DEPRESCRIBING IN THE ELDERLY DÉPRESCRIPTION CHEZ LES AÎNÉS
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous

DEPRESCRIBING IN THE ELDERLY DÉPRESCRIPTION CHEZ LES AÎNÉS

DISCLOSURES DIVULGATIONS I have no potential conflicts of interest Je n’entretiens aucun conflit d’intérêts potentiel. Images are from Microsoft Stock Images Les images proviennent de Microsoft Stock Images.

Vous avez récemment pris
en charge Mme Jones. Son
Ms. Jones is a new patient to médecin de famille a pris
you. Her family physician retired sa retraite l’an dernier, et
last year and one of your un de vos collègues, qui
colleagues who works in the travaille à l’urgence, a
Emergency Department asked if demandé si vous
MRS JONES you would accept Ms. Jones as a l’accepteriez comme
patient as she has been to the patiente, comme elle s’est
ED a number of times in the last retrouvée plusieurs fois à
MME JONES few months, usually with falls l’urgence dans les derniers
and once with acute confusion.. mois, la plupart du temps
This is your second time meeting après avoir fait une chute,
her and you asked her to bring et très confuse…
all her medications with her. C’est la deuxième fois que
The list is as follows: vous la rencontrez, et vous
lui demandez d’apporter la
liste de tous ses
médicaments, que voici :
MEDICATION LIST LISTE DES MÉDICAMENTS 1. Candesartan 4 mg PO Daily 10. Paxil 20 mg PO Daily 2. ASA 81 mg PO Daily 11. Donepezil 10 mg PO Daily 3. HCTZ 25 mg PO Daily 12. Ibuprofen ES QID 4. Metoprolol 100 mg PO BID 13. Vitamin D 1000 IU PO Daily 5. Melatonin 10 mg PO QHS 14. Metformin 1000 mg PO BID 6. Oxybutynin IR 5 mg PO TID 15. Glyburide 2.5 mg PO Daily 7. Atorvastatin 40 mg PO Daily 16. Pantoprazole 80 mg PO Daily 8. Clonazepam 0.5 mg PO QHS 17. Metoclopramide 10 mg BID 9. Calcium 1 tab PO Daily 18. Loperamide daily prn
POLL - HOW DO YOU Comment vous
FEEL WHEN YOU SEE sentez-vous lorsque
THIS MEDICATION LIST? vous voyez cette liste
de médicaments?
1. Excited for the
challenge
2. Defeated 1. Emballé par ce défi
3. Hopeless 2. Vaincu d’avance
3. Désespéré
4. Unflustered
4. Impassible
5. Overwhelmed
5. Dépassé
OBJECTIVES OBJECTIFS
By the end of the session À l’issue de la séance, les
participants will be able to: participants sauront :
1. Recognize problematic 1. reconnaître les
medications commonly médicaments
used in the elderly problématiques
2. Identify safer treatment
couramment utilisés
chez les aînés;
alternatives
2. y substituer des
3. Apply frailty as framework traitements plus sûrs;
to guide prescribing 3. appliquer la fragilité
decisions comme cadre pour
orienter les décisions de
prescription.
SYMPTOMS FRAILTY
THAT LEAD TO AS FRAMEWORK TO
CHALLENGING UNDERSTAND
PRESCRIBING THERAPEUTIC TARGETS
LES SYMPTÔMES LA FRAGILITÉ
QUI RENDENT EN TANT QUE CADRE
DIFFICILE LA POUR
PRESCRIPTION COMPRENDRE LES
CIBLES
THÉRAPEUTIQUES
DEFINITIONS DÉFINITIONS
01 02 03 04
Polypharmacy Inappropriate Prescribing Deprescribing
Prescribing Cascade
Polypharmacie Prescription Cascade de Déprescription
inappropriée prescription
Recueillir des données
Gather DATA: • Quels médicaments le patient
Gather •What drugs is patient currently taking and why? prend-il actuellement et pourquoi?
