PERLES CLINIQUES POUR LE CONSULTANT EN PÉDIATRIE - Dre Chrisane Gagnon Dr Jean Turgeon - AWS
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous
PERLES CLINIQUES POUR LE CONSULTANT
EN PÉDIATRIE
Dre Chris)ane Gagnon
Dr Jean Turgeon
21 novembre 2018
LE RAISONNEMENT CLINIQUE
• Processus de pensée qui permet au clinicien de prendre des décisions appropriées
dans un contexte de résolu)on de problèmes de santé.
• Pour ce faire, le clinicien synthé)se l’informa)on obtenue dans une situa)on
clinique donnée, l’intègre avec ses connaissances et ses expériences antérieures et
les u)lise pour prendre des décisions diagnos)ques et de prise en charge
ÉLÉMENTS ESSENTIELS • Stratégies générales de résolu)on de problèmes • Bagage de connaissances spécifiques adaptées aux tâches cliniques
L’IMPORTANCE DES HYPOTHÈSES
• Tous les cliniciens génèrent des hypothèses très rapidement lorsqu’ils se trouvent
devant un problème clinique.
• Ce qui dis)ngue les experts des débutants, ce n’est pas le nombre ou la vitesse
d’appari)on des hypothèses, mais plutôt leur qualité et leur per)nence par rapport
à la situa)on.
GÉNÉRATION D’HYPOTHÈSES
• Processus analyBque: recherche délibérée et consciente d’hypothèses explica)ves.
Surtout lorsqu’on est face à une situa)on peu familière.
• Processus non-analyBques (automa)ques, inconscients): relèvent de la
reconnaissance d’un schéma (paQern recogni)on). Processus prévalent lorsqu’on
est familier avec une situa)on.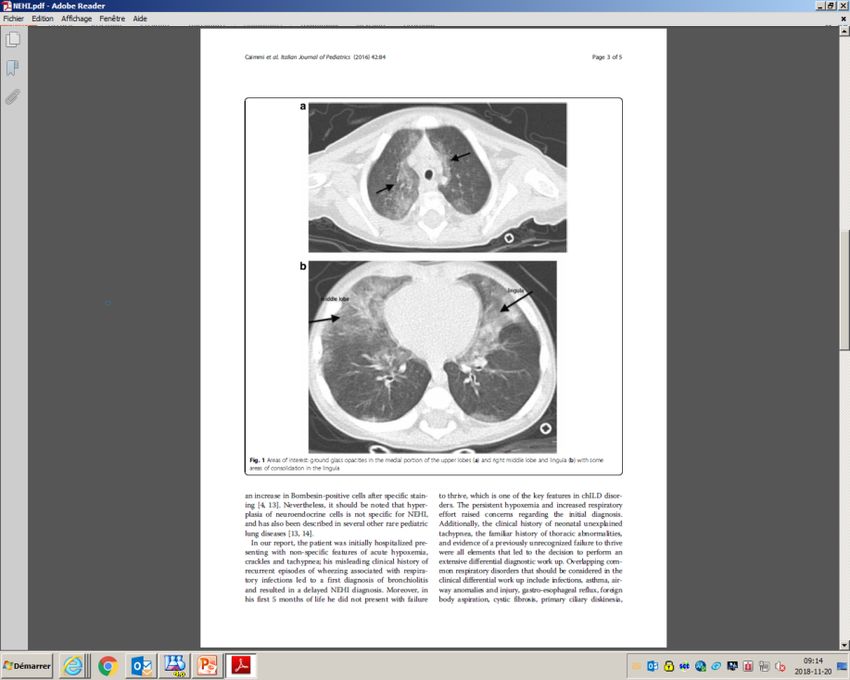
SCRIPTS DE MALADIE
• Un clinicien expérimenté mobilise très rapidement des connaissances faites de
mul)ples liens entre la maladie, ses signes, ses condi)ons d’appari)on, ses
caractéris)ques évolu)ves et ses op)ons d’inves)ga)on et de traitement.
• Ces connaissances organisées, les scripts, se développent grâce à l’exposi)on
clinique à de nombreux pa)ents.
