INFECTIONS CHEZ LE TRANSPLANTÉ D'ORGANE SOLIDE - COURS DESC RÉANIMATION 2019 STÉPHANIE PONS INSERM U976 HÔPITAL SAINT-LOUIS PARIS - CEMIR ...
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous
Infections chez le transplanté
d’organe solide
Cours DESC Réanimation 2019
Stéphanie Pons
INSERM U976
Hôpital Saint-Louis Paris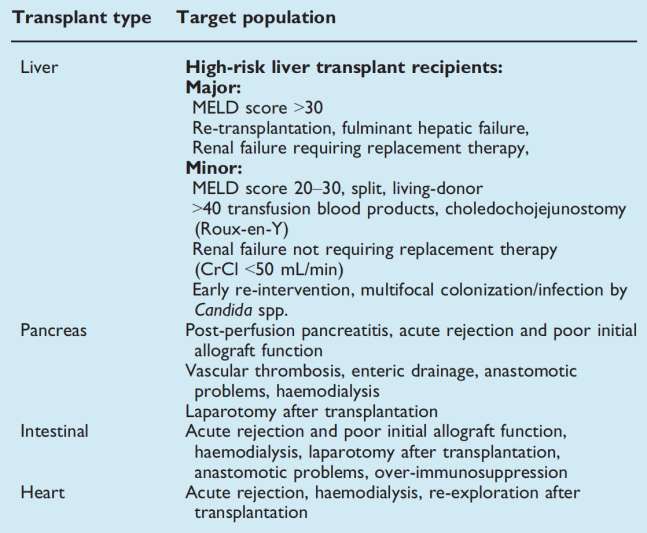
INFECTIONS ET
TRANSPLANTATION D’ORGANE:
GENERALITES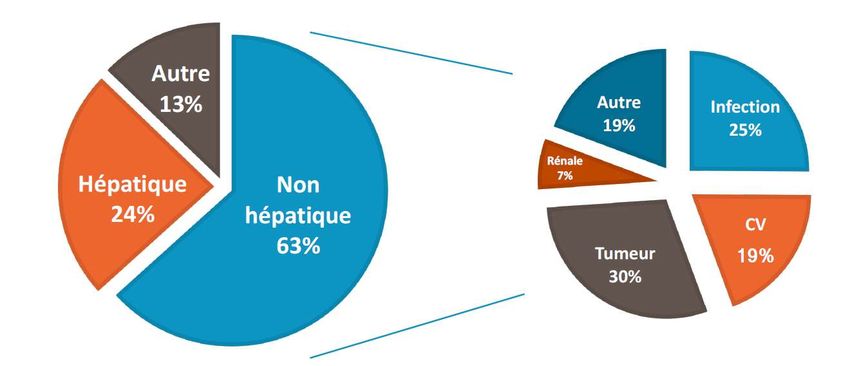
