INSTRUCTIONS FOR USE FOR: English Français
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous
INSTRUCTIONS FOR USE FOR:
®
en
English
fr
FrançaisINSTRUCTIONS FOR USE FOR: Efficacy:
GORE® PROPATEN® Vascular Graft At the end of the 12-month follow-up, primary patency,
secondary patency, and limb salvage rates for the GORE®
PROPATEN® Vascular Graft were 71.2%, 93.9%, and 95.8%,
I. INDICATIONS FOR USE
respectively. Comparatively, the GORE‑TEX® Stretch Vascular Graft
II. CONTRAINDICATIONS showed primary patency, secondary patency, and limb salvage
III. US CLINICAL EXPERIENCE rates of 71.0%, 91.7%, and 95.8%, respectively.
Long-term data are not available regarding improved patency
IV. PACKAGE HANDLING compared to marketed grafts.
V. TECHNICAL INFORMATION Safety:
VI. POSSIBLE COMPLICATIONS WITH THE USE OF ANY Two (2) GORE® PROPATEN® Vascular Graft subjects experienced
VASCULAR PROSTHESIS a total of two major device-related adverse events, both graft
infections. Three (3) GORE‑TEX® Stretch Vascular Graft subjects
VII. OPERATIVE TECHNIQUES experienced a total of four major device-related adverse events,
VIII. STERILITY a graft infection with an infected prosthetic mitral valve, a graft
infection, and a perigraft hematoma. There were no reported
IX. RESTERILIZATION cases of heparin induced thrombocyptopenia (HIT) and no
unanticipated adverse device effects (UADEs).
Survival at 12 months:
I. INDICATIONS FOR USE Kaplan-Meier estimates of survival at 12 months
GORE® PROPATEN® Vascular Grafts are intended for use as vascular were comparable between treatment groups, 92.5% (95% CI:
prostheses for replacement or bypass of diseased vessels in 84.8%, 96.3%) in the GORE® PROPATEN® Vascular Graft group and
patients suffering occlusive or aneurysmal diseases, in trauma 95.6% (95% CI: 88.7%, 98.3%) in the GORE‑TEX® Stretch Vascular
patients requiring vascular replacement, for dialysis access, or for Graft group. No device-related deaths were reported in the study.
other vascular procedures.
IV. PACKAGE HANDLING
II. CONTRAINDICATIONS Store in a cool dry place. This product has an expiration date
A. DO NOT use the GORE® PROPATEN® Vascular Graft in and should be used before the labeled “use by” (expiration) date
patients with known hypersensitivity to heparin, including marked on the box. The foil pouch is both a moisture barrier and
those patients who have had a previous incidence of HIT a sterile barrier. DO NOT use or store the graft if the foil pouch has
type II. been compromised.
B. DO NOT use any configuration of GORE® PROPATEN® To open the package, peel open the foil pouch and remove the
Vascular Grafts with Removable Rings, Non-Removable tray. Beginning at one corner, peel back the tray lid and gently
Rings or Integrated Rings for coronary artery bypass or remove the graft. Use clean gloves or atraumatic instruments
cerebral reconstruction procedures. when handling the graft.
C. DO NOT use GORE® PROPATEN® Vascular Grafts as a patch. If
cut and used as a patch, GORE® PROPATEN® Vascular Grafts V. TECHNICAL INFORMATION
may lack adequate transverse strength. A. The luminal surface of the GORE® PROPATEN® Vascular Graft
is bonded with fractionated active heparin of porcine origin
FOR PATCHING APPLICATIONS: (CARMEDA® BioActive Surface (CBAS® Surface)).
For cardiovascular procedures requiring patch materials, use B. The presence of heparin on the GORE® PROPATEN®
the appropriate GORE® ACUSEAL Cardiovascular Patch. Vascular Graft is not intended to serve as an alternative
to the surgeon’s chosen intraoperative or postoperative
III. US CLINICAL EXPERIENCE anticoagulation regimens. The physician should consider
Objectives: the need for intraoperative and / or postoperative
The primary objective of the US clinical study was to evaluate anticoagulation therapy based on the pharmacological
the safety and effectiveness of the GORE® PROPATEN® Vascular requirements and medical history of the patient.
Graft and demonstrate substantial equivalence to the GORE‑TEX® C. In the event of graft occlusion, established vascular
Stretch Vascular Graft in a peripheral application. prosthesis revision procedures should be considered.
Study Design: Appropriate revision procedure selection should be
This 200-subject, multi-centered, prospective, randomized, single- determined by the physician based on the specific case
blind clinical trial was designed to compare the GORE® PROPATEN® requirements.
Vascular Graft to the commercially available GORE‑TEX® Stretch D. DO NOT LET THE LUMINAL SURFACE OF THE GORE®
Vascular Graft for occlusive vascular disease in patients requiring PROPATEN® VASCULAR GRAFT DRY ONCE IT HAS BEEN
primary above-knee arterial bypass. WETTED.
The primary efficacy endpoint was primary patency at 12 months, E. With any vascular procedure, the possibility of HIT may
determined by hemodynamic evidence of blood flow. The primary exist. The incidence of HIT type II is extremely low in
safety endpoint was the major device-related adverse event rate vascular bypass patients receiving heparin over a period
at 12 months. of several days. If HIT type II is diagnosed, established
Study Enrollment: procedures for the treatment of this condition, including
immediate cessation of systemic heparin administration,
Eighteen (18) US sites enrolled patients in the study; 101 patients
should be followed.1,2,3 If symptoms persist, or the
received the GORE® PROPATEN® Vascular Graft while 99 patients
health of the patient appears compromised, alternative
received the GORE‑TEX® Stretch Vascular Graft. All grafts were thin
pharmaceutical or surgical procedures, including ligation or
walled with a 6 mm internal diameter.
removal of the graft, may be considered at the discretion of
Pre-procedure Subject Information: the attending physician.
Demographics and symptom grades were similar between the F. The total graft length printed on the package is the usable
GORE® PROPATEN® Vascular Graft and GORE‑TEX® Stretch Vascular length when the graft is placed under moderate tension.
Graft groups. Risk factors were also similar with the exception of (Refer to OPERATIVE TECHNIQUES - TENSIONING,
diabetes and hyperlipidemia. In the GORE® PROPATEN® Vascular Section VII. B.)