• Plus on génère de scripts, plus on génère d’incer)tude
« On mesure l’intelligence d’un individu à la
quanBté d’incerBtudes qu’il est capable de
supporter »
Emmanuel Kant
PONDÉRATION DES SCRIPTS Ø Approche diagnos)que doit tenir compte de deux axes qu’il faut apprendre à conjuguer et à croiser: • Du diagnos)c le plus fréquent au plus rare • Du diagnos)c le plus grave au moins sévère

PATTERN RECOGNITION
• Most doctors follow familiar paQerns and rules, oWen improvising around those
rules. In their methods of working they are more like jazz musicians than scien)sts.
Richard Smith, editor, BMJ 2004;328:0.9
10
L’ART DU DIAGNOSTIC
azz
Il tousse toujours docteur… RGO?
PRÉSENTATION DU PETIT BONHOMME Garçon de 2 ans 4/12 Tousse depuis l’âge de 2 mois Essai IPP infructueux Vu en ORL œdème du larynx → IPP Revu tousse toujours, référé en gastro pour RGO réfractaire Boit bien, aucune irritabilité, pas d’infec)on, pas de sillement, pas d’essai de pompes CSI ou BACA, développement normal, pas d’étouffement en buvant Grossesse et accouchement sp Pas d’antécédent familial d’atopie, pas d’irritant iden)fié EP: suit sa courbe, SP, mais toux occasionnelle et grasse durant l’entrevue
SYMPTÔMES DE RGO
Rosen et al JPGN # Volume 66, Number 3, M
TABLE 1. Symptoms and signs that may be associated with gastro- 17 years old (28). In this study, there were no definiti
esophageal reflux disease in infants and children 0 to 18 years old positive test was defined so calculation of specificity
was not possible.
Symptoms Signs
General General Other Considerations for the Use of B
Discomfort/irritability
!
Dental erosion Imaging
Failure to Thrive Anemia
Feeding refusal Other studies, while not meeting inclusion c
Dystonic neck posturing shown that reflux events can be detected in as man
(Sandifer syndrome) children undergoing radiologic imaging, regardless o
Gastrointestinal Gastrointestinal As such, routine use of upper GI barium contra
Recurrent regurgitation with/ Esophagitis the evaluation of infants and children with GERD
without vomiting in the older child Esophageal stricture uncomplicated GERD, is not supported by literatur
Heartburn/chest painy Barrett esophagus practice.
Epigastric painy While the use of upper GI barium contrast to
Hematemesis negate a diagnosis of GERD in infants and children is n
Dysphagia/odynophagia by literature nor clinical practice, the test does carry so
Airway Airway the evaluation of infants and children with alarm signs
Wheezing Apnea spells with symptoms that are particularly intense or not r
Stridor Asthma traditional therapies in order to evaluate for anatomic ab
Cough Recurrent pneumonia The test can be used to evaluate for other condition
Hoarseness associated with aspiration mimic or predispose to GERD such as hiatal hernia,
Recurrent otitis media pyloric stenosis, duodenal web, duodenal stenosis,
esophageal narrowing, Schatzki’s ring, achalasia, esop
BRUE ¼ brief resolved unexplained event; GERD ¼ gastroesophageal ture, and esophageal extrinsic compression. One
reflux disease. important roles for barium imaging is in the evaluatio
!
If excessive irritability and pain is the single manifestation, it is unlikely who have had anti-reflux surgery who are sympt
to be related to GERD. persistent typical or atypical reflux symptoms, dysph
y
Typical symptoms of GERD in older children. barium imaging can be helpful to differentiate an
fundoplication with esophageal stasis from a slipp
fundoplication (35,36).
TABLE 2. ‘‘Red flag’’ symptoms and signs that suggest disorders other than gastroesophageal reflux disease
Symptoms and signs
Pediatric_Gastroesophageal_Reflux_Clinical.33.pdf
Remarks
General
Weight loss Suggesting a variety of conditions, including systemic infectionsL’EXAMEN ORL
THE JOURNAL OF PEDIATRICS • www.jpeds.com ORIGINAL
ARTICLES
The Edematous and Erythematous Airway Does Not Denote Pathologic
Gastroesophageal Reflux
Rachel Rosen, MD, MPH1, Paul D. Mitchell, MS2, Janine Amirault, BS1, Manali Amin, MD3, Karen Watters, MD4, and
Reza Rahbar, MD4
Objective To determine if the reflux finding score (RFS), a validated score for airway inflammation, correlates
with gastroesophageal reflux measured by multichannel intraluminal impedance (MII) testing, endoscopy, and quality
of life scores.