Données de l’agence de la biomédecine
4000
Rein
3000
Foie
Coeur
Poumon
2000
Pancréas
Coeur-poumons
Intestin
1000
0
Rapport de l’Agence de la Biomédecine. 2018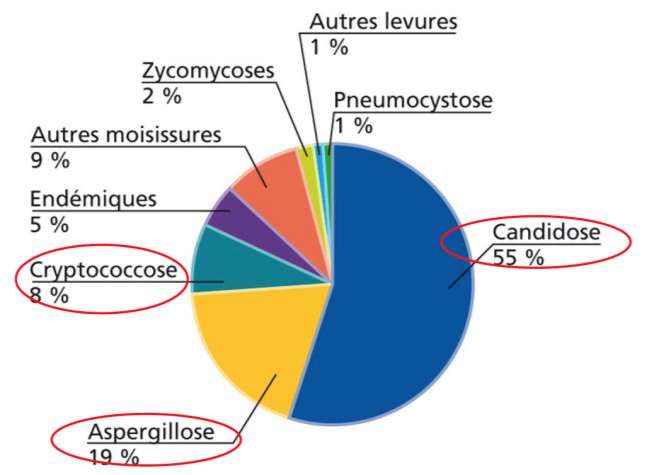
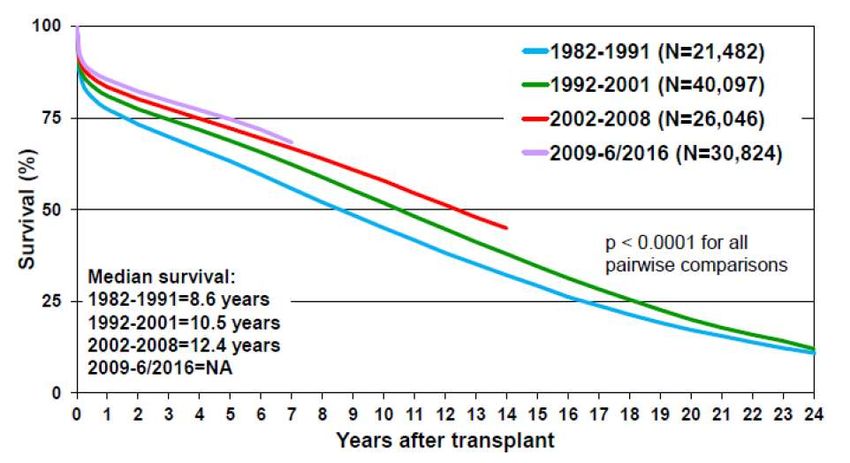
Médiane de survie du TOS
Transplantation cardiaque Transplantation pulmonaire
Khush/Chambers et al. ISHLT. Oct 2018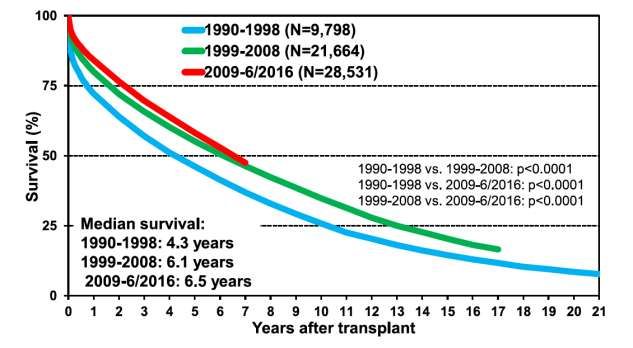
Causes de décès chez le TOS
800 Tx hépatiques
Watt K et al. Am J Transplant. 2010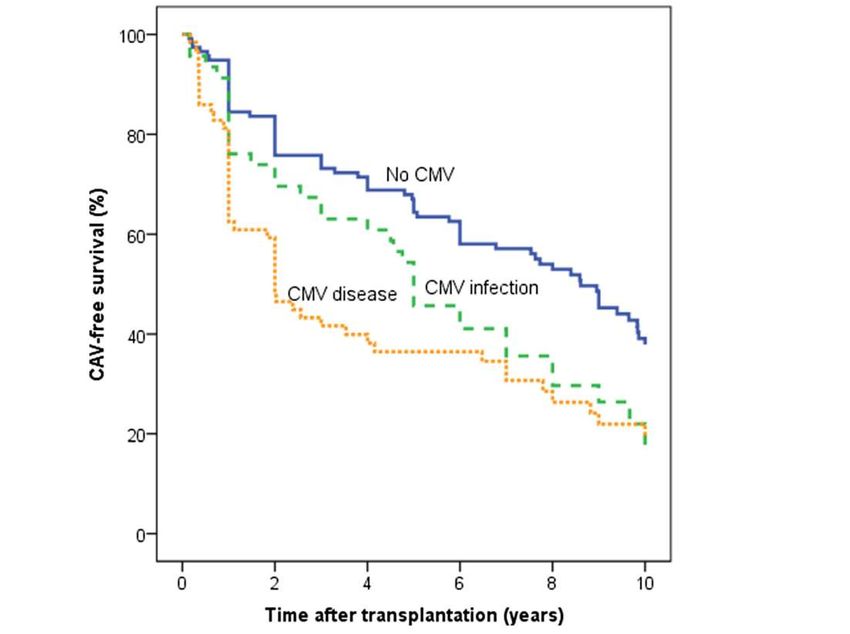
