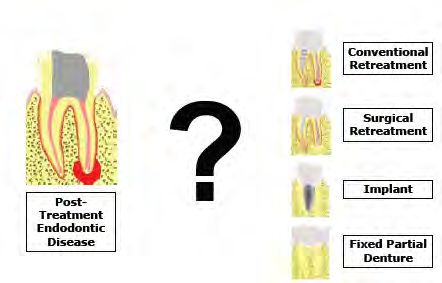
6 mois 1 an L’Adoption de la Chirurgie Endodontique
Etiologie, Diagnostic & Options de traitement
Styles de lambeaux gingival
Accès osseux, curettage & biopsie
Hémostase
Gestion de l'extrémité radiculaire
Résection radiculaire
Préparation rétrograde
Obturation rétrograde
Régénération parodontale
Sutures
Soins Post-op
EPT (+), Cold (+), Palpation (-), Percussion (-), ProbingRevue
Soft tissue de l’anatomie
management
Velvart et al.
as well as conservation and achievement of ‘white’ and stratum spinosum. The cells of the spinous la
largest in size and form the thickest layer of all ep
‘pink’ esthetics, in particular, in the more visible cells. Closer to the surface, the cells become fl
anterior jaw (11). ‘White esthetics’ refers to natural (stratum granulosum), whereas in the most sup
layer (stratum corneum) the cells are flat and
crown structures, or tooth-colored restorations of aligned, often without nuclei.
teeth with suitable materials. With restorative mod- The oral epithelium also contains Langerhan
also known as dendritic cells; they are mostly loc
alities, it is possible to obtain results, that come very the stratum spinosum. These cells play an imp
close to the natural look of teeth (12). Likewise, ‘pink role during the inflammation process as they bi
process antigens to the local lymph nodes and
esthetics’ refers to soft tissues and underlying bone, them to macrophages and lymphocytes (17). Ge
which are equally important for an optimal esthetic speaking, the oral epithelium, which is between
0.3 mm in thickness, has a largely protective fu
Jedmed
Rubinstein Retractor #1
result. (18).
Standard serrated flat Management of the periodontium with suitable
surgical and reconstructive techniques followed by SE: Sulcular
Fig. 2. Schematic drawing epithelium
of gingival histology; SE, Oral sulcular epithelium
long-term maintenance of the results are a great IP: Interdental
Fig. 1. Anatomy papilla
of a healthy gingival situation. IP, JE: Junctional
sulcular epithelium; epithelium
JE, junctional epithelium; OE, oral
CMG: Cervical
interdental papilla; CMG,marginal
cervicalgingiva
marginal gingiva
epithelium; PL, periodontal ligament; AB, alveolar bone; The sulcular epithelium makes up the linin
OE: tissue.
Oral epithelium
challenge in modern dentistry. The objective of AG: Attached gingiva CT, connective
PL: Periodontal ligament
gingival sulcus. A healthy sulcus extends to a d
with free marginal gingiva; AG, attached gingiva; MGJ,
MGJ: Mucogingival junction 0.5 mm. The sulcular epithelium is structurally
preserving the dentition is no longer acceptable with- AB: Aleveolar Bone
mucogingival junction; AM,mucosa
AM: Alveoloar alveolar mucosa. to the oral epithelium. The epithelial/connectiv
CT: Connective tissue
out consideration of esthetic consequences for all interface in the sulcus area forms rete pegs,
become elongated when inflammation is pres
involved dento-alveolar structures (13). contrast to the junctional epithelium, the s
The present article will address the tissue flap design Velvart 2005,
aging 0.97 mm, and a connective tissue attachment of Endod Topics epithelium is less permeable and not exte
infiltrated by polymorphonuclear leukocytes.
and the manipulation used to gain access to the 1.07 mm or in sum approximately 2 mm; this dimen- mostly protective functions.
55 underlining bone covering the roots, which are to be
treated surgically. Emphasis will be placed on the
sion is called the biologic width.
The papilla displays two peaks connected with a
56 Junctional epithelium
considerations of classical and modern soft tissue concave depression termed col. A papilla contains both The junctional epithelium is distinctly differen
sulcular and oral epithelium in both its orig
treatment modalities in order to fulfill the current non-keratinized sulcular and col epithelium as well as structure. In its most apical portion, the jun
functional and esthetic requirements. keratinized oral epithelium (14–16). The col area epithelium forms but few cell layers. The thick
the junctional epithelium increases gradually to
consists of a squamous stratified non-keratinized layers at the border to the sulcular epithelium. T
epithelium. of the stratum basale multiply rapidly an
reproduced cells tend to align themselves
Biology of the gingiva Fig. 3. Histology of the gingival epithelium/connective
to the long axis of the tooth and exfolia
the gingival sulcus. The interface between th
tissue interface. SB, stratum basale; SS stratum spinosum,
Gingival epithelium SG, stratum granulosum; SC, stratum corneum. Note the
tional epithelium and connective tissue is
The gingiva is one of four components of the period- marked extensions and depressions forming the rete straight. Migrating polymorphonuclear leukocy
ridges (courtesy Dr J. Gutmann). present throughout the junctional epithelium
ontium, which further comprises of periodontal liga- The gingival epithelium can be divided into three
migration process increases considerably duri
ment, alveolar bone, and cementum. Each of these different types based on their location and composition separates the epithelium from the subjacent connective development of an inflammatory process. In a
tissue. These rather small cells multiply continuously to polymorphonuclear leukocytes, T lymphocy
structures is distinct Soft in tissue
its location
managementand tissue archi- (14) (Fig. 2). The oral epithelium extends from the and as they mature into keratinizing cells, they form the then present (19).
tecture, but they function together as a single unit. One mucogingival junction to the tip of the gingival crest.
as well as conservation and achievement of ‘white’ and
‘pink’ esthetics, in particular, in the more visible component in a certain periodontal compartment can The sulcular epithelium is located between the gingival 80
anterior jaw (11). ‘White esthetics’ refers to natural influence the status of the adjacent structures. Conse- crest and the most coronal portion of the junctional
crown structures, or tooth-colored restorations of
teeth with suitable materials. With restorative mod- quently, pathological changes and injuries in one area of epithelium. The junctional epithelium extends from
alities, it is possible to obtain results, that come very the periodontium will have a marked effect on the the base of the gingival sulcus to a level approximately
close to the natural look of teeth (12). Likewise, ‘pink
esthetics’ refers to soft tissues and underlying bone, repair or regeneration of the adjacent periodontal 2 mm coronal from the alveolar bony crest. In a healthy
which are equally important for an optimal esthetic structures. situation without attachment loss, the junctional
result.