Graft and GORE‑TEX® Stretch Vascular Graft groups, respectively,
G. CORONARY ARTERY BYPASS PROCEDURES
pre-procedure demographics included average age (64.8,
67.3 years) and percent of male subjects (53.5%, 60.6%). In (Also refer to INDICATIONS FOR USE and
the GORE® PROPATEN® Vascular Graft and GORE‑TEX® Stretch CONTRAINDICATIONS) W. L. Gore & Associates, Inc., has
Vascular Graft groups, respectively, pre-procedure risk factors insufficient clinical and experimental data upon which to
included diabetes (27.8%, 14.3%), current tobacco use (55.4%, base any conclusion regarding the use of GORE® PROPATEN®
49.0%), hypertension (79.2%, 85.7%), and moderately elevated Vascular Grafts in coronary artery bypass procedures.
hyperlipidemia controlled through strict diet and medications H. AXILLOFEMORAL, FEMOROFEMORAL, and
(58.4%, 43.9%). In the GORE® PROPATEN® Vascular Graft and AXILLOBIFEMORAL BYPASS PROCEDURES
GORE‑TEX® Stretch Vascular Graft groups, respectively, 44.6% and The success of axillofemoral, femorofemoral, and
43.9% of subjects were enrolled with claudication and 55.4% and axillobifemoral bypasses depends in large part on the
56.1% with critical limb ischemia. implantation technique. Specific complications associated
with improperly implanted GORE® PROPATEN® Vascular
Grafts in these positions may include suture hole elongation
and mechanical disruption or tearing of the graft, suture
line, or host vessel.
1Failure to follow these techniques may result in • Begin implantation by pulling the graft from the
extreme blood loss, loss of limb function, loss of limb, axillary counterincision to the first portion of the
or death. Although experience indicates that the incidence axillary artery. The graft must be placed under
of these complications is extremely low, the following both the pectoralis major and the pectoralis minor
techniques MUST be employed if your treatment plan muscles.
includes one of the above procedures: The anastomosis must be performed in the first
• Consider the patient’s body weight and posture when portion of the axillary artery, proximal to the
determining the lengths of the tissue tunnel and the thoracoacromial trunk. This entails dissection and
graft. proximal control at the axillary-subclavian junction
• Drape the patient to allow full movement of the arm, under the clavicle. Correct placement in this area
shoulder girdle or legs when determining correct prevents excessive movement of the artery /
graft length. graft junction. Do not place the anastomosis on
• Avoid protracted hyperabduction of the arm. the second or third portion of the axillary artery.
Prolonged hyperabduction may lead to brachial Rotate the axillary artery with clamps so that
plexus injury. the arteriotomy is made on its inferior border,
• Allow sufficient length to avoid stressing the axillary placing the arteriotomy as close as possible to
or femoral anastomoses throughout the full range the first rib to minimize subsequent movement.
of movement of the arm, shoulder girdle, or legs. Correctly bevel the axillary anastomosis. Stress on the
Surgeons suggest that the graft be placed under both anastomosis is minimized when the graft is placed
the pectoralis major and pectoralis minor. parallel to the axillary artery.
• Cutting the graft slightly longer than necessary has • Continue the procedure by pulling the graft from
been reported by some surgeons to reduce further the axillary counterincision to the femoral incision
the risk of stressing the graft or the anastomoses. with use of an appropriate tunneling instrument.
• Correctly bevel the axillary anastomosis. Stress on the The graft should lie in the mid-axillary line
graft is minimized when the graft is placed parallel to minimize kinking when the patient bends
(0°) to the axillary artery. Therefore, the anastomotic forward at the waist.
angle should be as small as possible and should not CAUTION THE PATIENT AGAINST EXTREME OR ABRUPT
exceed 25° relative to the cut edge of the graft. MOVEMENTS OF THE ARM, SHOULDER, OR LEGS DURING
• Anastomose the graft close to the rib cage on the first A CONVALESCENT PERIOD OF SIX-TO-EIGHT WEEKS TO
portion of the axillary artery. Do not place the ALLOW FOR ADEQUATE HEALING. ROUTINE ACTIVITIES
anastomosis on the third portion of the axillary SUCH AS REACHING OUT IN FRONT, RAISING ARMS
artery. ABOVE THE SHOULDER LEVEL, THROWING, PULLING,
STRIDING, OR TWISTING SHOULD BE AVOIDED.
FAILURE TO FOLLOW THESE PROCEDURES MAY RESULT
IN EXTREME BLOOD LOSS, LOSS OF LIMB FUNCTION,
LOSS OF LIMB, OR DEATH.
I. VASCULAR ACCESS PROCEDURES
Patients should be carefully monitored when using GORE®
PROPATEN® Vascular Grafts for vascular access. Puncture
sites must be adequately separated when repeated needle
punctures of the graft are necessary. Multiple punctures in
the same area may lead to disruption of the graft material
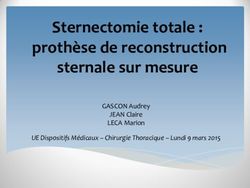
RECOMMENDED or formation of a perigraft hematoma or pseudoaneurysm.
ANASTOMOTIC For additional information, refer to the brochure GORE‑TEX®
PLACEMENT AND Vascular Grafts for Hemodialysis: Techniques for the Care
ABDUCTION TEST and Cannulation of A-V Fistulas, available from W. L. Gore &
Associates.
If the GORE® PROPATEN® Vascular Graft with Removable
0°-25° Rings is used for vascular access, the rings must be removed
RECOMMENDED from any cannulation region prior to implant (Reference,
ANGLE OF BEVEL “OPERATIVE TECHNIQUES - GORE® PROPATEN® VASCULAR
GRAFT WITH REMOVABLE RINGS,” Section VII.C.4.). Do not
puncture the graft at or near any ringed section.
• An alternative technique reported by some
surgeons4,5 to further avoid stressing the axillary VI. POSSIBLE COMPLICATIONS WITH THE USE OF ANY
anastomosis is to route the graft parallel and adjacent VASCULAR PROSTHESIS
to the axillary artery posterior to the pectoralis minor A. Complications which may occur in conjunction with
muscle for approximately 8-10 cm before forming a the use of any vascular prosthesis include but are not
gentle curve to its inferior course. limited to: redundancy; infection; ultrafiltration or
perigraft seroma; thrombosis; mechanical disruption
or tearing of the suture line, graft, and / or host
vessel; excessive suture hole bleeding; formation of
pseudoaneurysms due to excessive, localized, or large
needle punctures; or perigraft hematomas.
B. A possible complication which may occur in
conjunction with the use of any heparin-containing
product: HIT type II (see section V. E on previous page).
VII. OPERATIVE TECHNIQUES
A. ALL GORE® PROPATEN®
VASCULAR GRAFT CONFIGURATIONS
1. To avoid damage or contamination, always use clean
gloves and atraumatic instruments when handling
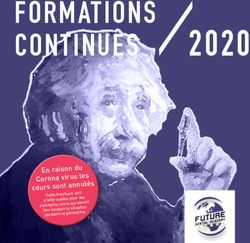
GRAFT TO AXILLARY ARTERY END-TO-SIDE the GORE® PROPATEN® Vascular Graft. Always protect
ANASTOMOSIS. THE GRAFT IS PLACED PARALLEL the graft from damage by heavy or sharp objects.
TO THE AXILLARY ARTERY POSTERIOR TO THE 2. When applying clamps, care should be taken to avoid
PECTORALIS MINOR MUSCLE FOR 8 TO 10 CM mechanical damage to, or disruption of, the graft. Use
BEFORE GENTLY CURVING TOWARD THE PROPOSED the appropriate atraumatic or guarded (for example,
ANASTOMOTIC SITE. rubber shod) clamps. Avoid repeated, localized
To aid in proper parallel placement of the graft in clamping or excessive clamping on any section
relation to the axillary artery, some surgeons6 have of the graft.
reported the use of an axillary counterincision near 3. It is not necessary to preclot the
the third part of the artery. GORE® PROPATEN® Vascular Graft.