Causes de décès chez le TOS
10.000 Tx rénales au Brésil
De Castro Rodrigues Ferreira et al. J Nephrol. 2017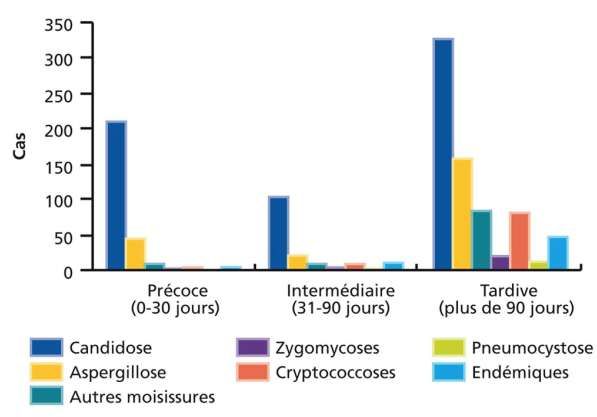
Infection et dysfonction de greffon
897 Tx rénales
184 infections du
tractus urinaire
Bodro et al. Clin Microbio Infect. 2015
Infection et dysfonction de greffon
226 Tx cardiaques
Suivi 10 ans
Johansson et al. BMC Infect Dis. 2015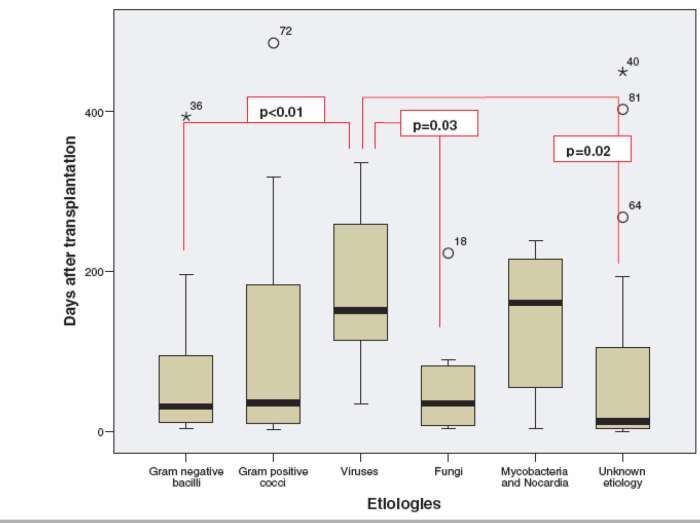
INFECTIONS ET TOS: COMMENT RAISONNER?