Journal of Perio 1992
Management of the periodontium with suitable
Anatomically, the extension of the gingiva reaches epithelium reaches the cemento-enamel junction. The Journal of Perio 1980
surgical and reconstructive techniques followed by from the papilla to the mucogingival junction, where it junctional epithelium is closely adapted to the tooth
long-term maintenance of the results are a great Fig. 1. Anatomy of a healthy gingival situation. IP,
challenge in modern dentistry. The objective of
joins the alveolar
interdental mucosa.
papilla; CMG, cervical It attaches
marginal gingivato the cementum surface to fulfill sealing and attachment functions.
with free marginal gingiva; AG, attached gingiva; MGJ,
preserving the dentition is no longer acceptable with- ofmucogingival
the teeth and AM,
junction; to the alveolar
alveolar mucosa. process (11, 14). The JOE 2011
La distance entre le point
involvedde contact et(13).
le niveaux osseux créstale
out consideration of esthetic consequences for all
gingiva is divided into three areas, namely free marginal
dento-alveolar structures
Oral gingival epithelium
inter-proximale est cruciale pour la hauteur de
The present article will address the tissue flap design gingiva,
and the manipulation used to gain access to the
la papille
aging 0.97papilla,
mm, and a and attached
connective gingivaof (Fig. 1). Histo-
tissue attachment
1.07 mm or in sum approximately 2 mm; this dimen-
underlining bone covering the roots, which are to be
logically, gingiva consists of superficial epithelial
sion is called the biologic width.
The oral epithelium is a stratified squamous keratinized Soft tissue management
treated surgically. Emphasis will be placed on the structures covering
The papilla displays underlining
two peaks connected withconnective
a tissue. epithelium, and four different cell layers can be
as well as conservation and achievement of ‘white’ and
5 mm du point
treatment de contact
modalities in order to➙ fulfill100%
the current papille
considerations of classical and modern soft tissue concave depression termed col. A papilla contains both
The attachment of the gingival tissues to the tooth
non-keratinized sulcular and col epithelium as well as
identified (Fig. 3). The cells of the stratum basale
‘pink’ liein particular, in the more visible
esthetics,
anterior jaw (11). ‘White esthetics’ refers to natural
6 mm du point de contact ➙ 56% papille
functional and esthetic requirements. comprises
keratinized oralof junctional
epithelium epithelium
(14–16). attachment,
The col area aver- in close contact with the basement membrane, which or tooth-colored restorations of
crown structures,
consists of a squamous stratified non-keratinized
Les changement parodontales peuvent prendre 1
teeth with suitable materials. With restorative mod-
7 mm du point de contact ➙ 27% papille
epithelium.
Velvart et al.
alities, it is possible to obtain results, that come very
Biology of the gingiva an après a chirurgie
close to the natural look of teeth (12). Likewise, ‘pink
79to soft tissues and underlying bone,
esthetics’ refers
Gingival epithelium general agreement that the same basic principleswhich applyare equally important for an optimal esthetic
The gingiva is one of four components of the period-
ontium, which further comprises of periodontal liga- The gingival epithelium can be divided into three to endodontic surgical interventions (37, 69). result.
ment, alveolar bone, and cementum. Each of these different types based on their location and composition Management of the periodontium with suitable
The choice of flap designs should allow the main-
surgical and reconstructive techniques followed by
structures is distinct in its location and tissue archi- (14) (Fig. 2). The oral epithelium extends from the tenance of optimal and sufficient blood supplylong-term
to all maintenance of the results are a great Fig. 1. Anatomy of a healthy gingival situation. IP,
tecture, but they function together as a single unit. One mucogingival junction to the tip of the gingival crest. parts of the mobilized and nonmobilized portions of in modern dentistry. The objective of interdental papilla; CMG, cervical marginal gingiva
challenge
component in a certain periodontal compartment can The sulcular epithelium is located between the gingival with free marginal gingiva; AG, attached gingiva; MGJ,
57 the soft tissues (37, 39, 55, 56, 69). This implies
58
preserving the dentition is no longer acceptable with- mucogingival junction; AM, alveolar mucosa.
influence the status of the adjacent structures. Conse- crest and the most coronal portion of the junctional out run
consideration of esthetic consequences for all
specifically that vertical releasing incisions should
Velvart et al. quently, pathological changes and injuries in one area of epithelium. The junctional epithelium extends from involved dento-alveolar structures (13).
the periodontium will have a marked effect on the the base of the gingival sulcus to a level approximately vertical, parallel to the long axis of the teethThe andpresent article will address the tissue flap design aging 0.97 mm, and a connective tissue attachment of
repair basic
or regeneration of the adjacent periodontal 2 mm coronal from the alveolar bony crest. In a healthy supraperiosteal blood vessels in the gingivaandand the manipulation used to gain access to the 1.07 mm or in sum approximately 2 mm; this dimen-
general agreement that the same principles apply
structures. situation without attachment loss, the junctional mucosa. Paramedian releasing incisions are recom- underlining bone covering the roots, which are to be sion is called the biologic width.