•Define overall treatment goals/frailty • Définir les objectifs généraux du
Recueillir traitement/la fragilité
STEPS TO
DEPRESCRIBING Décider quel médicament
Decide what medication to reduce réduire et (ou) arrêter
and/or stop Manque d’indications
LES ÉTAPES DE Decide •Lacking indication
•Weigh benefit vs harm for each drug
Peser les avantages et inconvénients de
chaque médicament
Décider •Patient preference Préférence du patient
LA •Prioritize drugs that have the lowest benefit-
harm ratio
Privilégier les médicaments qui
présentent le moins d’inconvénients par
DÉPRESCRIPTION rapport aux avantages qu’ils procurent.
Mettre en œuvre un plan
Implement Implement a plan Suivi étroit
•Close follow-up Surveillance des bienfaits/effets
Mettre en •Monitor for benefit/adverse effect indésirables
œuvre •Liaise with pharmacist Consultation du pharmacien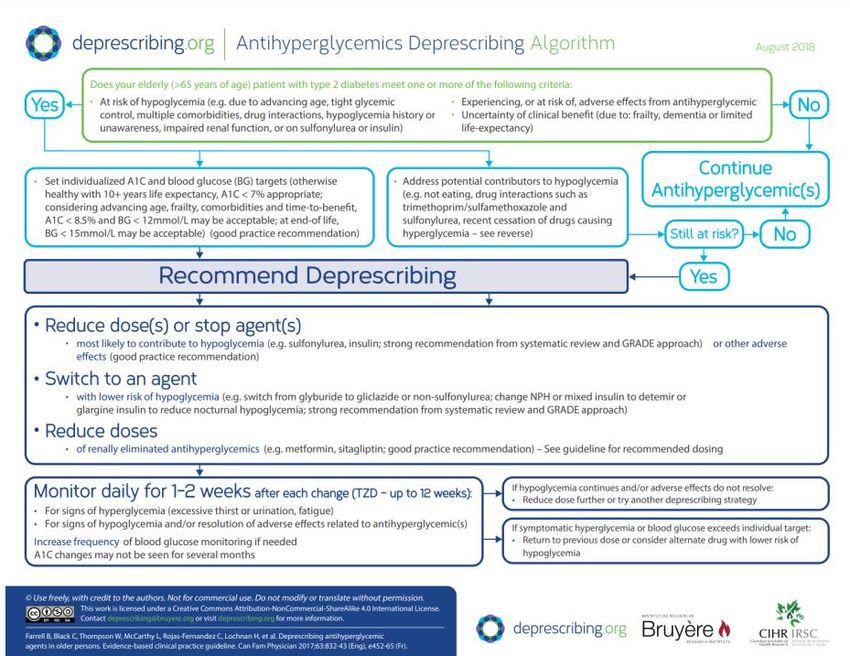
TAKE YOUR TIME
DON’T MAKE TOO MANY
TIPS CHANGES AT ONCE
FOR DEPRESCRIBING AVOID SUBSTITUTIONS
ASK FOR HELP
PRENEZ VOTRE TEMPS
CONSEILS POUR LA N’APPORTEZ PAS TROP
DE CHANGEMENTS EN
DÉPRESCRIPTION MÊME TEMPS
ÉVITEZ LES
SUBSTITUTIONS
DEMANDEZ DE L’AIDEPOLL: WHAT
SYMPTOM DO YOU
FIND MOST
CHALLENGING TO Sleep Sommeil
MANAGE SAFELY
WITH MEDICATIONS Mood Humeur
IN THE ELDERLY?