Study design We performed a prospective, cross-sectional cohort study of 77 children with chronic cough un-
dergoing direct laryngoscopy and bronchoscopy, esophagogastroduodenoscopy, and MII testing with pH (pH-MII)
between 2006 and 2011. Airway examinations were videotaped and reviewed by 3 blinded otolaryngologists each
of whom assigned RFS to the airways. RFS were compared with the results of reflux testing (endoscopy, MII, symptom
scores). An intraclass correlation coefficient was calculated for the degree of agreement between otolaryngolo-
gists’ RFS. Receiver operating characteristic curves were created to determine the sensitivity of the RFS. Spear-
man correlation was calculated between the RFS and reflux measurements by pH-MII.
J Pediatr. 2017 Apr;183:127-131
Results The mean ± SD RFS was 12 ± 4. There was no correlation between pH-MII variables and mean RFS
(|r| < 0.15). The concordance correlation coefficient for RFS between otolaryngologists was low (intraclass corre-CORRÉLATION SCORE ORL DE REFLUX ET RGO
THE JOURNAL OF PEDIATRICS • www.jpeds.com Volume 183
Junior: r = 0.01
Senior: r = 0.06
Midlevel: r - 0.11
Figure 2. Lack of correlation between RFS and total number of reflux events (open circle: junior otolaryngologist; solid circle:
midlevel otolaryngologist; star: senior otolaryngologist).
of 5 procedures as part of their diagnostic evaluation for our finding that there is a lack of relationship between the RFS
extraesophageal reflux disease. The results of our study suggest and reflux, acid suppression trials fail to consistently improve
that DLB has a low positive predictive value for diagnosing laryngeal findings; in a meta-analysis by Guo et al,14 the authors
GERD, and it should be removed from the list of diagnostic J Pediatr. 2017 Apr;183:127-131
found that the RFS did not predict PPI responsiveness; only
tests for extraesophageal reflux disease. 1 out of 4 studies showed a positive relationship between RFSCORRÉLATION SCORE ORL DE REFLUX ET RGO
Conclusions de l’étude:
• Le score visuel de l’examen ORL ne peut diagnos)quer un reflux
gastro-oesophagien pathologique
• On ne devrait pas de baser sur examen ORL pour prescrire un
traitement contre le reflux gastro-oesophagien
J Pediatr. 2017 Apr;183:127-131vided from this report can indeed be helpful in convincing
colleagues and families to temper the use of hypothermia for short-term outcomes of therapeutic hypothermia in preterm neonates 34-
35 weeks gestational age with hypoxic-ischemic encephalopathy. J Pediatr
preterm infants until randomized trials are conducted. ■ 2017;183:37-42.
6. Shankaran S, Laptook AR, Ehrenkranz RA, Tyson JE, McDonald SA,
Abbot R. Laptook, MD Donovan EF, et al. Whole-body hypothermia for neonates with hypoxic-
Neonatal Intensive Care Unit ischemic encephalopathy. N Engl J Med 2005;353:1574-84.
7. Walsh WF, Butler D, Schmidt JW. Report of a pilot study of cooling four
CONCLUSION DES ORLS
Women and Infants Hospital of Rhode Island
preterm infants 32-35 weeks gestation with HIE. J Neonatal Perinatal Med
Alpert Medical School 2015;8:47-51.
Brown University 8. Committee on Fetus and Newborn. Hypothermia and neonatal encepha-
Providence, Rhode Island lopathy. Pediatrics 2014;133:1146-50.