to endodontic surgical interventions (37, 69). treated
Anatomically, the extension of the gingiva reaches epithelium reaches the cemento-enamel junction. The mended to minimize the risk of recession (39). The surgically. Emphasis will be placed on the The papilla displays two peaks connected with a
The choice of flap designs should allow the main-
from the papilla to the mucogingival junction, where it junctional epithelium is closely adapted to the tooth considerations of classical and modern soft tissue concave depression termed col. A papilla contains both
initial portion of the vertical incision should be placed
tenance of optimal and sufficient treatment modalities in order to fulfill the current non-keratinized sulcular and col epithelium as well as
joins theblood
alveolarsupply
mucosa.toItall
attaches to the cementum surface to fulfill sealing and attachment functions. perpendicular to the marginal course of the gingiva functional and esthetic requirements. keratinized oral epithelium (14–16). The col area
parts of the mobilized and of nonmobilized
the teeth and to portions of process (11, 14). The
the alveolar toward the mid section of the papilla and gradually consists of a squamous stratified non-keratinized
the soft tissues (37, 39, 55, 56,is 69).
gingiva dividedThis implies
into three areas, namely free marginal epithelium.
Oral gingival epithelium turning the incision parallel to the tooth axis (Fig. 25).
gingiva,incisions
specifically that vertical releasing papilla, and attached
should run gingiva (Fig. 1). Histo-
logically, gingiva consists
Adequate micro-configuration of the gingival marginsBiology of the gingiva
vertical, parallel to the long axis of the teeth andof superficial epithelial The oral epithelium is a stratified squamous keratinized
will minimize any potential recession of the tissues. Gingival epithelium
structures covering underlining connective tissue. epithelium, and four different cell layers can be The gingiva is one of four components of the period-
supraperiosteal blood vessels in the gingiva and Postoperative results are also influenced by the which further comprises of periodontal liga- The gingival epithelium can be divided into three
The attachment of the gingival tissues to the tooth identified (Fig. 3). The cells of the stratum basale lie ontium,
mucosa. Paramedian releasing incisions are recom-
comprises of junctional epithelium attachment, aver- in close contact with the basement membrane, which amount of tissue shrinkage. With prolonged duration ment, alveolar bone, and cementum. Each of these different types based on their location and composition
mended to minimize the risk of recession (39). The structures
of the surgical procedure, there is a risk of drying out of is distinct in its location and tissue archi- (14) (Fig. 2). The oral epithelium extends from the
initial portion of the vertical incision should be placed tecture, but they function together as a single unit. One mucogingival junction to the tip of the gingival crest.
the tissues, especially when a high degree of hemostasis
perpendicular to the marginal course of the gingiva 79 component in a certain periodontal compartment can The sulcular epithelium is located between the gingival
has been achieved. The tissues must be kept moist at all the status of the adjacent structures. Conse- crest and the most coronal portion of the junctional
influence
toward the mid section of the papilla and gradually time to help avoid shrinkage and dehydrationquently, (70). pathological changes and injuries in one area of epithelium. The junctional epithelium extends from
turning the incision parallel to the tooth axis (Fig. 25). the
This can be particularly problematic in submarginal flap periodontium will have a marked effect on the the base of the gingival sulcus to a level approximately
Adequate micro-configuration of the gingival margins repair or regeneration of the adjacent periodontal 2 mm coronal from the alveolar bony crest. In a healthy
design, resulting in difficult flap re-approximation, with
structures. situation without attachment loss, the junctional
will minimize any potential recession of the tissues. Velvart et al. more tension on the tissues. Minimal tension during re-
Anatomically, the extension of the gingiva reaches epithelium reaches the cemento-enamel junction. The
Postoperative results are also influenced by the approximation and after suturing is important tofrom avoidthe papilla to the mucogingival junction, where it junctional epithelium is closely adapted to the tooth
amount of tissue shrinkage. With prolonged duration impairment of the circulation in the wound margins joins the alveolar mucosa. It attaches to the cementum surface to fulfill sealing and attachment functions.
general agreement that the same basic principles apply of the teeth and to the alveolar process (11, 14). The
of the surgical procedure, there is a risk of drying out of (56). Shrinkage of the reflected tissue with wound
the tissues, especially when a high degree of hemostasis
to endodontic surgical interventions (37, 69). gingiva is divided into three areas, namely free marginal
dehiscence will ultimately lead to increasedgingiva, scar papilla, and attached gingiva (Fig. 1). Histo- Oral gingival epithelium
has been achieved. The tissues must be kept moist at all The choice of flap designs should allow the main- formation. logically, gingiva consists of superficial epithelial The oral epithelium is a stratified squamous keratinized
time to help avoid shrinkage and dehydration (70). tenance of optimal and sufficient blood supply to all Tissue trauma such as stretching, tearing, or distor-
structures covering underlining connective tissue. epithelium, and four different cell layers can be
This can be particularly problematic in submarginal flap parts of the mobilized and nonmobilized portions of The attachment of the gingival tissues to the tooth
tion should be avoided through appropriate magnifica- identified (Fig. 3). The cells of the stratum basale lie
comprises of junctional epithelium attachment, aver- in close contact with the basement membrane, which
design, resulting in difficult flap re-approximation, with the soft tissues (37, 39, 55, 56, 69). This implies tion and careful manipulation with microsurgical
more tension on the tissues. Minimal tension during re- specifically that vertical releasing incisions should run instruments (71, 72). The elevation process following
approximation and after suturing is important to avoid the incision is aimed at undermined elevation of the 79
c diagram of a cross-section of the vertical, parallel to the long axis of the teeth and
lla. L, lingual; B, buccal, red area Fig. 5. Schematic Gutmann
impairment
drawingofofthe1991
circulation
gingival bloodin the wound margins
vessels. Velvart 2005 periosteum. In order to enhance regeneration of the
supraperiosteal blood vessels in the gingiva and
helium; AB, alveolar bone; DGF, Reprinted with(56). Shrinkage
permission fromof the reflected tissue with wound
(77). bone and periodontal ligament over the resected root
bers; TSF, transseptal fibers; DPF, dehiscence will ultimately lead to increased scar
mucosa. Paramedian releasing incisions are recom- surface, certain cells have to be prevented from
Gutmann).