24. Blood or plasma leakage may occur if appropriate C. OPERATIVE TECHNIQUES - GORE® PROPATEN® VASCULAR
handling techniques are not observed. Do not allow GRAFT WITH REMOVABLE RINGS
the graft to contact organic solvents such as alcohol 1. GORE® PROPATEN® Vascular Grafts with Removable
or Betadine® Solution. Avoid excessive manipulation Rings consist of a reinforced expanded PTFE Vascular
of the graft in contact with tissue fluids or blood, as Graft and an additional thin film to which rings
well as forcing irrigating solutions through the graft are attached. This design allows the surgeon to
wall or filling the graft with blood prior to passing it remove rings without damaging or compromising
through the tissue tunnel. the mechanical integrity of the graft. Following ring
5. The correct graft length for each procedure must removal, portions of the additional thin film are
be carefully determined, taking into consideration normally visible on the graft and removed ring(s).
the patient’s body weight and posture, and the 2. Use a tunneler to create a tissue tunnel that closely
range of motions likely to be encountered across the approximates the graft diameter, and allows free
anatomical area of the graft implantation. The graft passage of FEP rings. A tissue tunnel that is too tight
should never be too short. may disrupt ring attachment.
6. Failure to correctly cut the GORE® PROPATEN® Vascular 3. To prevent ring detachment when passing a graft
Graft may damage the outer reinforcing layer and through an incision, avoid catching the rings on the
may result in aneurysmal dilatation or reduced suture edge of the incision or tunneler.
retention strength. When cutting the graft, gently 4. RING REMOVAL: To avoid damaging the graft, do
pull the graft taut and determine the correct length. NOT use surgical blades or sharp instruments. Care
Cut the graft with a sharp surgical instrument. DO should be taken not to damage the reinforcing
NOT PULL OR PEEL THE OUTER REINFORCING LAYER layer immediately beneath the additional thin film
FROM ANY AREA OF THE GRAFT. IF THE OUTER to which the rings are attached. Following ring
REINFORCING LAYER BECOMES FRAYED AT THE END removal, portions of the additional thin film are
OF THE GRAFT, CAREFULLY TRIM THAT PORTION OF normally visible on the graft and removed ring(s).
THE GRAFT WITH A SHARP SURGICAL INSTRUMENT. IF THE REINFORCING LAYER APPEARS FRAYED OR
7. Use a tunneler, such as the GORE® Tunneler, to create DAMAGED, THAT SEGMENT OF THE GRAFT SHOULD
a tissue tunnel that closely approximates the graft NOT BE USED.
diameter. A tissue tunnel that is too loose may result To remove rings from the end of a ringed section
in delayed or insufficient perigraft tissue attachment, or before suturing: Hold the graft firmly with one
and may be a contributing factor to perigraft seroma gloved hand. With the other hand, gently grasp
formation. and lift a ring(s) with gloved fingers or atraumatic
8. Anastomotic angles vary with the vascular procedure instrument and slide it off the end of the graft.
being performed. Use of an appropriate anastomotic To remove rings from within a ringed section or
angle may minimize undue stresses which may lead after suturing: Hold the graft firmly with one gloved
to mechanical disruptions of the graft, host vessel, hand. With the other hand, loosen a ring(s) by gently
and / or suture lines. grasping and lifting with an atraumatic instrument.
9. Use only nonabsorbable, monofilament sutures, such Carefully cut each ring with blunt-nosed scissors and
as GORE‑TEX® Suture, of a size appropriate for the peel off the severed ring(s).
nature of the reconstruction. Do not use a full radius 5. Reference, “CONTRAINDICATIONS,” Section II. B.;
cutting needle as it may damage the graft. “TECHNICAL INFORMATION,” Section V. F.,G., and H.;
10. Undue anastomotic bleeding may occur if excessive and, “OPERATIVE TECHNIQUES: ALL GORE® PROPATEN®
tension causes suture holes to elongate or tear, if the VASCULAR GRAFT CONFIGURATIONS,” Section VII. A.
needle-to-suture diameter ratio is too great, or if gaps
occur between the graft and the host vessel. Use D. OPERATIVE TECHNIQUES ‑ GORE® PROPATEN®
appropriate suture placement and bites and avoid VASCULAR GRAFT WITH INTEGRATED RINGS
undue tension on the suture line. Hemostatic agents 1. GORE® PROPATEN® Vascular Grafts with Integrated
such as topical thrombin and Surgicel® Absorbable Rings consist of a reinforced ePTFE GORE‑TEX®
Hemostat may be used to minimize anastomotic Vascular Graft with integrated ePTFE radial support
bleeding. The manufacturers’ instructions for these within the wall of the graft.
products should be observed. 2. The ePTFE radial support is NOT removable. The
11. The physician should ensure that the patient has GORE® PROPATEN® Vascular Graft with Integrated
been informed as to appropriate postoperative care. Rings is a unibody design incorporating continuous
ePTFE microstructure between radial support and
B. OPERATIVE TECHNIQUES - TENSIONING non‑radial support sections of the graft. Attempting
1. When handling or tensioning the to remove the radial support will damage the graft.
GORE® PROPATEN® Vascular Graft, avoid using 3. The ePTFE radial support sections of the GORE®
excessive force or high rates of force which could lead PROPATEN® Vascular Graft with Integrated Rings can
to graft disruption. be incorporated into the anastomosis.
2. Even though the GORE® PROPATEN® Vascular Graft The integrated radial support can be cut and sewn
affords some extensibility, the graft must still be cut through using appropriate cutting and suturing
to the correct length. techniques.
3. After completing the proximal anastomosis, apply Reference, “OPERATIVE TECHNIQUES: ALL GORE®
moderate tension to the entire length of the PROPATEN® VASCULAR GRAFT CONFIGURATIONS,”
GORE® PROPATEN® Vascular Graft in order to remove Section VII. A.
the extensibility. Ensure that moderate tension is 4. When applying clamps, care should be taken to avoid
transmitted from the distal end of the graft to the mechanical damage or disruption to the GORE®
proximal (first) anastomosis immediately prior to PROPATEN® Vascular Graft with Integrated Rings. Use
cutting the graft to length. Blue orientation markers the appropriate atraumatic or guarded (for example,
can aid in determining moderate tension. rubber shod) clamps. Avoid repeated, localized
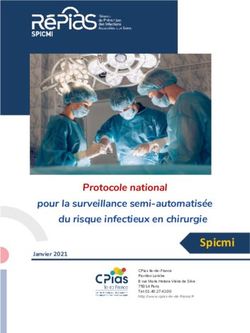
4. Reasonable assurance of moderate tension is clamping or excessive clamping on any section of the
provided when the blue orientation markers, graft.
illustrated in the following two figures, change 5. Reference, “Technical Information,” Section V. G.,
configuration from Figure A to Figure B at the “Coronary Artery Bypass Procedures,” and "OPERATIVE
proximal and distal anastomotic sites. TECHNIQUES: ALL GORE® PROPATEN® VASCULAR
GRAFT CONFIGURATIONS,” Section VII. A.
