Echographie ciblée en médecine familiale - 11 mai 2017 Anne-Patricia Prévost Payge Ouellet Rodrigue GMF-U St-Hubert ...
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous
Echographie ciblée
en médecine familiale
11 mai 2017
Anne-Patricia Prévost
Payge Ouellet Rodrigue
GMF-U St-Hubert
anne_pat@videotron.ca
@apprevost
Déclaration de conflit d’intérêt • Aucun
LES OBJECTIFS • Démontrer l’utilisation de l’échographie ciblée en médecine de famille • Démontrer son utilité par des données probantes • Fournir une stratégie d’implantation aux CUMF
5. Steinmetz et al, 2016 6. Hall et al, 2015 7. Bahner et al 2014

LITTERATURE 3. Steinmetz et al 2016
LISTE DES EXAMENS CIBLÉS EN
MEDECINE FAMILIALE
Société canadienne d’échographie ciblée (SCEDU)
•Les évaluations échographies de bases incluent:
•Dépistage de AAA
•Confirmation de la grossesse intra-utérine, de l’activité foetale et de l’âge de
la grossesse
•Confirmation de la présence d’ascite chez un patient avec une distension
abdominale
•Évaluer la présence d’un épanchement péricardique chez un patient avec de
la dyspnée
LISTE DES EXAMENS CIBLÉS EN
MEDECINE FAMILIALE
•Autres exemples:
•Présence d’épanchement pleural
•Présence d’une pneumonie
•Présence de surcharge
•Présence de cholélithiases ou cholecystite
•Présence d’une hydronéphrose
•Condition musculosquelettique
•Conditions obstétricales au 3ème trimestre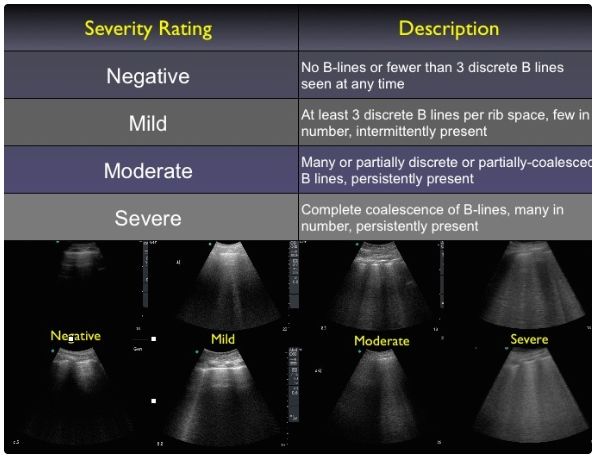


AAA
ECHO
Sensibilité 88% à 100%
Spécificité 98% à 100%
VPP 97 %
VPN 99 %
Temps moyen pour
un examen 3 1\2 minutes
Formation suggérée 50 échographies
Exactitude 98 %
8. Bois et al 2012
9. Vourvouri et al 2001
10. Wilmink 2002
11. Lindholt 1999Dépistage de l’AAA
ECHO
Sensibilité 88% à 100% E/O
Spécificité 98% à 100% Sensibilité de
29% à 76%
VPP 97 %
VPN 99 %
Temps moyen pour
un examen 3 1\2 minutes
Formation suggérée 50 échographies
Exactitude 98 %OBSTÉTRIQUE
ECHO
Sensibilité 97 %
Spécificité 98 %
Formation 5 jours (théorie et pratique)
nécessaire 3 demi-journée en salle
d’échographie
# total d’examen 15 à 50
requis
Exactitude 86 à 96 %
12. Keith et al 2001 16. Bofill et al 1998
13. Ornstein et al 1990 17. Rodney et al 1990
14. Hahn et al 1988 18. Fescina et al 1980
15. Stein et al 2008 19. Walter et al 1988Épanchement péricardique
ECHO
Sensibilité 96 %
Spécificité 98 %
Exactitude 86 %
Formation 8-10 heures
nécessaire
24. Labovitz et al 2010
25. Mandavia 2002
26. Goodkin et al 2001GLISSEMENT PLEURAL
PNEUMOTHORAX
ECHO
Sensibilité 95% à 100%
Spécificité 94% à 96%
30. Lanctôt 2011
31. Blaivas 2005