• La vascularization sanguine est parallèle a l’axe de la dent
fibers; AGF, alveolargingival fibers formation. mended to minimize the risk of recession (39). The
initial portion of the vertical incision should be placed
repopulating the bony defect (73). When the integrity
Tissue trauma such as stretching, tearing, or distor- of the periosteum has been maintained, it will serve as a
• L’incision verticale doit être parallèle a cet axe pour minimizer the saignement
tion should be avoided through appropriate magnifica-
tion and careful manipulation with microsurgical
perpendicular to the marginal course of the gingiva barrier against the connective tissue cells, so that these
cells cannot invade the bone cavity during the healing
toward the mid section of the papilla and gradually
nd fibroblasts. Numerous studies in-
• L’incision verticale doit éviter les éminences osseuse
instruments (71, 72). The elevation process following process and prevent a complete bone fill. Scaling of root Fig. 25. Vertical releasing incisions. (A) Incorrect
turning the incision parallel to the tooth axis (Fig. 25).
phocytes exert a significant cytotoxic the incision is aimed at undermined elevation of the attached tissue and tissueIncorrect
tags on the cortical bone straight vertical incisionCorrect creates compromised tissue area
Adequate micro-configuration of the gingival margins with insufficient blood supply, which will eventually
l fibroblasts either through the release periosteum. In order to enhance regeneration of the should be avoided to allow rapid reattachment and necrose. (A) dashed line indicates the desired incision
will minimize any potential recession of the tissues. protection against bone resorption (37, 55, 74). After
ators or via direct cell-to-cell contact bone and periodontal ligament over the resected root course. Reprinted with permission from (7). (B) Correct
should the balance between bacteria
Postoperative results are also influenced by the reflecting the mucogingival tissues, a retractor must be placement of the releasing incision perpendicular to the
surface, certain cells have to be prevented from
amount of tissue shrinkage. With prolonged duration placed securely on sound bone to prevent compression marginal contour of the gingiva shown in a schematic
e shift unfavorably, uncontrolled tissue repopulating the bony defect (73). When the integrity diagram (B), reprinted with permission from (3). (C)
take place and the inflammation may of the periosteum has been maintained, it will serve as a of the surgical procedure, there is a risk of drying out of Clinical example of a correctly placed incision.
into the periodontal ligament and barrier against the connective tissue cells, so that these the tissues, especially when a high degree of hemostasis
92 Velvart 2005, Endod Topics
esulting in attachment loss in conjunc- cells cannot invade the bone cavity during the healing has been achieved. The tissues must be kept moist at all
process and prevent a complete bone fill. Scaling of root Fig. 25. Vertical releasing incisions. (A) timeIncorrect
to help avoid shrinkage and dehydration (70).
migration of the junctional epithelium. straight vertical incision creates compromised tissue area
attached tissue and tissue tags on the cortical bone
should be avoided to allow rapid reattachment and
Fig. 6. Dental radiograph of a first mandibular molar
59 with insufficient blood supply, which will This
necrose. (A) dashed line indicates the desired
can be particularly problematic in submarginal flap
eventually
design, resulting in difficult flap re-approximation, with
incision
60
protection against bone resorption (37, 55, 74). After course. Reprinted with permission from (7). (B) Correct
with a radiolucent lesion on the distal root. The mental more tension on the tissues. Minimal tension during re-
foramen is not reflecting
visible. the mucogingival tissues, a retractor must be
placed securely on sound bone to prevent compression
placement of the releasing incision perpendicular to the
marginal contour of the gingiva shown inapproximation
a schematic and after suturing is important to avoid Avantage Endo PM - May 15, 2019
sue reaches from the papilla to the diagram (B), reprinted with permission from (3). (C) of the circulation in the wound margins
impairment
unction, where it joins the alveolar gradually changes its appearance toward the character- Clinical example of a correctly placed incision.
(56). Shrinkage of the reflected tissue with wound
). The height of the gingiva from the 92
istics of the epithelial cuff (epithelial attachment). The dehiscence will ultimately lead to increased scar
nction to the gingival margin is highest width of the col between the buccal and lingual papilla93
Mini “baby” flaps doit être guidé avec 3D CBCT
Votre “Minnesota” doit toujours est sur l’os
causing distinct damage. and the cols were less concave.
(arrow). Note the tissue squeezed under the instrument not fill the embrasure as completely as before excision,
Fig. 26. Traumatic placement of tissue retractors
height. The regenerated papillae appeared flatter, did
papillae did not regenerate to their original shape and
posterior area of each student. From 32 specimens, 22
students: one from the anterior and one from the
Holmes (33) excised interdental papillae in 16 dental
the microsurgical techniques used.
after 1 and 3 months and more importantly in spite of
results in considerable retraction of the papilla height
These results indicate that the traditional sulcular flap
compared with the 1-month value (0.2 ! 0.3 mm).
10 sites, while in three sites the loss had diminished
(1.1 ! 0.8 mm). At 3 months retractions increased in
between baseline and the 1-month recall
and 3 months. Major loss of the papilla height occurred
sites exhibited a significant loss of the papilla height at 1
Velvart 2005,
following microsurgical Endod
treatment Topics
in endodontic sur- again periodontally healthy situations.