Pain Douleur
SONDAGE : QUEL
SYMPTÔME Incontinence Incontinence
TROUVEZ-VOUS LE
PLUS DIFFICILE DE
GÉRER SANS
Other Autre
RISQUE CHEZ LES
AÎNÉS?SOMMEIL, DOULEUR, SLEEP, PAIN, MOOD, HUMEUR, INCONTINENCE URINARY INCONTINENCE URINAIRE WHAT TO PRESCRIBE, WHAT TO DEPRESCRIBE QUOI PRESCRIRE, QUOI DÉPRESCRIRE
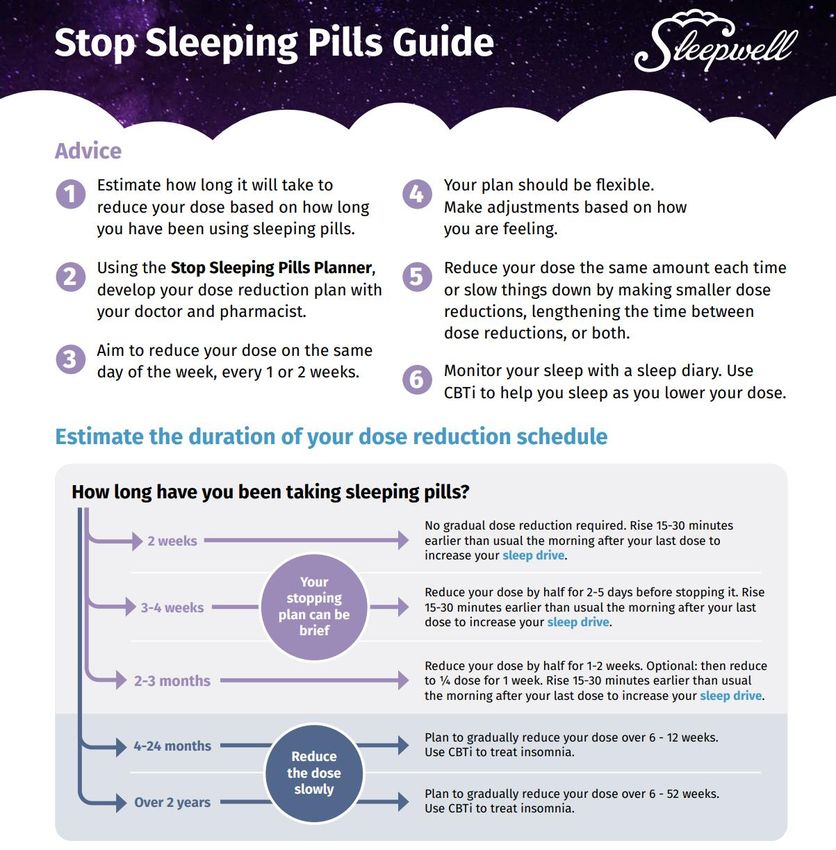
CE N’EST PAS UN RÊVE : DORMEZ BIEN SANS SOMNIFÈRES.
MEDICATION FOR SLEEP THAT MAY BE BENEFICIAL AND SAFER
MÉDICAMENTS POUR LES TROUBLES DU SOMMEIL QUI POURRAIENT
S’AVÉRER BÉNÉFIQUES ET PLUS SÛRS
MELATONIN / MÉLATONINE
Recommended dose: 0.5mg - 3mg 1 hour before Dose recommandée : de 0,5 mg à 3 mg, 1 h
sleep avant le coucher
PROS: CONS:
May be safer May be ineffective
Fewer/milder adverse effects OTC so not covered by pharmacare
May help if limited exposure to sunlight Potential adverse effects: headaches, nausea, dizziness, low blood
pressure, ?fractures
AVANTAGES :
Pourrait être plus sûr
INCONVÉNIENTS:
Moins d’effets indésirables/effets moins importants
Pourrait être inefficace
Pourrait s’avérer efficace en cas d’exposition limitée au soleil
En vente libre; n’est donc pas couvert par l’assurance-maladie
Effets indésirables potentiels : maux de tête, nausée, étourdissements,
hypotension artérielle, fracturesMEDICATION FOR SLEEP THAT MAY BE INDICATED
MÉDICAMENTS POUR LES TROUBLES DU SOMMEIL QUI POURRAIENT ÊTRE
INDIQUÉS
MIRTAZAPINE
ONLY has a role as sleep aid if concurrent En cas d’anxiété ou de dépression concomitante
anxiety or depression! UNIQUEMENT!