VIII. STERILITY
GORE® PROPATEN® Vascular Grafts are supplied STERILE unless the
integrity of the package has been compromised. The sterilization
Figure A Figure B method is marked on the box. Sterility will be maintained until
RELAXED MODERATE the labeled “use by” (expiration) date marked on the box.
TENSION
IX. RESTERILIZATION
DO NOT RESTERILIZE THE GORE® PROPATEN®
VASCULAR GRAFT.
3REFERENCES
1. Ortel TL, Chong BH. New treatment options for heparin-
induced thrombocytopenia. Seminars in Hematology
1998; 35 (4): 26-34.
2. Almeida JI, Coats R, Liem TK, Silver D. Reduced morbidity
and mortality rates of heparin-induced thrombocytopenia.
Journal of Vascular Surgery 1998; 27 (2): 309-16.
3. Warkentin TE, Grienacher A, Koster A, Lincoff AM.
Treatment and prevention of heparin-induced
thrombocytopenia: American College of Chest Physicians
evidence-based clinical practice guidelines (8th edition).
Chest 2008;133:340S-380S.
4. Landry GJ, Moneta GL, Taylor Jr. LM, Porter JM.
Axillobifemoral bypass. Annals of Vascular Surgery
2001;14(3):296-305.
5. Taylor Jr. LM, Park TC, Edwards JM, Yeager RA,
McConnell DC, Moneta GA, Porter JM. Acute disruption
of polytetrafluoroethylene grafts adjacent to axillary
anastomoses: a complication of axillofemoral grafting.
Journal of Vascular Surgery 1994;20:520-528.
6. Bunt TJ, Moore W. Optimal proximal anastomosis /
tunnel for axillofemoral grafts. Journal of Vascular Surgery
1986;3:673-676.
DEFINITIONS
Use By
Caution
Consult Instructions for Use
2
STERILIZE Do Not Resterilize
Do Not Reuse
Catalogue Number
Batch Code
CAUTION: USA Federal Law restricts the sale, distribution, or
use of this device to, by, or on the order of a physician.
Sterile
Sterilized using Ethylene Oxide
Do Not Use if Package is Damaged
Keep Dry
Store in a Cool Place
AXL Axillobifemoral
Diameter
Fibril Length 25 Microns (Nominal)
Fibril Length Radial Support 5 Microns (Nominal)
IR Integrated Rings
Length
Manufacturer
Non-Removable Rings
Removable Rings
Ring Section
Standard Wall
Thin Wall
4MODE D'EMPLOI : 67,3 ans et le pourcentage de sujets masculins de 53,5 % et de
Prothèse vasculaire GORE® 60,6 %. Dans le groupe recevant la prothèse vasculaire GORE®
PROPATEN® et celui recevant la prothèse vasculaire extensible
PROPATEN® GORE‑TEX®, les facteurs de risque pré-procédure incluaient,
respectivement, le diabète (27,8 %, 14,3 %), le tabagisme
I. INDICATIONS D’UTILISATION (55,4 %, 49 %), l’hypertension (79,2 %, 85,7 %) et une
hyperlipidémie moyennement élevée régulée par un régime
II. CONTRE-INDICATIONS alimentaire strict et la prise de médicaments (58,4 %, 43,9 %).
III. EXPÉRIENCE CLINIQUE AUX ÉTATS-UNIS Dans le groupe recevant la prothèse vasculaire GORE® PROPATEN®
et celui recevant la prothèse vasculaire extensible GORE‑TEX®,
IV. MANIPULATION DU CONDITIONNEMENT
44,6 % et 43,9 %, respectivement, des sujets admis présentaient
V. INFORMATIONS TECHNIQUES une claudication et 55,4 % et 56,1 %, respectivement, une
VI. COMPLICATIONS ÉVENTUELLES ASSOCIÉES AVEC ischémie critique d’un membre.
L'UTILISATION DE TOUTE PROTHÈSE VASCULAIRE Efficacité :
VII. TECHNIQUES OPÉRATOIRES À la fin de la période de suivi sur 12 mois, les taux de perméabilité
primaire, secondaire et de sauvetage de membre pour la prothèse
VIII. STÉRILITÉ vasculaire GORE® PROPATEN® étaient respectivement de 71,2 %,
IX. RESTÉRILISATION 93,9 % et 95,8 %. Par comparaison, la prothèse vasculaire
extensible GORE‑TEX® a produit des taux de perméabilité primaire,
secondaire et de sauvetage de membre de 71,0 %, 91,7 % et
95,8 %, respectivement.
I. INDICATIONS D’UTILISATION Aucune donnée à long terme n’est disponible concernant
Les prothèses vasculaires GORE® PROPATEN® sont destinées à être l’amélioration de la perméabilité par rapport aux prothèses
utilisées comme prothèses vasculaires pour le remplacement ou commercialisées.
le pontage de vaisseaux malades chez les patients souffrant de Innocuité :
maladies occlusives ou anévrysmales, chez les patients victimes
de traumatismes et nécessitant un remplacement vasculaire, pour Deux (2) sujets porteurs de prothèse vasculaire GORE® PROPATEN®
un accès de dialyse ou pour d’autres procédures vasculaires. ont connu au total deux effets indésirables majeurs liés au
dispositif, tous deux concernant des infections de prothèse. Trois
(3) sujets porteurs de prothèse vasculaire extensible GORE-TEX®
II. CONTRE-INDICATIONS ont développé au total quatre effets indésirables majeurs liés
A. NE PAS utiliser la prothèse vasculaire GORE® PROPATEN® au dispositif, une infection de prothèse avec une valvule mitrale
chez des patients présentant une hypersensibilité connue prothétique infectée, une infection de prothèse et un hématome
vis-à-vis de l’héparine, y compris les patients ayant une périprothétique. Il n’a été signalé aucun cas de thrombopénie
incidence passée de TIH de type II. induite par l’héparine (TIH) ni aucun effet indésirable lié au
B. N’utiliser AUCUNE configuration de prothèse vasculaire dispositif non anticipé.
GORE® PROPATEN® avec anneaux amovibles, anneaux Survie à 12 mois :
inamovibles ou anneaux intégrés pour une procédure de Les estimations de Kaplan-Meier analysant la survie à 12 mois
pontage coronarien ou de reconstruction cérébrale. étaient comparables entre les groupes de traitement : 92,5 %
C. NE PAS utiliser les prothèses vasculaires GORE® PROPATEN® (IC à 95 % : 84,8 %, 96,3 %) dans le groupe ayant reçu la prothèse
comme des patchs. Si elles sont coupées et utilisées comme vasculaire GORE® PROPATEN® et 95,6 % (IC à 95 % : 88,7 %, 98,3 %)
des patchs, les prothèses vasculaires GORE® PROPATEN® dans le groupe ayant reçu la prothèse vasculaire extensible
risquent de ne pas présenter une force transversale GORE‑TEX®. Aucun décès lié au dispositif n’a été signalé au cours
adéquate. de l’étude.