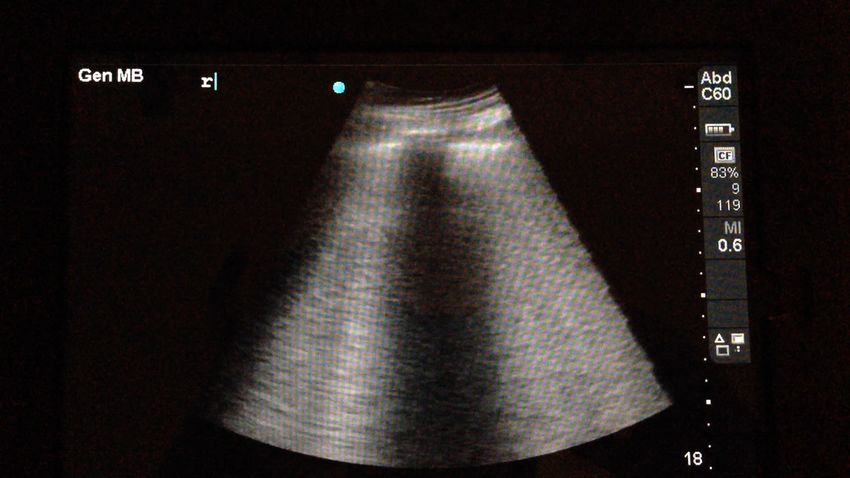
32. Lichtenstein 2004SYNDROME INTERSTITIEL
SYNDROME INTERSTITIEL
ECHO
Sensibilité 85% à 100%
Spécificité 89% à 97%
VPP
86% à 99%
33. Liechtenstein et all 2007
34. Volpicelli et all 2006
35. Zanobetti et all 2011ÉPANCHEMENT PLEURAL
ECHO RXP
Sensibilité Sensibilité
97.5% 92.5%
Spécificité Spécificité
99,7% 99,7%ÉPANCHEMENT PLEURAL
ECHO
Écho: 20 cc
Sensibilité
RXP: 50-100 cc
Spécificité
RXP couché: 175 cc
Cout-Efficacité
Plus rapide que la
radiographie
Plus précis que la
radiographie
36. Sisley et al 1998
37. Vignon et al 2005PNEUMONIE
ECHO
Sensibilité 90 %
Spécificité 98 %
Cout-Efficacité
Plus rapide que la
radiographie
Plus précis que la
radiographie
38. Liechtenstein et al 2004PNEUMONIE ECHO RXP Sensibilité Sensibilité 95% 85% Spécificité Spécificité 99% 67%
PRATICO-PRATIQUE EN RÉSIDENCE • Formation cours d’urgence (Écho ciblée 1 et 2) • Application à l’UMF • Suivi de grossesse • SRV • Chirurgie mineure • Clinique MSK • Pratique à ICM / urgence / hospit
EN COURS À U DE M
Comité sur l’échographie au programme d’études médicales de 1er cycle
• Initier les étudiants à l’usage de l’échographie
• Intégration longitudinale de la 1ère à la 4ème année
• Cours magistral et formations sur simulateur:
• Principes de base
• Connaître artéfacts
• Connaître les limites de l’échographie
• Localiser les organes
• Évaluation cibléeEN COURS À U DE M
Comité sur l’échographie en médecine familiale
• Examens ciblés choisis (AAA, grossesse, rétention urinaire, épanchement
péricardique et pleural, liquide libre, tissus mous)
• Plan de formation des médecins de famille en UMF
• Identifier les leaders d’écho (2 PI par UMF)
• Formation professorale en septembre 2017
• Formation pratique en 2018
• Plan de formation des résidents pour les R1
• Susciter l’intérêt
• Initiation à l’échographie
• Développer des compétences et connaître ses limitesFORMATION ACTUELLE • SCEDU (société canadienne de l’échographie ciblée) • EDU • Praticien indépendant • MUSE (McGill) • Congrès mondial sur l’enseignement de l’échographie ciblée (WCUME 2017)
COÛT • 1000-2000$ / journée de formation • Appareil entre 10 000 et 40 000$
LES BENEFICES • Non-invasif • Réassurant pour les patients • Réduction de tests inutiles • Réduction d’admission aux urgences • Réduction des visites à l’hôpital • Favorise le développement d’habiletés techniques • Augmente la satisfaction professionnelle
LE FUTUR
• Programmes balisés
• Normes canadiennes
• Maintien des compétences
• Politiques de standardisation :règlement du
CMQ à venirQUESTIONS?