Moiseiwitsch 1995 All experimental
Studies have highlighted the healing of the papilla study analyzed the recession of the interdental papilla in
loss. tive levels at any time. Subsequently, a quantitative
the buccal papilla is often difficult and may lead to tissue phase. None of the 17 sites remained at the preopera-
In narrow interproximal areas, complete dissection of papillary height increased gradually in the initial healing
from the lingual papilla in the area of the col (Fig. 27). of the papilla was investigated (81). The reduction in
Ideally, a sulcular incision should dissect the buccal 61 papillae after sulcular flaps with complete mobilization 62
papilla is mobilized and becomes part of the flap (76). recession of the gingiva. Preliminarily, shrinkage of the
is a full-thickness marginal flap. In this flap design, the challenging situation – with the goal of preventing a
The most frequently used flap in periradicular surgery outcome in healthy periodontal tissues – a most
periodontal reconstructive surgery (11). geries (64, 77–80). Specific emphasis was placed on the
interdental papillae is one of the greatest challenges in
reasons. Complete and predictable restoration of lost
is critical for aesthetic, functional, and phonetic
blade. Reprinted with permission from (3).
integrity of the papilla during dental treatment is that it Fig. 27. Dissection of the papilla using a microsurgical
ment (75). Another important reason to respect the
cementum, and alveolar bone from the oral environ-
biological barrier that protects periodontal ligament,
reality, the role of the papilla is more complex: it is a
have the sole function of deflecting food debris. In
between two adjacent teeth. It was long considered to
The interdental papilla is the portion of the gingiva
Papilla preservation and protection
Mini “baby” flaps doit être guidé avec 3D CBCT Mini “baby” flaps doit être guidé avec 3D CBCT
positioned (3).
with a small round bur in which the retractor can be
tissue slipping under the retractor, a fine groove is made
and delayed healing. As a practical measure to avoid
trauma from retraction may cause increased swelling
or crushing of the soft tissue (Fig. 26). Excessive
Soft tissue management
63 64
Lambeau Triangulaire Lambeau Rectangulaire
Pour les dents postérieures Biotype favorable et < 5mm hauteur de papille
Symétrie est critique pour les dents antérieures
Practical Lessons in Endodontic Surgery Practical Lessons in Endodontic Surgery
Arens, Torabinejad, Chivian, Rubinstein Arens, Torabinejad, Chivian, Rubinstein
65 66
Avantage Endo PM - May 15, 2019Soft tissue management
connective tissue without meeting resistance to a level Flap design
where a stop is encountered, which can be either bone
When designing a tissue flap, various modes of incision
or deeper collagen fibers in the connective tissue. This
can be selected, including horizontal, sulcular, sub-
results in an overestimation of the ‘true’ depth of
marginal, and vertical releasing incisions. The tissue
pocket. Another reason for potential overestimation of
flap in its entirety can be a full-thickness or a
pocket depth is the presence of tissue swelling. There-
combination of a full- and a split-thickness flap.
fore, bleeding on probing has to be assessed in the
Consequently, a number of flap designs exist and are
evaluation process. The degree of inflammation is
discussed in the literature, including specific rules and
correlated to the amount of bleeding. As the inflam-
recommendations (3, 50–53). The variety of flap
matory process is mainly plaque induced, attempts
designs reflects a number of variables to be considered.
should be made to reduce the inflammatory process
While many designs have been suggested over the
presurgically. This can be achieved through increased
and improved plaque control prior to the surgery.
Plaque reduction includes professional measures by a
Soft tissue management
dental hygienist and meticulous oral hygiene by the
connective tissue without meeting resistance to a levelpatient.
Flap In general,
designit may be advisable to prescribe a
where a stop is encountered, which can be either bone0.2% chlorhexidine rinse twice daily 1 week before and
When designing a tissue flap, various modes of incision
or deeper collagen fibers in the connective tissue. This2 weeks after the surgery. Chlorhexidine reduces
can be selected, including horizontal, sulcular, sub-
results in an overestimation of the ‘true’ depth ofplaque growth significantly (44, 45), reduces post-
marginal, and vertical releasing incisions. The tissue
pocket. Another reason for potential overestimation ofoperative discomfort, and promotes healing (46, 47).
flap in its entirety can be a full-thickness or a
pocket depth is the presence of tissue swelling. There-Moreover, rinsing with chlorhexidine markedly reduces
combination of a full- and a split-thickness flap.
fore, bleeding on probing has to be assessed in thethe bacterial load and contamination of the operative
Consequently, a number of flap designs exist and are
evaluation process. The degree of inflammation isarea, operator and staff (48).
discussed in the literature, including specific rules and
Submarginal flap correlated to the amount of bleeding. As the inflam-
matory process is mainly plaque induced, attempts
Therecommendations
presence, type, and(3, quality
50–53). ofTherestorations
variety ofwith
flap
Submarginal flap
special reference
designs reflectsto the position
a number of the
of variables to berestoration
considered.
should be made to reduce the inflammatory process
marginWhileto the
manygingiva
designsmust
have be determined
been suggested and
over are
the
presurgically. This can be achieved through increased
Biotype défavorable avec gencive attaché de 2mm our plus critical to the esthetic outcome of the surgical
and improved plaque control prior to the surgery.
Plaque reduction includes professional measures by procedure.
a Manipulations on soft tissues in areas with
Risque de cicatrice: Pas recommandé pour les sourires qui expose la gencive
dental hygienist and meticulous oral hygiene by therestoration margins placed subgingivally for esthetic
patient. In general, it may be advisable to prescribe reasons
a can lead to exposure of these margins because
0.2% chlorhexidine rinse twice daily 1 week before andof recession following the surgery (Fig. 13). How to
2 weeks after the surgery. Chlorhexidine reducesaddress this problem will be discussed extensively at a
plaque growth significantly (44, 45), reduces post-later point in this article.
operative discomfort, and promotes healing (46, 47). The determination of the attached gingival width is
Moreover, rinsing with chlorhexidine markedly reducesanother important aspect in making the proper
the bacterial load and contamination of the operative
treatment plan with regard to the flap design. When a
area, operator and staff (48).
submarginal incision is considered, a minimum of
The presence, type, and quality of restorations with
2 mm of attached gingiva is necessary to maintain a
special reference to the position of the restoration
margin to the gingiva must be determined and arestable position of the gingival margin (49). When a
critical to the esthetic outcome of the surgicalsubmarginal incision has been made, the marginal
procedure. Manipulations on soft tissues in areas withgingiva in the cervical area is supplied with blood from
restoration margins placed subgingivally for estheticcrestal vessels and to a minor extent from the period-
Fig. 14. Determination of the width of the attached
reasons can lead to exposure of these margins becauseontal ligament (34). Insufficient blood supply com-
gingiva. (A) Measurement of the probing depth. The
of recession following the surgery (Fig. 13). How topromises the survival of the unreflected tissue and can gingival tissue over the probe represents the free gingiva.