POUR LES APPLICATIONS PAR PATCH : IV. MANIPULATION DU CONDITIONNEMENT
Pour les procédures cardio-vasculaires qui nécessitent Stocker dans un endroit frais et sec. Ce produit comprend une
l’utilisation de patchs, utiliser le patch cardio-vasculaire date de péremption (« À utiliser avant le ») indiquée sur la boîte
GORE® ACUSEAL approprié. avant laquelle il doit être utilisé. La pochette en aluminium
constitue à la fois une barrière contre l'humidité et une barrière
III. EXPÉRIENCE CLINIQUE AUX ÉTATS-UNIS stérile. NE PAS utiliser ni stocker la prothèse si la pochette en
Objectifs : aluminium a été compromise.
L’objectif principal de l’étude clinique menée aux États-Unis Pour ouvrir l’emballage, ouvrir la pochette en aluminium en
consistait à évaluer l’innocuité et l’efficacité de la prothèse la décollant, puis retirer le plateau. En commençant par un
vasculaire GORE® PROPATEN® et à démontrer son équivalence coin, décoller le couvercle du plateau et retirer avec précaution
substantielle par rapport à la prothèse vasculaire extensible la prothèse. Utiliser des gants propres ou des instruments
GORE‑TEX® concernant une application périphérique. atraumatiques propres afin de manipuler la prothèse.
Conception de l’étude :
Cet essai clinique à simple insu, randomisé, prospectif et V. INFORMATIONS TECHNIQUES
multicentrique de 200 sujets visait à comparer la prothèse A. La face luminale de la prothèse vasculaire GORE®
vasculaire GORE® PROPATEN® à la prothèse vasculaire extensible PROPATEN® est enduite d’héparine active fractionnée
GORE‑TEX® actuellement en vente pour les maladies vasculaires d’origine porcine (CARMEDA® BioActive Surface [CBAS®
occlusives chez les patients exigeant un pontage artériel primaire Surface]).
au dessus du genou. B. La présence d’héparine sur la prothèse vasculaire GORE®
Le critère d’efficacité principal était la perméabilité primaire à PROPATEN® n’est pas supposée remplacer les schémas
12 mois, déterminée par preuve hémodynamique de circulation posologiques d'anticoagulothérapie peropératoires et
du sang. Le critère d’innocuité principal était le taux d’effets postopératoires prescrits par le chirurgien. Ce dernier
indésirables majeurs associés au dispositif à 12 mois. décidera de la nécessité d’une anticoagulothérapie
Recrutement dans l’étude : peropératoire et/ou postopératoire en se basant sur les
Dix-huit (18) centres situés aux États-Unis ont admis des patients exigences pharmacologiques et les antécédents médicaux
dans le cadre de cette étude ; 101 patients ont reçu la prothèse du patient.
vasculaire GORE® PROPATEN® et 99 la prothèse vasculaire C. Si une occlusion de la prothèse survient, considérer les
extensible GORE‑TEX®. Toutes les prothèses avaient une paroi fine procédures de révision établies pour la prothèse vasculaire.
et un diamètre interne de 6 mm. Le choix de la procédure de révision qui convient revient au
Informations sur les sujets avant la procédure : médecin qui se basera sur les exigences spécifiques du cas.
Les données démographiques et niveaux de symptômes étaient D. NE PAS LAISSER LA FACE LUMINALE DE LA PROTHÈSE
similaires pour le groupe recevant la prothèse vasculaire GORE® VASCULAIRE GORE® PROPATEN® SÉCHER APRÈS L'AVOIR
PROPATEN® et celui recevant la prothèse vasculaire extensible HUMIDIFIÉE.
GORE‑TEX®. Les facteurs de risque étaient également similaires, E. Toute intervention vasculaire entraîne potentiellement
à l’exception du diabète et de l’hyperlipidémie. Dans le groupe le risque d’une TIH. L’incidence de TIH de type II est
recevant la prothèse vasculaire GORE® PROPATEN® et celui extrêmement faible chez les patients subissant un pontage
recevant la prothèse vasculaire extensible GORE‑TEX®, l’âge vasculaire et recevant de l’héparine pendant plusieurs
moyen pré-procédure était respectivement de 64,8 ans et de jours. Si une TIH de type II est diagnostiquée, suivre
les procédures établies pour le traitement de cet état,
y compris l’interruption immédiate de l’administration
systémique d’héparine.1,2,3 Si les symptômes persistent,
ou si la santé du patient paraît compromise, d’autres
5procédures pharmaceutiques ou chirurgicales, y compris la
ligature ou le retrait de la prothèse, peuvent être envisagées
à la discrétion du médecin traitant.
F. La longueur totale de la prothèse vasculaire indiquée sur
l’emballage est la longueur utilisable lorsque la prothèse
vasculaire est soumise à une tension modérée. (Voir
« TECHNIQUES OPÉRATOIRES - ÉTIREMENT », section VII. B.)
G. PROCÉDURES DE PONTAGE CORONARIEN
(Voir aussi INDICATIONS D’UTILISATION et CONTRE-
INDICATIONS) W. L. Gore & Associates, Inc. ne dispose
pas de données expérimentales et cliniques suffisantes
sur lesquelles elle peut baser des conclusions concernant
l’utilisation des prothèses vasculaires GORE® PROPATEN®
dans les procédures de pontage coronarien.
H. PROCÉDURES DE PONTAGE AXILLOFÉMORAL,
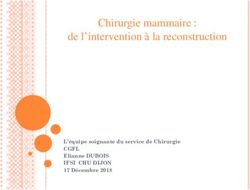
FÉMOROFÉMORAL et AXILLOBIFÉMORAL ANASTOMOSE TERMINO-LATÉRALE PROTHÈSE/
Le succès des pontages axillofémoraux, fémorofémoraux et ARTÈRE AXILLAIRE. LA PROTHÈSE EST PLACÉE
axillobifémoraux dépend en grande partie de la technique PARALLÈLEMENT À L’ARTÈRE AXILLAIRE EN POSITION
d’implantation. Les complications spécifiques associées à POSTÉRIEURE PAR RAPPORT AU MUSCLE PETIT
une implantation incorrecte des prothèses vasculaires GORE® PECTORAL SUR 8 À 10 CM AVANT DE L’INCURVER
PROPATEN® à ces endroits peuvent inclure l’élongation des DÉLICATEMENT EN DIRECTION DU SITE PRÉVU POUR
trous de suture et la rupture mécanique ou la déchirure de la L’ANASTOMOSE.
prothèse, de la ligne de suture ou du vaisseau receveur. • Pour faciliter la mise en place parallèle correcte de
Si les techniques d’implantation correctes ne sont pas la prothèse par rapport à l’artère axillaire, certains
suivies, il peut s’en suivre une hémorragie importante, chirurgiens6 ont signalé l’utilisation d’une contre-
la perte de l’usage d’un membre, la perte d’un incision axillaire près de la troisième partie de l’artère.
membre ou le décès. Bien que d’expérience, l’incidence de • Commencer l’implantation en tirant sur la prothèse à
ces complications soit extrêmement faible, les techniques partir de la contre-incision axillaire jusqu’à la première
suivantes DOIVENT être suivies si le plan de traitement inclut portion de l’artère axillaire. La prothèse doit être placée
l’une des procédures mentionnées ci-dessus : à la fois sous le muscle grand pectoral et le muscle
• Considérer le poids et la posture du patient lors de la petit pectoral. L’anastomose doit être exécutée dans
détermination de la longueur du tunnel tissulaire et la première portion de l’artère axillaire, en position
de la prothèse. proximale par rapport au tronc acromiothoracique.