Complications infectieuses
Age
Etat nutritionnel
Comorbidités
VIH, VHB, VHC
Rupture des barrières Receveur
muqueuses Prophylaxie
Séroconversion CMV, EBV
PTLD
Type et date Hospitalisations
Complications chir antérieures
Ttt d’induction Greffe Suivi Exposition antibiotiques,
Ttt d’entretien antiviraux, antifongiques
Rejet aigu
Dysfonction chronique
Fishman et al. N Engl J Med. 2007Infections et type/date de transplantation
• Cohorte prospective Espagnole RESITRA: 2702 TOS
Créée en 2003-16 hôpitaux espagnols
• Recueil prospectif de données: Avant, pendant, et après la greffe (suivi 2 ans)
Incidence des infections en fonction du type
et de la période post-transplantation
16
Incidence / 1000 jours
14
de transplantation
12
10
8
6
4
2
0
Rein-Pancréas Poumon Foie Cœur Rein Total
6mois
D’après San Juan et al. Am J Transplant. 2007Délai post-transplantation
Infections Virus Ca dépend…
bactériennes
nosocomiales +++ C. Difficile
Candidémie PCP si pas de
prophylaxie
Infections
dérivées du Infections fongiques
donneur
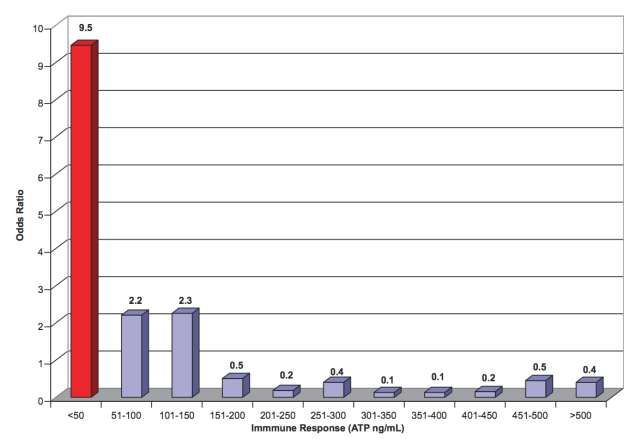
Fishman et al. N Engl J Med. 2007Monitorage de l’immunodépression
175 transplantés pulmonaires. 3 à 4 dosages par patient
Husain et al. Transplantation. 2009Fishman et al. N Engl J Med. 2007
Infections transmises par le greffon • Prévalence faible des infections non attendues (
Infections préalables du receveur
• Histoire personnelle du patient +++:
- Infections connues contrôlées
- Recherche des infections plausibles
• Principaux micro-organismes en cause:
- Infestations parasitaires (Anguillule)
- Mycobactéries
- Mycoses
- Virus latents
- Bactéries (BMR++)
Fishman et al. N Engl J Med. 2007Infections précoces après transplantation • RESITRA: Réseau espagnol pour la recherche sur les infections après transplantation • Caractéristiques des infections après transplantation d’organes: - La majorité des infections précoces sont bactériennes - Elles sont susceptibles d’engager le pronostic vital
Infections précoces: sites
San Juan et al. Am J Transplant. 2007Infections secondaires à la chirurgie
292 patients Tx cardiaques
17 infections de site opératoire
Ramos et al. Transplant Infect Dis. 2008Infection de l’organe transplanté
• 236 patients transplantés pulmonaires entre 2003 et 2007
• Médiane de suivi : 180 jours
• 85 épisodes d’infection pulmonaire chez 61 patients
• 44% des épisodes le premier mois ++
Aguilar-Guisado et al. Am J Transplant. 2007Infection de l’organe transplanté
Aguilar-Guisado et al. Am J Transplant. 2007Infection de l’organe transplanté
Aguilar-Guisado et al. Am J Transplant. 2007Infections précoces: germes
113 transplantés cardiaques entre 2011 et 2015
100
h e a r t t r a n s p la n t r e c ip i e n t s
B e fo r e d a y 8
80 D a y s 8 to 3 0
P e rc e n ta g e o f
D a y s 3 1 to 1 8 0
60
40
20
0
i
a
s
i
a
e
c
g
ri
u
s
a
c
n
te
ir
o
e
o
u
c
in
V
c
c
F
a
a
g
ri
e
b
ru
iv
te
ll
it
e
c
A
s
a
a
o
b
.