Papilla base incision P. Velvart
address this problem will be discussed extensively at lead
a to necrosis and the potential for a deleterious Probing depth is designated by arrows. (B) Arrows mark
later point in this article. esthetic result. Clinically, the width of attached gingiva the mucogingival line. The distance between the tip of the
The determination of the attached gingival width iscan be determined by subtracting the probing depth probe (representing the probing depth) and the
incision using a microsurgical blade (BB
Practical 369, Aesculap,
Lessons in Endodontic Surgery another important aspect in making the proper mucogingival junction is the width of the attached
from the distance between the gingival margin and the gingiva. The dashed line represents the location for a
Tuttlingen, Germany). The Arens,2.5 mm Torabinejad,
wide blade with a
Chivian, Rubinstein treatment plan with regard to the flap design. When a Velvart 2005, Endod Topics
mucogingival junction (Fig. 14). proper placement of a submarginal incision.
round configuration at the tip has cutting edges on both submarginal incision is considered, a minimum of
sides and all around the tip. The papilla base incision 2 mm of attached gingiva is necessary to maintain a
required two different incisions at the base of the papilla. stable position of the gingival margin (49). When a
1 The first shallow incision severed the epithelium and
connective tissue to the depth of 1.5 mm from the surface
67 submarginal incision has been made, the marginal
gingiva in the cervical area is supplied with blood from
68 87
of the gingiva. The incision was placed at the level of the crestal vessels and to a minor extent from the period-
Fig. 14. Determination of the width of the attached
ontal ligament (34). Insufficient blood supply com-
lower third of the papilla in a slight curved line going gingiva. (A) Measurement of the probing depth. The
promises the survival of the unreflected tissue and can gingival tissue over the probe represents the free gingiva.
from one side of the papilla to the other (Fig. 1). The
lead to necrosis and the potential for a deleterious Probing depth is designated by arrows. (B) Arrows mark
incision started and ended in a 90 degree angle between the mucogingival line. The distance between the tip of the
esthetic result. Clinically, the width of attached gingiva
the border of the tooth and the gingiva (see lines in probe (representing the probing depth) and the
can be determined by subtracting the probing depth
Fig. 1). mucogingival junction is the width of the attached
from the distance between the gingival margin and the gingiva. The dashed line represents the location for a
2 The scalpel was then placed to the base of the mucogingival junction (Fig. 14). proper placement of a submarginal incision.
previously created shallow incision at the base of the
papilla and subsequently inclined apically, almost
parallel to the long axis of the tooth, aiming at the crestal 87
bone margin. With this second incision a split thickness
flap was prepared in the apical third of the base of the
papilla. The incision ended at the crestal bone level,
where the periosteum was separated from the bone
(Fig. 2). From there on the preparation continued in a full
thickness muco periosteal flap (Fig. 3). Buccally over the Figure 2 Schematic drawing of the longitudinal section
tooth the vertical incision and papilla base incision were through the interdental papilla. *marks the initial shallow
Incision “Papilla base”
joined by an intrasulcular incision. The scalpel was incision through the epithelium and connective tissue to the
moved within the sulcus, dissecting the gingiva to the depth of 1.5 mm. **demonstrates the second incision directed to
the crestal bone. The scalpel blade is inserted into the base of the
crestal bone. The sulcular Pour lesreached
incision scenarios
from the défavorables.
first incision and directed nearly parallel to the long axis of the Guérison de l’incision “Papilla Base”
releasing incision to the start of the papilla base incision,
Biotype défavorable, gencive attaché limitée
tooth. et longe
The second incision
Papilla base incision P. Velvart papille
will prepare a split thickness flap
reaching from the first incision to the crestal bone level.
Papilla base incision P. Velvart
incision using a microsurgical blade (BB 369, Aesculap, P.P.Velvart
Velvart Papilla
Papillabase
baseincision
incision
Tuttlingen, Germany). The 2.5 mm wide blade with a
round configuration at the tip has cutting edges on both or from one papilla to the next papilla. The flap was
sides and all around the tip. The papilla base incision mobilized and retracted, during the root-end resection
required two different incisions at the base of the papilla.
1 The first shallow incision severed the epithelium and
and filling.
connective tissue to the depth of 1.5 mm from the surface The flap closure was initiated from the releasing inci-
of the gingiva. The incision was placed at the level of the sions. For the vertical incisions 6/0 (Supramid, B. Braun,
lower third of the papilla in a slight curved line going
from one side of the papilla to the other (Fig. 1). The
Neuhausen, Switzerland) interrupted polyamide sutures
incision started and ended in a 90 degree angle between were used. The papilla base incision was sutured with
the border of the tooth and the gingiva (see lines in two or three polypropylene 7/0 (Prolene, Ethicon, Nor-
Fig. 1).
2 The scalpel was then placed to the base of the
derstedt, Germany) interrupted sutures depending on
previously created shallow incision at the base of the the width of the papilla. Great care was taken in passive
papilla and subsequently inclined apically, almost reapproximation and perfect adaptation of the wound post-op 1 month post-op 1 week 1 month
parallel to the long axis of the tooth, aiming at the crestal
bone margin. With this second incision a split thickness
margins without tension to the sutures (Fig. 4a). The
Figure Incompletehealing.