Questioning the Utility of Laryngoscopy in the Evaluation
of Pediatric Gastroesophageal Reflux
G
astroesophageal reflux disease (GERD) is a common endpoint of symptom and examination improvement as an al-
and well-known problem throughout medicine, and ternative to more invasive testing. Most of this work has been
its extraesophageal manifestations have been well- done in adults and extrapolated to the treatment of children.
documented. As the organ at the junction of In both populations, this evaluation is com-
the respiratory tract, the gastrointestinal tract, See related article, p 127 monly accomplished by office-based
• Les conclusions de l’étude sont bonnes
and the pharyngeal airway, the larynx is
uniquely at risk for exposure to the effects of gastric refluxate,
fiberoptic laryngoscopy. A general anes-
thetic with diagnostic laryngoscopy in the operating room, com-
• Ne pas généraliser à toutes les situa)ons cliniques
and is particularly susceptible to the effects of gastric contents.1,2
This clinical diagnosis is commonly known as laryngopha-
bined with 24-hour pH-impedance (pH-MII) probe, as
performed in the study by Rosen et al in this volume of The
• Ne pas prescrire les IPP comme des bonbons
ryngeal reflux disease (LPRD). A myriad of symptoms in the
pediatric population have been attributed to or exacerbated
Journal,3 to guide treatment decisions for non–life-threatening
symptoms attributed to reflux, is not usual practice. Such an
à tous les enfants qui toussent
by GERD and LPRD ranging from non–life-threatening symp-
toms that impact quality of life, such as chronic cough, globus
approach is more often reserved for children with life-
threatening or complex aerodigestive disorders refractory to
sensation, and dysphonia, to major aerodigestive problems such treatment or those undergoing complex airway surgery, in
as laryngomalacia, dysphagia, failure to thrive, infant apnea, whom reflux is a known contributor to complications in sur-
and laryngotracheal stenosis. Otolaryngologists combine gical intervention of the upper airway.4-6
symptom presentation with diagnostic laryngoscopy to diag- Empiric proton pump inhibitor therapy and its unknown
nose LPRD and may recommend empiric therapy with an long-term side effect profile, combined with the high cost of
GERD Gastroesophageal reflux disease
J Pediatr. 2017 Apr;183:9-11
The authors declare no conflicts of interest.
LPRD Laryngopharyngeal reflux disease
pH-MII pH-Impedance 0022-3476/$ - see front matter. © 2017 Elsevier Inc. All rights reserved.
http://dx.doi.org10.1016/j.jpeds.2017.01.035INVESTIGATION DES SYMPTÔMES
EXTRAOESOPHAGIENS DE RGO
• Test thérapeu)que aux IPP n’apporte rien et n’est pas
recommandé
o Sauf si manifesta)ons claires de RGO pathologique,
ou examen diagnos)c posi)f
• Vidéofluoroscopie / repas baryté
• Impédance pH-métrie
• Endoscopie oesophagienne:
o Pour exclure les mascaradeurs
o À faire sans traitement
Pediatric_Gastroesophageal_Reflux_Clinical.33.pdfLA FIN DE L’HISTOIRE
• Impédance pH-métrie
o Néga)ve: aucun reflux, acide ou non acide
• Retour au diagnos)c différen)el de toux chronique:
o Rayon X du poumon et des )ssus mous du cou
o Test de suda)on :
Fait 2 x valeurs intermédiaires 36 et 40LA FIN DE L’HISTOIRE
• Vu en pneumologie:
o Suspicion de FKP
o Ciprofloxacin 2 semaines
o Culture de gorge posi)ve pour Pseudomonas
aeruginosa
o Salin hypertonique en inhala)on bid
o DDx: FKP, cils immobiles, bronchiectasieLES POINTS RETENUS • Les trouvailles à l’examen ORL du larynx ne peuvent permeQre de diagnos)quer un RGO et ne peuvent déclencher un traitement contre le RGO • Revenir au diagnos)c différen)el de la toux chronique • Inves)guer avant de traiter si le rgo n’est évoqué que par des manifesta)ons respiratoires
Un garçon de presque 4 ans est référé pour lombalgie et boiterie
PRÉSENTATION CLINIQUE
• Syndrome d’allure viral il y a 5 jours avec IVRS, céphalée, perte d’appé)t sans
fièvre
• Quelques jours plus tard, se plaint de douleurs aux OGE, sans symptômes
urinaires
• Appari)on progressive d’une douleur lombaire et boiterie gauche sans fièvre
• À l’examen physique, l’enfant est irritable et semble très souffrant,
par)culièrement lorsqu’on lui touche la région lombaire.