RÉFÉRENCES 1. Kobal et al. Comparaison of effectiveness of hand-carried ultrasound to bedside cardiovascular physical examination. Am J Cardiol 2005; 96: 1002-6 2. Liebo et al. Is pocket mobile echocardiography the next-generation sthetoscope? A cross-sectional comparaison of rapidly acquired images with standard transthoracic echocardiography. Ann Intern Med 2011; 155: 33-8 3. Steinmetz et al. The benefit of doing ultrasound examen in your office. J of Fam Prac 2016 65, 8; 517-523 4. Deshpande et al. Utility of ultrasound in the ICU. Curt Opim Anesthesiol 2014 ; 27: 123-132 5. Steinmetz et al. Bedside ultrasound education in Canadian medical schools: a national survey. Can Med Educ J 2016; 7:e78-e86 6. Hall et al. Point of Care Ultrasound in Family Medecine Residency Program: A CERA Study. Fam Med 2015; 47: 706-711 7. Banner al. The State of Ultrasound Education in U.S. Medical Schools : Results of a National Survey. Academic Medicine 2014; 89, 12 8. Blois et al. Office-based ultrasound screening for abdominal aortic aneurysm. Can Fam Physician 2012; 58: e172-178 9. Vourvouri et al. Abdominal aortic aneurysm screening using a hand-held ultrasound device. « A pilot study ». Our J Vasc Endovasc Surg 2001; 22: 352-354 10.Wilmink et al. Accuracy of serial screening for abdominal aortic aneurysms by ultrasound. J Med Screen 2002; 9: 125-127 11. Lindholt et al. The validité of ultrasonographic scanning as sceening method for abdominal aortic aneurysm. Eur J Vasc Endovasc surg 1999; 17: 472-475 12. Keith et al. Fetal biometry: a comparison of family physicians ans radiologistes. Fam Med 2001; 33:111-114 13. Ornstein et al. Obstetric ultrasound by family physicians. Adequacy as assessed by pregnancy outcome. J Fam Pract 1990; 30:403-408 14. Hahn et al Cost-effectiveness of office obstetrical ultrasound in family practice: preliminary considerations. J Am Board Fam Pract 1988; 1: 33-38 15. Stein et al. A two-level ultrasonographic service in a maternity care unit of a rural district hospital in Tanzania. Trop Doct 2008 ; 38: 125-126
RÉFÉRENCES 16. Bofill et al. Obstétric sonography. Who to scan, when to scan, and by whom. Obstet Gynecol Clin North Am 1998; 25: 465-478 17. Rodney et al. Family practice obstetric ultrasound in an urban community health center. Birth outcomes and examination accuracy of the initial 227 cases. J Fam Pract 1990; 30: 163-8 18. Fescina et al. Reliability of fetal anthropometry by ultrasound. J Perinat Med 1980; 8; 93-7 19. Walter et al. Ultrasound for the primary care physicianPostgraduate medecine 1988 83;2: 103-107 20. Mjolstad et al. Assessment of left ventricular function by GPs using pocket-size ultrasound. Fam Pract 2012; 29: 534-540 21. Mueller et al. Subjective visual echocardiographic estimante of left ventricular ejection fraction as en alternative to conventional echocardiographic methods; Comparison with contrast angiography. Cardiol Clin 1991; 14: 898-902 22. Manasia et al. Feasibility and potential clinical utility of goal-directed transthoracic echocardiography performed by non cardiologist intensivists using a small hand-carried device in critically ill patients. J Cardiothorac Vasc Anesth 2005; 19: 155-159 23. Moore et al. Determination of left ventricular function by emergency physician echocardiography of hypotensive patients 2002 Acad Emerg Med ;9 : 186-193 24. Labovitz et al. Focused cardiac ultrasound in the mergency setting: a consensus statement of the American Society of echocardiography ans American College of emergency physicians. J Am Soc Echocardiogram 2010; 23 (12) ; 1225-1230 25. Mandavia et al. Bedside echocardiography by emergency physicians, 2001 Ann Emerg Med ; 38 : 337-382 26. Goodman et al. How useful is hand-carried bedside echocardiography in critically ill patients? 