• Recouvrir le patient de champs stériles de façon à Ceci implique la dissection et le contrôle proximal à
pouvoir bouger son bras, sa ceinture scapulaire ou la jonction axillaire-sous-clavière sous la clavicule. La
ses jambes pour déterminer la longueur correcte de mise en place correcte dans cette zone empêche le
la prothèse. mouvement excessif de la jonction artère/prothèse.
• Éviter une hyperabduction prolongée du bras, car Ne pas placer l’anastomose sur la deuxième ou la
celle-ci peut entraîner une lésion du plexus brachial. troisième portion de l’artère axillaire. Faire pivoter
• Prévoir une longueur suffisante pour éviter de trop l’artère axillaire avec des clamps pour effectuer
tirer sur les anastomoses axillaires ou fémorales lors l’artériotomie sur son bord inférieur, en plaçant
du mouvement du bras, de la ceinture scapulaire ou l’artériotomie le plus près possible de la première
des jambes du patient. Les chirurgiens suggèrent côte afin de minimiser un mouvement subséquent.
de placer la prothèse à la fois sous le muscle grand Biseauter correctement l’anastomose axillaire. La
pectoral et le muscle petit pectoral. tension sur l’anastomose est minimisée lorsque la
• Certains chirurgiens ont également observé que prothèse est placée parallèlement à l’artère axillaire.
le fait de couper la prothèse un peu plus long que • Continuer la procédure en tirant sur la prothèse de la
nécessaire réduisait davantage le risque de tension contre-incision axillaire jusqu’à l’incision fémorale en
exercée sur la prothèse ou sur les anastomoses. utilisant un instrument approprié de tunnellisation. La
• Biseauter correctement l’anastomose axillaire. prothèse doit reposer sur la ligne médio-axillaire
La tension sur la prothèse est moindre lorsque la pour minimiser les coudures lorsque le patient se
prothèse est placée parallèlement (0°) à l’artère penche vers l’avant.
axillaire. En conséquence, l’angle anastomotique doit- INDIQUER AU PATIENT D’ÉVITER DE FAIRE DES
il être aussi petit que possible et ne pas dépasser 25° MOUVEMENTS EXTRÊMES OU BRUSQUES DU BRAS,
par rapport au bord coupé de la prothèse. DE L’ÉPAULE OU DES JAMBES DURANT LA PÉRIODE DE
• Réaliser l’anastomose de la prothèse près de la cage CONVALESCENCE QUI DURERA SIX À HUIT SEMAINES
thoracique sur la première portion de l’artère axillaire. DE FAÇON À CE QU’UNE CICATRISATION ADÉQUATE
Ne pas réaliser l’anastomose sur la troisième portion AIT LIEU. TOUTES LES ACTIVITÉS DE ROUTINE TELLES
de l’artère axillaire. QUE TENDRE LES BRAS VERS L’AVANT, LEVER LES
BRAS AU-DESSUS DU NIVEAU DES ÉPAULES, JETER OU
TIRER QUELQUE CHOSE, MARCHER À GRANDS PAS OU
EFFECTUER DES TORSIONS DOIVENT ÊTRE ÉVITÉES.
SI CES INSTRUCTIONS NE SONT PAS SUIVIES, IL PEUT
S’EN SUIVRE UNE HÉMORRAGIE IMPORTANTE, UNE
PERTE DE L’USAGE D’UN MEMBRE, UNE PERTE D’UN
MEMBRE OU LE DÉCÈS.
I. PROCÉDURES D’ABORD VASCULAIRE
Surveiller les patients de très près lorsque les prothèses
vasculaires GORE® PROPATEN® sont utilisées pour un abord
vasculaire. Lorsque la prothèse demande plusieurs points,
TECHNIQUE
faire bien attention à ne pas piquer toujours au même
ANASTOMOTIQUE endroit, car ceci risquerait d’entraîner une rupture du
RECOMMANDÉE ET matériau de la prothèse ou la formation d’un hématome
TEST D’ABDUCTION autour de la prothèse ou d’un pseudo-anévrysme. Pour
plus d’informations, consulter la brochure sur les prothèses
vasculaires GORE‑TEX® pour hémodialyse : techniques
0°-25° d’entretien et de canulation des fistules artérioveineuses,
ANGLE DU
BISEAU disponible auprès de W. L. Gore & Associates.
RECOMMANDÉ Si la prothèse vasculaire GORE® PROPATEN® à anneaux
amovibles est utilisée pour établir une voie d’abord
vasculaire, les anneaux doivent être retirés des zones
• Une autre technique indiquée par certains
de canulation avant l’implantation (voir « TECHNIQUES
chirurgiens4,5 pour éviter encore davantage de
OPÉRATOIRES - PROTHÈSE VASCULAIRE GORE® PROPATEN®
tendre l’anastomose axillaire consiste à acheminer la
À ANNEAUX AMOVIBLES », Section VII. C. 4.). Ne pas
prothèse parallèlement et à côté de l’artère axillaire,
ponctionner la prothèse au niveau d’une des sections à
en position postérieure par rapport au muscle petit
anneaux ou à proximité de celles-ci.
pectoral sur 8 à 10 cm environ avant de former une
courbe douce vers sa trajectoire inférieure.