CONS:
PROS:
Increases risk of falls
If concurrent depression/anxiety may have beneficial side effect
of improving sleep Can be overly sedating
Antihistamine effect, Dry mouth
INCONVÉNIENTS :
AVANTAGE : Accroît le risque de chute
Pourrait améliorer le sommeil chez un sujet dépressif/anxieux Son effet sédatif peut être trop puissant
Effet antihistaminique, bouche sèche
Sleep benefit is at the low dose range 7.5mg to 15mg
Aide-sommeil à faible dose, de l’ordre de 7,5 mg à 15 mgMEDICATIONS USED FOR SLEEP THAT MAY CAUSE MORE HARM THAN GOOD
MÉDICAMENTS POUR LES TROUBLES DU SOMMEIL QUI POURRAIENT FAIRE
DAVANTAGE DE TORT QUE DE BIEN
All are high-risk medications
Tous sont des médicaments à haut risque
•Trazodone
•TCAs
•Z Drugs
•BenzodiazepinesPAIN DOULEUR
Acétaminophène à heures fixes
Schedule Acetaminophen Anti-inflammatoires non
stéroïdiens (AINS) topiques
Topical NSAIDs
PAIN PEARLS Use opioids if there is a need, Recourir aux opioïdes au besoin;
l’âge à lui seul n’est pas une
don’t use age alone as a raison pour ne pas traiter
reason not to treat pain adéquatement la douleur
RECOMMANDATIONS adequately
CONCERNANT LA Codeine (non responders)
Codéine (non-répondants)
DOULEUR Hydromorphone better option
L’hydromorphone constitue une
meilleure option en cas
for renal impairment d’insuffisance rénale.
Concurrent constipation with
Constipation due aux opioïdes –
opioids – Use PEG utiliser le polyéthylène glycol
(PEG)“
OPIOID THERAPY FOR ELDERLY LE TRAITEMENT PAR OPIOÏDES
PATIENTS CAN BE SAFE AND CHEZ LES PATIENTS ÂGÉS PEUT
EFFECTIVE (GRADE B) WITH ÊTRE SÉCURITAIRE ET EFFICACE
APPROPRIATE PRECAUTIONS , (GRADE B) À CONDITION DE
INCLUDING LOWER STARTING PRENDRE LES PRÉCAUTIONS
DOSES, SLOWER TITRATION, APPROPRIÉES, DONT DES DOSES
LONGER DOSING INTERVAL, INITIALES INFÉRIEURES, UN
MORE FREQUENT TITRAGE PLUS LENT, UN
MONITORING, AND TAPERING INTERVALLE PLUS LONG ENTRE LES
OF BENZODIAZEPINES (GRADE
C).
RECOMMENDATION 17
DOSES, UNE SURVEILLANCE PLUS
FRÉQUENTE ET LA RÉDUCTION
PROGRESSIVE DES
BENZODIAZÉPINES (GRADE C).
”
Recommandation 17 [traduction]
2010 Canadian Guideline for Safe and Effective Use of Opioids for Chronic Non-Cancer Pain.
2010 Lignes directrices canadiennes sur l’utilisation sécuritaire et efficace des opioïdes pour la douleur chronique non
cancéreuse
Kahan, Meldon, Lynn Wilson, Angela Mailis-Gagnon, and Anita Srivastava. "Canadian Guideline for Safe and Effective Use of Opioids for Chronic Noncancer Pain Clinical Summary for Family
Physicians. Part 2: Special Populations." Canadian Family Physician 57.11 (2011): 1269-276. Web.MOOD HUMEUR
MOOD / HUMEUR
PREFERRED ANTI-DEPRESSANTS AND ANXIOLYTICS
ANTIDÉPRESSEURS ET ANXIOLYTIQUE À PRIVILÉGIER
Sertraline
•Monitor sodium
•Surveiller le sodium
RISKS: RISQUES
Citalopram or Escitalopram Increase Falls Risque accru de chutes
•Monitor QT
•Surveiller l’intervalle QT
Confusion Confusion
Bupropion QT Prolongation Allongement
•May increase anxiety and insomnia de l'intervalle QT
•Peut accroître l’anxiété et l’insomnie
Hyponatremia Hyponatrémie
Mirtazapine
•Sedating but this can be a desirable adverse effect
Urinary Incontinence Incontinence urinaire
•Effet sédatif, mais ce peut être un effet désirableDEPRESCRIBING MOOD MEDS
DÉPRESCRIPTION DES MÉDICAMENTS POUR L’HUMEUR
Why are you deprescribing?