5 5Incomplete healing.Clearly
Clearlydetectable
detectableincision
incision
flap was prepared in the apical third of the base of the flap was compressed for 1 min at the conclusion of the Figure Figure 8 Tissue irritation at suture removal. (a) Post surgery;
wound.
wound. (a)(a) Post
Post surgery;(b)
surgery; (b)healing
healingatat11month.
month.
papilla. The incision ended at the crestal bone level, surgery. Patients were instructed to apply a cold com- (b) before suture removal; (c) healing at 1 month.
where the periosteum was separated from the bone
press to the face for 10 min every 30 min for the rest of
(Fig. 2). From there on the preparation continued in a full
the day and were prescribed NSAID (Ponstan, Parke Davis, 1 1before
beforesurgery;
surgery;
Figure 1 Papilla thickness
base flapmuco periosteal
consisting of flap
two(Fig. 3). Buccally
releasing over the
incisions Figure 2 Schematic drawing of the longitudinal section
four sites with visible defects (grade 1), seven sites with
tooth the vertical incision and papilla base incision were Baar, Switzerland),
through 250
the interdental papilla. mgthethree
*marks times per day for 48 h.
initial shallow 2 2immediately
immediately
Figure 6 Partially complete postoperatively;
healing. There are areas in which
postoperatively;
and the papilla base incision. The papilla base incision is placed 3 3can
atat
33toto5still
5days
daysafter
aftersuture
sutureremoval;
removal; and
joined by an intrasulcular incision. The scalpel was incision through the epithelium and connective tissue to the
Following this, patients only the incision be detected, where as inand
other parts the partially detectable incision defect (grade 2) and nine
in the lower thirdmoved
of thewithin
interdental papilla. The incision starts depth of 1.5 mm. **demonstrates the second incisiontook
directedthe
to analgesics 4 at a recall appointment 1 month postoperatively.
the sulcus, dissecting the gingiva to the
Velvart 2002the 4 at a recall appointment
healing is undetectable. (a) Post 1 month(b)
postoperatively. sites with perfect healing (grade 3).
and ends at a 90 degree angleThe
crestal bone. (seesulcular
lines) toincision
the gingival
reached margin,
from the when crestalrequired. Patients
bone. The scalpel wereinto
blade is inserted instructed to refrain from
the base of the Great care was takensurgery;
to maintain healing
the at 1 month.
same angulation
Great care was taken to maintain the same angulation
resulting in a curved lineincision
releasing at the base
to theof theofpapilla.
start the papilla base incision,
first incision and directed nearly parallel to the long axis of the
mechanical oral hygiene in the operated area and rinse
tooth. The second incision will prepare a split thickness flap
and magnification of the photographs. The photographs
and magnification of the photographs. The photographs
Velvart 2002
reaching from the first incision to the crestal bone level. were digitized in a slide scanner (LS 2000, Nikon Corpo-
were digitized in a slide scanner (LS 2000, Nikon Corpo-
ration, Japan), imported as TIFF files into the Photoshop
ration, Japan), imported as TIFF files into the Photoshop
Discussion
Figure 3 Clinical photograph after complete reflection of the 6.0 (Adobe Systems Incorporated, USA) and the pictures
456 International Endodontic Journal, 35, 453 –460, 2002
69 or from one papilla to the next papilla. The
and filling.
© 2002flapBlackwell
mobilized and retracted, during the root-end resection
was Science Ltd
Figure 3 Clinical photograph after complete reflection of the
papilla base flap. Note the elevated split thickness flap from the
papilla base flap. Note the elevated split thickness flap from the
incision to the crestal bone level. Apical to the crestal bone area
incision to the crestal bone level. Apical to the crestal bone area
6.0 (Adobe Systems Incorporated, USA) and the pictures
enlarged to 3× magnification. The images were compared
enlarged to 3× magnification. The images were compared
for increase of the space between the papilla and contact
70
It is of utmost importance to preserve epithelial and
connective tissue attachment at its original level and
the full thickness flap exposes the bone over the roots. for increase of the space between the papilla and contact
The flap closure was initiated from the releasing inci- the full thickness flap exposes the bone over the roots. area as a sign of loss of height. The change of the position
area as a sign of loss of height. The change of the position
of the most coronal point of the papilla was determined by
traumatize the attachment apparatus as little as possible
sions. For the vertical incisions 6/0 (Supramid, B. Braun,
Neuhausen, Switzerland) interrupted polyamide sutures ofmeasuring
the most coronal point of
the distance the papilla
between was determined
a reproducible point by
during the incision in order to obtain rapid healing
on
were used. The papilla base incision was sutured with measuring the papilla
distance tipbetween a reproducible
probe. The point on
the tooth and using a perio through primary intention. This can be obtained by:
precision
two or three polypropylene 7/0 (Prolene, Ethicon, Nor- the
oftooth and papilla tipreading
the measurement using a perio
was anprobe. The precision
approximation to
derstedt, Germany) interrupted sutures depending on of0.5
themm.
measurement reading was an approximation 1 complete and sharp incision of the tissues;
to
Wound healing complications, such as excessive
the width of the papilla. Great care was taken in passive 0.5 mm. Wound
swelling, healingwound
infections, complications,
dehiscencesuchand 2 avoiding crushing of the tissues;
as excessive
necrosis,
reapproximation and perfect adaptation of the wound
swelling, infections,
were recorded wound
at all times. dehiscence
Probing and measured
depths were necrosis,
3 preventing drying of the tissues during the procedure; and
margins without tension to the sutures (Fig. 4a). The
flap was compressed for 1 min at the conclusion of the were recorded
at recall at all times.except
appointments, Probing depths
at the were
suture measured
removal.