• SV normaux, pas de fièvre
• Tes)cule droit semble augmenté de volume, douloureux avec une légère
rougeur du scrotum
• Le MIG est en rota)on externe, la flexion des hanches est douloureuse et il n’y a
pas de signes d’arthriteINVESTIGATION INITIALE
• Formule sanguine complète normale
• CRP à 5,7
• Créa)nine normale
• Albumine à 32
• ALT et CK normaux
• Écho tes)culaire compa)ble avec une épididymite
• Écho abdominal normal sauf pour la présence d’un peu de liquide libre pelvien
• Écho de surface lombaire montre un aspect infiltré et hétérogène de la graisse
sous-cutanée
• Ct-Scan montre en plus un rehaussement du fascia superficiel des muscles para-
lombairesIMPRESSIONS INITIALES • Lombalgie sévère avec image radiologique de fasciite lombaire • Boiterie • Épididymite gauche • Hypothèse de tableau viral demeure la plus probable • Couverture empirique avec cefotaxime et clindamycine
ÉVOLUTION
• L’enfant demeure très souffrant, ne peut se mobiliser et est par)ellement
soulagé par la morphine
• Appari)on d’un œdème temporal gauche
• Au deuxième jour d’hospitalisa)on quelques pétéchies aux membres supérieurs
• Le lendemain les pétéchies progressent aux membres inférieurs
• Au quatrième jour appari)on d’une ecchymose derrière le genou gauche avec
douleur ar)culaireDIAGNOSTIC FINAL
Purpura d’Henoch-Schönlein
Pt revu une semaine plus tard: douleur
lombaire disparue, rash typique aux MI et
douleurs ar)culaires migratoires aux genoux
et chevilles
Dosage IgA à 2,05 (0,3 – 1,50)PURPURA D’HENOCH-SCHÖNLEIN
• Le rash typique comme présenta)on ini)ale survient chez environ 75% des cas.
• Dans de très rares cas, il peut même être absent…
• Le dx de PHS doit donc être considéré dans le diagnos)c différen)el chez un
pa)ent présentant des douleurs abdominales ou musculo-squele~ques
inexpliquées.Il ne fait plus rien docteur… DÉPRESSION CATATONIQUE ?
PRÉSENTATION DE CET ADOLESCENT • Garçon de 17 ans, né au Québec, parents d’origine pakistanaise, consanguinité • J1 première consulta)on pour insomnie, référé en psychiatrie pour insomnie, blocage de la pensée et isolement social; Rx : Olanzapine • J22 consulte urgence pour insomnie sévère, ne fait rien, diminu)on des résultats scolaires; EP normal, ralen)ssement cogni)f, bilan sanguin ALT 90 ré olanzapine Diagnos)c psychose, référé à hôpital psychiatrique • Trouble dépressif majeur épisode isolé, modéré à sévère sans caractéris)que psycho)que, ni élément de dangerosité Rx : fluoxé)ne, quiétapine
PRÉSENTATION DE CET ADOLESCENT
• J29 mère reconsulte, détérioré sous médica)on, ne boit
plus, ne s’alimente plus:
Insomnie, mu)sme, confusion, anxiété
EP : catatonique, raideur diffuse
test challenge au benzodiazépine à l’urgence
Hospitalisa)onADO CATATONIQUE
• Vu en psy: confusion mentale liée à problème organique ou
dépression majeure
• EEG normal
• CT Scan cérébral: normal
• IRM cérébrale: normale
• Labos:
o ALT 172 diminuent ad 82 spontanément en quelques jours, GGT
76
o Phosphatase alcaline, bili, protéines, albumines, INR, amylase,
CK, FSC, ferri)ne : Normales
• Entre temps va un peu mieux, veut retourner à la maisonADO CATATONIQUE
• Céruloplasmine 0,09 (N>2)
• Dosage du cuivre urinaire: en aQente
• Échographie abdominale:
Foie de texture neQement anormale d'échogénicité accrue et d'une texture
diffusément micronodulaire qui est dans le contexte clinique men)onné doit
faire penser à un foie cirrho)que avec nodules de régénéra)ons, ce qui pourrait
naturellement être confirmé par des biopsies hépa)ques.