No longer needed?
Ineffective?
Right dose?
Right diagnosis?
Unsafe choice?
Cross taper
Pourquoi les déprescrivez-vous?
Plus nécessaires?
Inefficaces?
Bonne posologie?
Bon diagnostic?
Choix dangereux?
Remplacement progressif par un médicament
de substitution https://www2.gov.bc.ca/assets/gov/health/practitioner-pro/bc-guidelines/depress_appd.pdfBENZODIAZEPINES
BENZODIAZÉPINES
Lorazepam or clonazepam
“best of the bad”
VERY SLOW TAPER
Deprescribing.org
Lorazépam ou clonazépam – les
« moins pires »
DIMINUTION TRÈS PROGRESSIVE
deprescribing.orgURINARY INCONTINENCE
IS RX REALLY HELPING? Strong anticholinergic effect
Antimuscarinic agents: cognitive impairment, falls
Alpha Blocker: orthostatic hypotension
INCONTINENCE
URINAIRE : LES Fort effet anticholinergique
MÉDICAMENTS SUR Agents antimuscariniques : dégradation des facultés
ORDONNANCE cognitives, chutes
CHANGENT-ILS Alphabloquants : hypotension orthostatique
VRAIMENT QUELQUE
CHOSE?NAUSEA
NAUSÉE
Try instead: Essayer plutôt :
High Risk due to Ginger ▪ Gingembre
anticholinergic effect: Small Meals
▪ Repas légers
▪ S’agit-il d’un effet
Risque élevé étant donné Is it a side effect from secondaire d’un
autre
l’effet anticholinergique another med? médicament?
Get to root cause ▪ Trouver la cause
•Diphenhydramine profonde
PPI ▪ IPP
•Metoclopramide
•H2 blockersHIGH RISK CARDIAC MEDS MÉDICAMENTS POUR LE COEUR
À HAUT RISQUE
Frequent offenders / Souvent mis en cause Considerations / Considérations
Digoxin – monitoring + toxicity Patient centered Prise de décisions
decision making centrée sur le patient
Beta Blockers – orthostatic hypotension,
Goals of therapy Objectifs du
fatigue
traitement
Burden of
Calcium Chanel Blockers – prescribing Fardeau de la
monitoring
cascade surveillance
Renal function
Diuretics – orthostatic hypotension, urinary Fonction rénale
incontinence, feeling “dry”, electrolytes and Orthostatic Hypotension
creatinine need monitoring hypotension orthostatiqueFRAILTY FRAGILITÉ HOW DOES FRAILTY FIT INTO PRESCRIBING AND DEPRESCRIBING SA PLACE DANS LA PRESCRIPTION ET LA DÉPRESCRIPTION
WHAT IS FRAILTY QU’EST-CE QUE LA FRAGILITÉ?
“Frailty is a progressive physiological decline in multiple organ systems marked by loss of
function, loss of physiological reserve and increased vulnerability to disease and death. Frail
older adults are vulnerable to poor health outcomes including an increased risk of disability,
social isolation and institutionalisation.”