6VI. COMPLICATIONS ÉVENTUELLES ASSOCIÉES AVEC trous se forment entre la prothèse et le vaisseau
L’UTILISATION DE TOUTE PROTHÈSE VASCULAIRE receveur. Utiliser l’emplacement et les points de
A. Les complications qui peuvent survenir lors de suture appropriés et éviter d’exercer une tension
l’utilisation de n’importe quelle prothèse vasculaire excessive sur la ligne de suture. On peut utiliser des
incluent sans s’y limiter : redondance ; infection ; agents hémostatiques tels que de la thrombine
ultrafiltration ou séromes autour de la prothèse ; topicale et l’hémostatique résorbable Surgicel® pour
thrombose ; rupture mécanique ou déchirure de la minimiser l’hémorragie anastomotique. Respecter
ligne de suture, de la prothèse et/ou du vaisseau les instructions données par les fabricants de ces
receveur ; hémorragie excessive par les points de produits.
suture ; formation de pseudo-anévrysmes provoqués 11. Le médecin devra s’assurer que le patient a bien été
par les perforations de l'aiguille qui sont soit trop informé des soins postopératoires à suivre.
nombreuses, trop grandes ou faites au même endroit ;
ou formation d’hématomes autour de la prothèse. B. TECHNIQUES OPÉRATOIRES - ÉTIREMENT
B. Une complication pouvant se produire en association 1. Lors de la manipulation ou de l’étirement de la
à l’utilisation des produits à base d’héparine : TIH de prothèse vasculaire GORE® PROPATEN®, éviter
type II (consulter la section V. E., page précédente). d’exercer une force excessive ou de fréquence élevée
pour éviter de la déchirer.
VII. TECHNIQUES OPÉRATOIRES 2. Bien que la prothèse vasculaire GORE® PROPATEN®
présente une certaine extensibilité, elle doit être
A. TOUTES LES CONFIGURATIONS DE PROTHÈSES coupée à la longueur correcte.
VASCULAIRES GORE® PROPATEN® 3. Une fois l’anastomose proximale terminée, exercer
1. Afin d’éviter d’endommager ou de contaminer la une tension modérée sur toute la longueur de la
prothèse vasculaire GORE® PROPATEN® lors de la prothèse vasculaire GORE® PROPATEN® afin d’enlever
manipulation, toujours utiliser des gants propres et toute extensibilité. S’assurer qu’une tension modérée
des instruments atraumatiques propres. Toujours soit transmise de l’extrémité distale de la prothèse
protéger la prothèse de façon à ce qu’elle ne soit pas à l’anastomose (première) proximale juste avant de
endommagée par des objets tranchants ou lourds. couper la prothèse à la longueur correcte. Les repères
2. Lors de la mise en place de clamps, prendre bien bleus d’orientation peuvent aider à déterminer une
soin d’éviter tout dommage mécanique ou déchirure tension modérée.
de la prothèse. Utiliser des clamps appropriés 4. La tension modérée appliquée est raisonnable
atraumatiques ou recouverts d’une gaine protectrice lorsque les repères bleus d’orientation, illustrés dans
(en caoutchouc, par exemple). Éviter les clampages les deux figures suivantes, passent de la configuration
répétés, toujours au même endroit ou trop forts sur représentée à la figure A à celle de la figure B aux
une section quelconque de la prothèse. sites anastomotiques distaux et proximaux.
3. Il n’est pas nécessaire de précoaguler la prothèse
vasculaire GORE® PROPATEN®.
4. Une fuite plasmatique ou sanguine peut avoir lieu
si les techniques de manipulation appropriées ne
sont pas respectées. Ne pas laisser la prothèse entrer
en contact avec des solvants organiques tels que Figure A Figure B
de l’alcool ou de la Betadine® (solution). Ne pas
manipuler plus que nécessaire la prothèse lorsque DÉTENDUE TENSION
celle-ci est en contact avec les liquides interstitiels MODÉRÉE
ou le sang, éviter également de forcer les solutions
d’irrigation au travers de la paroi de la prothèse ou de
remplir la prothèse de sang avant de la faire passer
dans le tunnel tissulaire. C. TECHNIQUES OPÉRATOIRES - PROTHÈSE VASCULAIRE
5. La longueur correcte de la prothèse vasculaire doit GORE® PROPATEN® À ANNEAUX AMOVIBLES
être déterminée avec soin pour chaque procédure. 1. Les prothèses vasculaires GORE® PROPATEN® à
Prendre en compte le poids et la posture du anneaux amovibles consistent en une prothèse
patient ainsi que tous les mouvements qui sont vasculaire en PTFE expansé renforcé et en un film
susceptibles d’être faits dans la région anatomique mince supplémentaire auquel sont attachés les
de l’implantation de la prothèse. La prothèse ne doit anneaux. Cette conception permet au chirurgien de
jamais être trop courte. retirer les anneaux sans endommager la prothèse
6. Si la prothèse vasculaire GORE® PROPATEN® n’est pas ou compromettre son intégrité mécanique. Après
correctement coupée, l’enveloppe externe renforcée le retrait des anneaux, des portions du film mince
peut être abîmée, ce qui pourrait entraîner une supplémentaire sont normalement visibles sur la
dilatation anévrysmale ou une réduction de la force prothèse et sur les anneaux retirés.
de rétention des sutures. Couper la prothèse en 2. À l’aide d’un tunnellisateur, créer un tunnel tissulaire
tirant doucement dessus et déterminer la longueur ayant à peu près le même diamètre que la prothèse
correcte. Couper la prothèse avec un instrument et qui permette un passage aisé des anneaux en
de chirurgie tranchant. NE PAS TIRER NI DÉCOLLER FEP. Si le tunnel tissulaire est trop étroit, les anneaux
L’ENVELOPPE EXTERNE RENFORCÉE D’UNE ZONE risquent de se détacher.
QUELCONQUE DE LA PROTHÈSE. SI L’ENVELOPPE 3. Pour éviter que les anneaux ne se détachent lors du
EXTERNE RENFORCÉE EST EFFILOCHÉE À L’UNE passage de la prothèse dans une incision, faire en
DES EXTRÉMITÉS DE LA PROTHÈSE, COUPER AVEC sorte qu’ils ne s’accrochent pas au bord de l’incision
SOIN CETTE SECTION DE LA PROTHÈSE AVEC UN ou au tunnellisateur.
INSTRUMENT CHIRURGICAL TRANCHANT. 4. RETRAIT DES ANNEAUX : Pour éviter d’endommager
7. À l'aide d’un tunnellisateur tel que le tunnellisateur la prothèse, NE PAS utiliser de lames chirurgicales
GORE®, créer un tunnel tissulaire ayant à peu près le ni d’instruments tranchants. Faire attention à ne
même diamètre que la prothèse. Un tunnel tissulaire pas endommager l’enveloppe renforcée se trouvant
trop large peut retarder ou diminuer l’attachement juste au-dessous du film mince supplémentaire
tissulaire et contribuer à la formation de séromes auquel sont attachés les anneaux. Après le retrait des
autour de la prothèse. anneaux, des portions du film mince supplémentaire
8. Les angles anastomotiques varient selon la procédure sont normalement visibles sur la prothèse et sur
vasculaire effectuée. L’utilisation d’un angle les anneaux retirés. SI L’ENVELOPPE RENFORCÉE
anastomotique approprié peut minimiser les tensions SEMBLE EFFILOCHÉE OU ENDOMMAGÉE, NE PAS
excessives qui sinon peuvent entraîner des ruptures UTILISER CE SEGMENT DE LA PROTHÈSE.
mécaniques de la prothèse, du vaisseau receveur et/ Pour retirer les anneaux se trouvant à l’extrémité
ou des lignes de suture. d’une section à anneaux ou avant de suturer :
9. N’utiliser que des fils monobrin non résorbables tels Maintenir fermement la prothèse d’une main gantée
que les sutures GORE‑TEX® d’une grosseur appropriée et avec l’autre main, saisir doucement un (des)
pour la nature de la reconstruction. Ne pas utiliser anneau(x) et le(s) soulever avec les doigts gantés
d’aiguille tranchante sur toute la circonférence de son ou avec un instrument atraumatique, puis le(s) faire
extrémité sous peine d’endommager la prothèse. glisser de l’extrémité de la prothèse.