Dx: Maladie de WilsonMALADIE DE WILSON
• 1/30 000
• Début à tous les âges
• Age médian de présenta)on 17 ans
• Fréquence de la présenta)on ini)ale grands ados:
neurologique > asymptoma)que > hépa)que
• Présenta)on neurologique: changement de comportement, de personnalité,
anxiété et dépression
• ALT peu élevés dans la présenta)on neurologique
• Étude familiale nécessaire: transmission autosomale dominante
Can J Gastroenterol Vol 26 No 6 June 2012CUIVRE ALIMENTAIRE
Hepatic (n=13) 4 (3
Neurological 8 (5
(n=15)
Hepatic and 3 (5
neurological
WILSON, PRÉSENTATION NEUROLOGIQUE (n=6)
Total (n=48) 23 (
Treatment at review
Asymptomatic 1(
(n=14)
Hepatic (n=13) 3 (2
Neurological 3 (2
(n=15)
Hepatic and 1 (1
neurological
(n=6)
Total (n=48) 8 (1
Data presented as n (%
seven on a benzodia
typical antipsychotic
Latest laboratory va
At the time of t
Figure 2) Presenting hepatic (A) and neurological symptoms (B) for (Supplementary Tab
patients who had hepatic and mixed (n=20), and neurological and mixed treatment was 10.1 y
(n=21) presentations, respectively with access to follow
Can J Gastroenterol Vol 26 No 6exclusively
June 2012 on zinc
Median urinary coppMoores et al
WILSON, PRÉSENTATION HÉPATIQUE
TABLE 3
Initial treatmen
review accordi
Presentation, n
Initial treatment
Asymptomatic
(n=14)
Hepatic (n=13)
Neurological
(n=15)
Hepatic and
neurological
(n=6)
Total (n=48) 2
Treatment at revie
Asymptomatic
(n=14)
Can J Gastroenterol Vol 26 No 6 June 2012
Hepatic (n=13)
NeurologicalWILSON DIAGNOSTIC
me 66, Number 2, February 2018 Wilson’s Disease
JPGN " Volume 66, Number 2, February 2018 Wilson’s Disease in Children
• Clinical evalua!on for hepato-splenomegaly,
• Clinical evalua!on ascites,
for hepato-splenomegaly, ascites, K-FK-F
ring ring
JPGN " • Liver tests:
Volume 66, Number •ALT/AST,
2, February bilirubin
2018
Liver tests: ALT/AST, total/direct,
bilirubin total/direct,INR, AP
INR, AP Wilson’s Disease in Children
I step
I step • Biochemical tests of copper metabolism: serum ceruloplasmin, 24h urinary copper excre!on
• Biochemical tests of copper metabolism: serum ceruloplasmin, 24h urinary copper excre!on
• Clinical evalua!on for hepato-splenomegaly, ascites, K-F ring
• Molecular
• Liver tes!ng bilirubin
tests: ALT/AST, (commontotal/direct,
muta!ons, whole
INR, gene
AP sequencing)
II step
•I Molecular tes!ng (common muta!ons, whole gene sequencing)
step • Biochemical tests of copper metabolism: serum ceruloplasmin, 24h urinary copper excre!on
II step
• Liver copper (if molecular tes!ng inclonclusive or not available)
• Molecular tes!ng (common muta!ons, whole gene sequencing)
III step
II step
• Liver copper (if score
Ferenci molecular
calculatedtes!ng inclonclusive
at each step; orconfirm
4 points or more not available)
diagnosis- once diagnosis is confirmed
III step further tes!ng is not required to start therapy
FIGURE 1. Diagnostic approach• to
Liver copperdisease.
Wilson’s (if molecular
ALT ¼ tes!ng
alanineinclonclusive or not AP
aminotransferase; available)
¼ alkaline phosphatase; AST ¼ aspartate aminotransferase.