« La fragilité est un déclin physiologique progressif de multiples systèmes d’organes
caractérisé par la perte de fonction, la perte de réserve physiologique et une plus grande
vulnérabilité à la maladie et au décès. Les personnes âgées fragiles s’exposent à de piètres
résultats en matière de santé, courant notamment un risque accru d’invalidité, d’isolement
social et institutionnalisation. » [traduction]
Moorhouse, P., and K. Rockwood. "Frailty and Its Quantitative Clinical Evaluation." The
Journal of the Royal College of Physicians of Edinburgh 42.4 (2012): 333-40. Web.POLL: WHO ROUTINELY ADJUSTS SONDAGE : QUI AJUSTE
THEIR PRESCRIBING IN PATIENTS RÉGULIÈREMENT SES
WHO ARE MODERATELY OR PRESCRIPTIONS CHEZ LES
SEVERELY FRAIL FOR THE PATIENTS MODÉRÉMENT OU
FOLLOWING TRÈS FRAGILES EN CE QUI
CONCERNE :
1. Statins 1. Statines
2. ASA 2. AAS
3. Hypertensives 3. Médicaments contre l’hypertension
4. Bisphosphonates 4. Bisphosphonates
5. Diabetic medications 5. Médicaments pour diabétiquesSeverely frail elderly patients: No indication
Patients âgés très fragiles : absence d’indication
FRAILTY AND
STATINS
Over 85 years of age: Likely limited benefit for risks
Patients de 85 ans et plus : les avantages sont
FRAGILITÉ ET probablement limités par rapport aux risques
STATINES
Over 75 years of age: Value of statins is controversial
Patients de 75 ans et plus : la valeur des statines est
controversée
https://www.choosingwisely.org/clinician-lists/amda-lipid-lowering-medications
Ruscica, M., C. Macchi, C. Pavanello, A. Corsini, A. Sahebkar, and C.R Sirtori. "Appropriateness of Statin
Prescription in the Elderly." European Journal of Internal Medicine 50 (2018): 33-40. Web.HTN AND FRAILTY
Target SBP: 140 and 160
Target: No orthostatic drop to less than 140
Initiate: if SBP over 160
Severe Frailty:
Target SBP: 160 to 190
HYPERTENSION ET
FRAGILITÉ
Tension artérielle systolique cible : 140 et 160
Objectif : pas de chute orthostatique à moins
de 140 Promotion d’une tension artérielle plus élevée chez les personnes
Débuter : si la tension artérielle systolique âgées fragiles : directive consensuelle du Canada
dépasse 160
Grande fragilité :
Mallery LH, Allen M, Fleming I, Kelly K, Bowles S, Duncan J, Moorhouse P.
Tension artérielle systolique cible : de 160 à Promoting higher blood pressure targets for frail older adults: a consensus guideline from
190 Canada. Cleve Clin J Med. 2014 Jul;81(7):427-37.DIABETES AND DIABÈTE ET
FRAILTY FRAGILITÉ
1. Maintain HbA1c at or above 8% 1. Maintenir l'HbA1c à 8 % ou plus
rather than below a specific level plutôt qu’en dessous d’un certain
niveau
2. Simplify treatment by 2. Simplifier le traitement par
administering basal insulin alone l’administration d’insuline basale
seulement
3. Use NPH insulin instead of long-
3. Utiliser de l’ insuline NPH au lieu des
acting insulin analogues, analogues de l'insuline à action
prolongéeDEPRESSION AND
FRAILTY
“Second-generation antidepressants
have uncertain benefit for older adults
with depression and cause more
adverse events compared to placebo.
Until further research clarifies benefit,
careful consideration of
antidepressant prescribing with frailty
is warranted.”
DÉPRESSION ET FRAGILITÉ
« Les avantages des antidépresseurs
de seconde génération chez les aînés
atteints de dépression sont incertains,
et ils causent davantage d’effets
indésirables que les placebos. Jusqu’à
ce que des recherches plus poussées
permettent d’établir clairement ces
avantages, il convient de les prescrire Examen systématique et méta-analyse d’antidépresseurs de
avec circonspection chez les patients seconde generation pour le traitement de la depression chez
fragiles. »
les aînés : avantages discutables et considérations liées à la
fragilitéPITFALLS AND CHALLENGES OF DEPRESCRIBING LES PIÈGES ET LES DÉFIS DE LA DÉPRESCRIPTION
WHAT MAKES POURQUOI EST-IL FACILE
PRESCRIBING EASY DE PRESCRIRE ET
AND DEPRESCRIBING DIFFICILE DE
HARD? DÉPRESCRIRE?
Psychological: Psychologiquement :
We want to “do” something Nous voulons « faire » quelque
Act of “taking away” may chose.
be seen as lack of Le fait de « retirer » quelque chose
attention pourrait être perçu comme un
manque d’attention.