2001 J Am Coll Cardiol; 37: 2019-2022 27. Jardin et al. Ultrasonographic examination of the vena cava. Intensive Care Med 2006; 30: 1834-1837 28. Beaulieu. Bedside echocardiography in the assessment of the critically ill. Brit Care Med 2007; 35:5 S235-S249 29. Lucas et al. Diagnostic accuracy of hospitalist performed hand-carried ultrasound echocardiography after a brief staining program, 2009 J Hosp Med ; 4: 340-349 30. Lanctôt et al 2011. Echo-guided life support, an algorithmic approach to undifferentiated shock. 2011 Crit Care Med; 33: 123-129 16. Marik
RÉFÉRENCES 31. Blaivas et al A prospective comparison of supine chest radiography and bedside ultrasound for the diagnostic of traumatic pneumothorax 2005. Acad Emerg; 12: 844-849 32. Liechtenstein et al Relevance of lung ultrasound in the diagnosis of acute lung respiratory failure, the BLUE protocol, 2008 CHEST ; 134: 117-125 33. Liechtenstein et al Ultrasound in the management of thoracic disease 2007 Crt Med Care; 35: SS250-261 34. Volpicelli et al Bedside ultrasound in the assessment of alveolar-interstitial syndrome, 2006 Am J Emerg Med 24; 689-696 35. Zanobetti et al Can chest ultrasonography can replace standard chest radiography for evaluation of acute dyspnea in the ED, 2011 CHEST ; 139: 1140-1147 36. Sisley et al. Rapid detection of traumatic effusion using surgeon performed ultrasound 1998 J Trauma; 44: 291-297 37. Vignon et al. Quantitative assessment of pleural effusion in critically ill patients by means of ultrasonography, 2005 35; 1757-1763 38. Liechtenstein et al Ultrasound disgnosis of alveolar consolidation in the critically ill, 2004 Int Care Med ; 30: 276-281 39. Crisp et al Compression ultrasonography of the lower extremity with portable vascular ultrasonography can accurately detect deep venous thrombosis in the emergency department 2010. Ann Emerg Med ; 56: 601-610 40. Blaivas et al Lower extremity doppler fr deep venous thrombosis - can emergency physicians be accurate and fast? 2000 Acad Emerg Med; 7: 120-126 41. Jolly et al. Color doppler ultrasonography by emergency physicians for the diagnosis of acute deep venous thrombosis. 1997. Acad Emerg Med; 4: 129-132 42. Frazee et al. Negative emergency department compression ultrasound reliability excludes proximal deep vein thrombosis. 1998 Acad Emerg Med ; 5: 406-407 43. Randolf et al. Ultrasound guidance for placement of central venous catheters. 1996 Crit Care Med ; 24 (12): 2053-2058 44. Hahn et al. Diagnostic ultrasound in general practice 1988 Fam Pract ; 5 (2): 129-135 45. Chan et al. Use of clinical ultrasonography in a Autralian Suburban Family Practive: its indications and findings 1999 Hong Kong Pracctitioner; 21: 405-415 46. Siepel et al. The ultrasound-assisted physical examination in the periodic health evaluation of the elderly 2000. J Fam pact 49; 7: 628-632 47. Bornemann et al. Military family physicians’ perceptions of a pocket point-of-care ultrasound device in clinical practice. 2014 Mil Med; 179: 1474-1477
Vous pouvez aussi lire