10. Une hémorragie anastomotique excessive peut avoir Pour retirer les anneaux se trouvant à l’intérieur
lieu si une tension excessive est exercée sur les trous d’une section à anneaux ou après avoir suturé :
de suture et les allonge ou les déchire, si le rapport Maintenir fermement la prothèse d’une main gantée
de diamètre aiguille/suture est trop grand ou si des et avec l’autre main, détacher un (des) anneau(x) en
7le(s) saisissant doucement et en le(s) soulevant avec DEFINITIONS
un instrument atraumatique. Délicatement, couper
chaque anneau avec des ciseaux à bouts ronds et Utiliser avant le
décoller chaque anneau détaché.
5. Voir « CONTRE-INDICATIONS », Section II. B. ; Attention
« INFORMATIONS TECHNIQUES », Section V. F., G. et
Consulter le mode d’emploi
H. ; et « TECHNIQUES OPÉRATOIRES : TOUTES LES
CONFIGURATIONS DE PROTHÈSES VASCULAIRES 2
STERILIZE Ne pas restériliser
GORE® PROPATEN® », Section VII. A.
Ne pas réutiliser
D. TECHNIQUES OPÉRATOIRES ‑ PROTHÈSE VASCULAIRE
GORE® PROPATEN® À ANNEAUX INTÉGRÉS Numéro de référence
1. Les prothèses vasculaires GORE® PROPATEN® à
anneaux intégrés comprennent une prothèse Code du lot
vasculaire GORE‑TEX® en ePTFE, renforcée par un
support radial intégré en ePTFE situé dans la paroi de ATTENTION : Selon loi fédérale des États-Unis, ce dispositif ne
la prothèse. peut être vendu, distribué ou utilisé que par un médecin ou
2. Le support radial en ePTFE n'est PAS amovible. La sur prescription.
prothèse vasculaire GORE® PROPATEN® à anneaux
intégrés est un dispositif une pièce qui incorpore Stérile
une microstructure continue en ePTFE entre le
support radial et les sections sans support radial de la Stérilisé à l’oxyde d’éthylène
prothèse. Toute tentative de retrait du support radial
Ne pas utiliser si l’emballage est endommagé
endommagera la prothèse.
3. Les sections à support radial en ePTFE de la prothèse Conserver au sec
vasculaire GORE® PROPATEN® à anneaux intégrés
peuvent être incorporées dans l’anastomose. Le
Conserver dans un endroit frais
support radial intégré peut être coupé et cousu
par les techniques appropriées. Voir « TECHNIQUES AXL Axillo-bifémoral
OPÉRATOIRES : TOUTES LES CONFIGURATIONS DE
PROTHÈSES VASCULAIRES GORE® PROPATEN® », Diamètre
Section VII. A.
4. Lors de l’application des clamps, éviter tout Longueur de fibrille 25 microns (nominal)
endommagement mécanique ou déchirure de la
prothèse vasculaire GORE® PROPATEN® à anneaux Longueur de fibrille 5 microns (nominal), support radial
intégrés. Utiliser des clamps appropriés atraumatiques
ou recouverts d’une gaine protectrice (en caoutchouc, IR Anneaux intégrés
par exemple). Éviter les clampages répétés, toujours
au même endroit ou trop forts sur une section Longueur
quelconque de la prothèse.
5. Voir « INFORMATIONS TECHNIQUES », Section V. G. ; Fabricant
« Procédures de pontage coronarien » et
« TECHNIQUES OPÉRATOIRES : TOUTES LES Anneaux inamovibles
CONFIGURATIONS DE PROTHÈSES VASCULAIRES
GORE® PROPATEN® », Section VII. A. Anneaux amovibles
VIII. STÉRILITÉ Section avec anneaux
Les prothèses vasculaires GORE® PROPATEN® sont fournies Paroi standard
STÉRILES à moins que l’emballage n’ait été endommagé. La
méthode de stérilisation utilisée est indiquée sur la boîte. La Paroi fine
stérilité est maintenue jusqu’à la date de péremption (« À utiliser
avant le ») indiquée sur l’étiquette de la boîte.
IX. RESTÉRILISATION
NE PAS RESTÉRILISER LA PROTHÈSE VASCULAIRE
GORE® PROPATEN®.
RÉFÉRENCES
1. Ortel TL, Chong BH. New treatment options for heparin-
induced thrombocytopenia. Seminars in Hematology
1998; 35 (4): 26-34.
2. Almeida JI, Coats R, Liem TK, Silver D. Reduced morbidity
and mortality rates of heparin-induced thrombocytopenia.
Journal of Vascular Surgery 1998; 27 (2): 309-16.
3. Warkentin TE, Grienacher A, Koster A, Lincoff AM.
Treatment and prevention of heparin-induced
thrombocytopenia: American College of Chest Physicians
evidence-based clinical practice guidelines (8th edition).
Chest 2008;133:340S-380S.
4. Landry GJ, Moneta GL, Taylor Jr. LM, Porter JM.
Axillobifemoral bypass. Annals of Vascular Surgery
2001;14(3):296-305.
5. Taylor Jr. LM, Park TC, Edwards JM, Yeager RA,
McConnell DC, Moneta GA, Porter JM. Acute disruption
of polytetrafluoroethylene grafts adjacent to axillary
anastomoses: a complication of axillofemoral grafting.
Journal of Vascular Surgery 1994;20:520-528.
6. Bunt TJ, Moore W. Optimal proximal anastomosis /
tunnel for axillofemoral grafts. Journal of Vascular Surgery
1986;3:673-676.
8AQ3580-ML2
Manufacturer
W. L. Gore & Associates, Inc.
Flagstaff, Arizona 86004 • USA
Order Information: Tel.: 928.526.3030 • Tel.: 800.528.8763
Technical Information: Tel.: 928.779.2771 • Tel.: 800.437.8181
For international contact and additional product information,
visit www.goremedical.com
GORE®, GORE‑TEX®, ACUSEAL, PROPATEN®, and designs are trademarks of W. L. Gore & Associates.
CARMEDA® and CBAS® are trademarks of Carmeda AB Corp., a wholly owned subsidiary of W. L. Gore & Associates, Inc.
SURGICEL is a trademark of Johnson & Johnson, Inc.
BETADINE® is a trademark of Purdue Fredrick Company.
© 2001, 2005, 2006, 2009 - 2012 W. L. Gore & Associates, Inc.
Printed on recyclable paper JANUARY 2012Vous pouvez aussi lire