Clinical Guidelines Lignes directrices cliniques
When started by others Lorsque les prescriptions émanent
de quelqu’un d’autre
Withdrawal side effects
Complex decisions Effets secondaires liés au sevrage
Décisions complexes
Think of deprescribing as a procedure
Envisagez la déprescription comme une procédure.PRESCRIBING PITFALLS LES PIÈGES DE LA DÉPRESCRIPTION
Not considering
Prescribing Cascade
Frailty
Cascade de
Ne pas tenir compte
prescription
de la fragilitéDEPRESCRIBING PITFALLS LES PIÈGES DE LA DÉPRESCRIPTION Going too fast Aller trop vite Substitution Effect Effet de substitution Trying to do it Alone Essayer de procéder seul
RESOURCES RESSOURCES
BLOOMPROGRAM.CA
RESOURCES RESSOURCES https://deprescribing.org http://medstopper.com https://choosingwiselycanada.org/toolkit/less-sedatives-for- your-older-relatives https://www.deprescribingnetwork.ca Polypharmacy and Deprescribing module: https://www.bruyere.org/en/polypharmacy-deprescribing
TAKE HOME POINTS CONCLUSIONS
Frailty will help focus
Patient centered
decisions
process Take your time
Tenez compte de la
Processus centré sur Prenez votre temps
fragilité dans la prise
le patient
de décisions
Don’t make too many
Ask for
changes at once Avoid substitutions
help/Collaborate
N’apportez pas trop Évitez les
Demandez de
de changements à la substitutions
l’aide/collaborez
foisREFERENCES / RÉFÉRENCES
Anderson TS, Steinman MA. Antihypertensive Prescribing Cascades as High-Priority Targets for Deprescribing. JAMA Intern Med. 2020;180(5):651–652. doi:10.1001/jamainternmed.2019.7082
Anghel, Lucretia, Liliana Baroiu, Corina Risca et al "Benefits and Adverse Events of Melatonin Use in the Elderly." Experimental and Therapeutic Medicine 23.3 (2022): Experimental and Therapeutic Medicine, 2022-03-01, Vol.23 (3). Web.
Best Practice Journal. A practical guide to stopping medicines in older people. Best Pract J 2010;27:10-23.
Djatche, L., S. Lee, D. Singer, S. E Hegarty, M. Lombardi, and V. Maio. "How Confident Are Physicians in Deprescribing for the Elderly and What Barriers Prevent Deprescribing?" Journal of Clinical Pharmacy and Therapeutics 43.4 (2018): 550-55.
Web.
Farrell, Barbara, Cody Black, Wade Thompson, Lisa McCarthy, Carlos Rojas-Fernandez, Heather Lochnan, Salima Shamji, Ross Upshur, Manon Bouchard, and Vivian Welch. "Deprescribing Antihyperglycemic Agents in Older Persons: Evidence-
based Clinical Practice Guideline." Canadian Family Physician 63.11 (2017): 832-43. Web.
Frank, Christopher, and Erica Weir. "Deprescribing for Older Patients." Canadian Medical Association Journal (CMAJ) 186.18 (2014): 1369-376. Web.
Frisher M, Gibbons N, Bashford J, Chapman S, Weich S. Melatonin, hypnotics and their association with fracture: a matched cohort study. Age Ageing. 2016;45(6):801–6
Kahan, Meldon, Angela Mailis-Gagnon, Lynn Wilson, and Anita Srivastava. "Canadian Guideline for Safe and Effective Use of Opioids for Chronic Noncancer Pain Clinical Summary for Family Physicians. Part 1: General Population." Canadian Family
Physician 57.11 (2011): 1257-266. Web.
Kahan, Meldon, Lynn Wilson, Angela Mailis-Gagnon, and Anita Srivastava. "Canadian Guideline for Safe and Effective Use of Opioids for Chronic Noncancer Pain Clinical Summary for Family Physicians. Part 2: Special Populations." Canadian,
Robert L, Joseph Hanlon, and Emily R Hajjar. "Clinical Consequences of Polypharmacy in Elderly." Expert Opinion on Drug Safety 13.1 (2014): 57-65. Web.