P
p
ro
m
te
ra
n
E
G
P a th o g e n s
Pons et al. Ann Intensive Care. 2019BMR et TOS
• Portage BLSE avant Tx hépatique (n=734): 4,9% portage rectal
Bert et al. Emerg Infect Dis. 2012
• Infections urinaires après Tx rénale (n=2174): 118 épisodes
E. coli= 57,8% dont la moitié BLSE Vidal et al. Transplant Infect Dis. 2012
• Transplantation pulmonaire: 5,5% infections à BMR n= 1065
• Transplantation cardiaque: 2,2% Mortalité 8,3%
Bui et al. Transplantation. 2014
• Transplantation cardiaque (n=113): 19% des patients ont présenté
une infection à BMR dans les 6 mois suivant la greffe
Pons et al. Ann Intensive Care. 2019FDR candidose invasive
Gavaldà et al. Clin Microbiol Infect. 2014Fishman et al. N Engl J Med. 2007
Période 2-6 mois • Influence ++ des traitements prophylactiques: CMV/ PCP • Mais également: - Infections bactériennes - Infections fongiques - Autres infections virale: EBV, BK, Parvovirus B19
CMV: prophylaxie
3ème recommandations d’experts sur la PEC du CMV chez les TOS:
- Dépend du statut D+/R- ou R+
- Dépend de l’organe transplanté
Prophylaxie universelle Stratégie préemptive
ADNémie CMV ou infection Rare Habituelle
précoce
Prévention CMV Bonne efficacité Bonne efficacité
CMV tardif Habituel Rare
Facilité de mise en œuvre Facile Plus difficile
Prévention des autres virus HSV, VZV Non
Sécurité Toxicité médicamenteuse Moins de toxicité med.
Coût Coût médicamenteux Coût du monitorage
Kotton et al. Transplantation. 2018CMV
• Quasi-disparition des CMV précoces depuis l’utilisation la prophylaxie
• Impact sur la survenue de CMV tardifs
191 Tx cardiaques
3 mois de prophylaxie orale
(ganciclovir)
Maladies à CMV décalées mais
persistantes
Li et al. Clin Infect Dis. 2007
• Impact sur la résistance du CMV?Pneumocystose
• Egalement favorisée par une réactivation/infection CMV, une
leucopénie
• Toux sèche, décours subaigu mais ≠ VIH:
- Maladie plus aigue, plus hypoxémiante
- Plus rapidement progressive
- Plus souvent admis en réanimation
Roux et al. Emerg Infect Dis. 2014
• Faut-il traiter par corticoïdes ces malades? (Etude PIC en cours-
V. Lemiale)Pneumocystose
• Risque variable au cours du temps:
- Maximum théorique entre le 2ème et le 6ème mois
- Quasi-éradiquée à ce délai par la prophylaxie par Bactrim
• Incidence (hors prophylaxie) variable avec l’organe greffé:
- Coeur-poumons / poumons : 6,5 à 43%
- Coeur : 2 à 10% (jusqu’à 41%)
- Rein : 0,6 à 14%
- Foie : 3 à 11%
Rodriguez et al. Clin Microbiol Rev. 2004Pneumocystose
41 PCP/2842 TOS cohorte suisse
prospective entre 2008 et 2016
De Castro et al. Clin Microbiol Infect. 2010 Neofytos et al. Transplant Infect Dis. 2018Autres infections fongiques invasives
• Étude prospective TRANSNET :
- 16 centres aux USA ≈17 000
transplantations d'organes
- 1 208 épisodes d'infections fongiques
invasives
Pappas et al. Clin Infect Dis. 2010Autres infections fongiques invasives
Pappas et al. Clin Infect Dis. 2010Fishman et al. N Engl J Med. 2007
Infections tardives et TOS
RESITRA: 2169 patients > 6 mois après TOS
San Juan et al. Am J Transplant. 2007Infections tardives et TOS
942 TOS- cohorte prospective monocentrique
Durée médiane de suivi 789 jours
% Episodes infectieux tardifs (n=276)
100
90
80
70
60
50
40
30
20
10
0
D’après Cervera et al. Transplant Infect Dis. 2011CONCLUSION
Take home messages • Complications infectieuses très fréquentes la première année • Grèvent: - le pronostic vital du patient - le pronostic fonctionnel du greffon • Etiologies et donc ttt probabiliste en fonction de l’organe greffé, du site d’infection présumé et du délai après la greffe • Attention aux BMR/BHR et aux germes opportunistes
MERCI
Vous pouvez aussi lire

















