at recall
4 perfect adaptation of wound edges upon closure
surgery. Patients were instructed to apply a cold com- One appointments, except at the
month post operatively thesuture removal.sites
experimental
press to the face for 10 min every 30 min for the rest of One observed
were month post withoperatively the experimental
a 3× magnification (Gutmann & Harrison 1991b).
and graded sites
as to
the day and were prescribed NSAID (Ponstan, Parke Davis,
Figure 1 Papilla base flap consisting of two releasing incisions were observed
whether withdefect
a visible a 3× magnification
resulting from the andincision
graded couldRecession of the papilla after sulcular incisions has not
as to
Baar, Switzerland), 250 mg three times per day for 48 h.
and the papilla base incision. The papilla base incision is placed whether a visible
be detected. defect resulting
Incomplete healingfrom the incision
(grade coulda
1) described
in the lower third of the interdental papilla. The incision starts Following this, patients only took the analgesics been discussed recently. It remains however, an import-
when required. Patients were instructed to refrain from
be detected. Incomplete healing (grade 1) described
clearly visible defect along the entire incision (Fig. 5b). a
and ends at a 90 degree angle (see lines) to the gingival margin, Figure 7 Perfect
clearly healing.
visible
Partially
Thehealing
defect
complete
placethe
along of the incision
entire
(grade 2)incision
can
was noted,
ant problem, which cannot be corrected in a predictable
(Fig.not
5b).be
when
resulting in a curved line at the base of the papilla. mechanical oral hygiene in the operated area and rinse
Figure 4 (a) Wound closure of the papilla base incision detected.
with (a) Postofsurgery;
Partially
parts complete (b)
the incision healing
healing
were (gradeat 12)
visible month.
and was noted,
at the same manner. Although advanced restorative procedures and
when
time
three
Figure 4 polypropylene sutures;
(a) Wound closure (b) sutures
of the removed
papilla base afterwith
incision 4 days. parts
thereofwere
the also
incision
areaswere
withvisible and athealing
undetectable the same time
patterns
materials have expanded the therapeutic options, anter-
456 International Endodontic Journal, 35, 453–460, 2002 © 2002 Blackwell Science Ltd three polypropylene sutures; (b) sutures removed after 4 days. (Fig.were
there 6b). also
Perfect healing
areas with(grade 3) was given
undetectable forpatterns
healing undetec-
table incision
ior hard and soft tissue deformities continue to represent
(Fig. 6b). Perfectlines (Fig.(grade
healing 7b). 3) was given for undetec-
twice daily with 0.2% chlorhexidine during the first occurred. Oneincision
week table patient exhibited
lines (Fig. 7b). delayed healing at suture a significant technical and aesthetic challenge (Salama
Conclusion des lambeaux
after
twice thewith
daily
post
after
surgery.
0.2%The
theoperatively
sutures were
chlorhexidine
(Fig.sutures
surgery. The 4b).
removed
during 3removal
the first
were removed 3 – 5 days
–week
Results L’Adoption de la Chirurgie Endodontique
5 days along the entire margin of the flap, leading et al. 1998). When semilunar flaps were compared with
to visible and persistent scar formation. Three other trapezoidal flaps, no statistically significant change was
Twenty sites
post operatively were
(Fig. evaluated. The surgical areas were Results
4b). Complete closure of the wound was achieved in all cases
photographed
Twenty perpendiculy
sites were evaluated.toThe
the surgical
interproximalpatients
areas area:
were
displayed irritation
and no closure
Complete severe around
complications
of the wound was
the
suchachievedsutures
as papilla at the
necrosis
in all cases
observed in pocket depth or attachment levels (Chindia &
Triangulaire photographed perpendiculy to the interproximal area: time of their removal
and no (Fig. 8b). Further
severe complications such as healing in these
papilla necrosis Valderhaug 1995). In another study, despite microsurg-
patients was uneventful (Fig. 8c). All other patients dis- ical techniques, the mobilization of the papilla resulted in
Dents postérieurs © 2002 Blackwell Science Ltd
played rapid healing.
International Endodontic Journal, 35, 453 –460, 2002 457
considerable loss of height after 3–5 days (Zimmerman
Rectangulaire © 2002 Blackwell Science Ltd
The photographs did Etiologie,
not reveal Diagnostic
any noticeable&open-
International Endodontic Journal, 35, 453 –460, 2002
Optionsetde
457
traitement
al. 2001). Besides aesthetic disadvantages, this may
Dents Antérieures ing of the space between Styles de lambeaux
the papilla and contact gingival
area as create biological and phonetic problems, as well as food
Avec biotype favorable a result of the loss of papilla height at any observation impaction. The height of the papilla depends on the dis-
Accès osseux, curettage & biopsie
Papille 5mm ou moins time. The mean difference between a reference point and tance between the contact point and crestal bone. In a
the most coronal pointHémostase
of the papilla comparing the pre- healthy periodontium without any attachment loss, the
Submarginal Gestion
operative and the one-month de l'extrémité
postoperative situation radiculaire
was papilla fills the entire interproximal space between two
0.05 ± 0.39 mm. None of the patients exhibited probing teeth in almost all instances (Tarnow et al. 1992). In
Dents avec 2mm de gencive attachée et sans exposition de gencive lors d’un sourire Résection radiculaire
depths greater than 3 mm at one month. The visual periodontally healthy sites, particularly when subgingi-
Ponts Préparation rétrograde
observation of the incisions at this recall demonstrated vally placed crown margins are present, recession is a
Papilla base Obturation rétrograde
Pour cas esthétiques complex Régénération parodontale
458 International Endodontic Journal, 35, 453 –460, 2002 © 2002 Blackwell Science Ltd
Sutures
“Mini” flap
Possible mais doit être guidé Soins Post-op
71 72
Avantage Endo PM - May 15, 2019Vous pouvez aussi lire