MaFamily Physician 57.11 (2011): 1269-276. Web.,
Mallery LH, Moorhouse P, McLean Veysey P, Allen M, Fleming I. Severely frail elderly patients do not need lipid-lowering drugs. Cleve Clin J Med. 2017 Feb;84(2):131-142. doi: 10.3949/ccjm.84a.15114. PMID: 28198686.
Maherllery LH, Allen M, Fleming I, Kelly K, Bowles S, Duncan J, Moorhouse P. Promoting higher blood pressure targets for frail older adults: a consensus guideline from Canada. Cleve Clin J Med. 2014 Jul;81(7):427-37. doi: 10.3949/ccjm.81a.13110. PMID:
24987044.
Mallery, Laurie Herzig, MD, FRCPC, Ransom, Tom, MD, FRCPC, Steeves, Brian, MD, Cook, Brenda, MAdEd, PDt, CDE, Dunbar, Peggy, MEd, PDt, CDE, and Moorhouse, Paige, MD, MPH, FRCPC. "Evidence-Informed Guidelines for Treating Frail Older
Adults With Type 2 Diabetes: From the Diabetes Care Program of Nova Scotia (DCPNS) and the Palliative and Therapeutic Harmonization (PATH) Program." Journal of the American Medical Directors Association 14.11 (2013): 801-08. Web.
Matthew E, Edie Espejo, Bocheng Jing, W John Boscardin, Andrew R Zullo, Kristine Yaffe, Kenneth S Boockvar, and Michael A Steinman. "Attitudes toward Deprescribing among Older Adults with Dementia in the United States." Journal of the
American Geriatrics Society (JAGS) (2022): Journal of the American Geriatrics Society (JAGS), 2022-03-10. Web.
Rossi, Pier Riccardo, Sarah E. Hegarty, Vittorio Maio, Marco Lombardi, Andrea Pizzini, Aldo Mozzone, Marzio Uberti, and Simonetta Miozzo. "General Practitioner Attitudes and Confidence to Deprescribing for Elderly Patients." Geriatric Care (Pavia)
6.1 (2020): Geriatric Care (Pavia), 2020-03-12, Vol.6 (1). Web
Savage RD, Visentin JD, Bronskill SE, et al. Evaluation of a Common Prescribing Cascade of Calcium Channel Blockers and Diuretics in Older Adults With Hypertension. JAMA Intern Med. 2020;180(5):643–651.
doi:10.1001/jamainternmed.2019.7087
Scott, Ian A, Sarah N Hilmer, Emily Reeve, Kathleen Potter, David Le Couteur, Deborah Rigby, Danijela Gnjidic, Christopher B Del Mar, Elizabeth E Roughead, Amy Page, Jesse Jansen, and Jennifer H Martin. "Reducing Inappropriate Polypharmacy:
The Process of Deprescribing." JAMA Internal Medicine 175.5 (2015): 827-34. Web.
Should Melatonin Be Used as a Sleeping Aid for Elderly People?. Can J Hosp Pharm. 2019;72(4):327-329.WEBSITES AND PODCASTS SITES WEB ET BALADOS Podcasts: GeriPal: Polypharmacy and Deprescribing. July 16, 2021 The Curbsiders Internal Medicine Podcast #56 and #57 Polypharmacy and Deprescribing. September 11, 2017 Websites: https://deprescribing.org http://medstopper.com https://choosingwiselycanada.org/toolkit/less-sedatives-for-your-older-relatives https://www.deprescribingnetwork.ca https://pathclinic.ca/education/clinical-practice-guidelines Polypharmacy and Deprescribing module: https://www.bruyere.org/en/polypharmacy-deprescribing START/STOPP Toolkit: https://www.cgakit.com/m-2-stopp-start BEERS Criteria: https://www.guidelinecentral.com/guideline/340784/
Vous pouvez aussi lire

















