III step
Ferenci score calculated at each step; 4 points or more confirm diagnosis- once diagnosis is confirmed
asymptomatic patients (68,70).
further Furthernot
tes!ng studies are needed to evaluate and the monitoring of compliance and early detection of
Ferenciisscore required
calculated atto start
each step;therapy
4 points or more confirm diagnosis- once diagnosis is confirmed
further tes!ng is not required to start therapy complications. Prognosis is excellent provided compliance to ther-
its diagnostic accuracy in children with liver disease.
Recommendations of the ESPGHAN Hepatology Committee apy is adequate.
agnostic
FIGURE
approach
are1.shown to
in Table
Diagnostic
Wilson’s
1.
approach
disease. ALT ¼ alanine aminotransferase; AP ¼ alkaline phosphatase; AST ¼ aspartate amin
to Wilson’s disease. ALT ¼ alanine aminotransferase; AP ¼ alkaline phosphatase; AST ¼ aspartate aminotransferase.
The diagnostic approach is illustrated in Figure 1. Treatment Options
D-penicillamine was introduced in 1956, and remains the
c patients
asymptomatic (68,70). Further
patients (68,70).studies are needed
Further studies to evaluate
are needed to evaluate and
and the
the
standard monitoring
monitoring
treatment for WD. of compliance
ofIt chelates
compliancecopperand earlyand
and favors early of d
itsdetection
urinary
its The Importance
diagnostic
accuracy in accuracy
children in of Family
children
with with
liver Screening
liver
disease. disease. for Wilson’s complications.
complications. JPGND-penicillamine
Prognosis is
Prognosis
excretion. Experimentally, 2018;66:
excellent
is 334–344
provided
excellent compliance
also provided
has a copper to ther-
compli
Disease
Recommendations of the ESPGHAN Hepatology Committee apy is adequate.
‘‘detoxifying’’ effect by inducing the endogenous hepatic metal-
mmendations of the
are shown in Table 1. ESPGHAN Hepatology Committee apy is adequate.
lothionein, a cytosolic metal-binding protein, which sequestersSCORE DE FERENCI
Therapeutic Advances in Psychopharmacology 8(7)
Table 2. The scoring system (Ferenci score) for the diagnosis of Wilson’s disease developed at the 8th
International Meeting on Wilson’s Disease and Menkes Diseases, Leipzig 2002.
K–F rings Present (2 points) Absent (0 points)
Neuropsychiatric Yes (2 points) No (0 points)
symptoms suggest WD
(or typical brain MRI)
Coombs negative Yes (1 point) No (0 points)
hemolytic anemia
24 h urinary copper Normal (0 points) 1–2 × ULN (1 point) >2 × ULN, or normal,
excretion (in the but >5 × ULN after
absence of acute challenge with 2 × 0.5
hepatitis) g D-penicillamine (2
points)
Liver copper Normal (−1 point) 5 × ULN (2 points)
quantitative
Rhodanine-positive Absent (0 points) Present (1 point)
hepatocytes (only
in case of lack of
Cu quantitative
assessment)
Serum ceruloplasmin Normal (0 points) 10–20 mg/dL (1 point) 20 mg/dL)
Mutation analysis Disease causing Disease causing No mutation detected (0
mutations on both mutations on one points)
chromosomes (4 points) chromosome (1 point)
Assessment of the WD diagnosis score:
⩾4 points: diagnosis of WD highly likely.
2–3 points: diagnosis of WD probable, more investigations needed.
0–1 point: diagnosis of WD unlikely.
MRI, magnetic resonance imaging; ULN, upper limit of normal.
Therapeu)c Advances in Psychopharmacology 8(7) · March 2018RECOMMANDATIONS ESPGHAN
1 WD should be considered in the differen)al diagnosis of children older than 1
year presen)ng with any sign of liver disease ranging from asymptoma)cally
increased serum transaminases to cirrhosis with hepatosplenomegaly and
ascites or ALF. Grade 1A (level of agreement: 86%)
2 WD should be ruled out in any teenager with unexplained cogni)ve,
psychiatric, or movement disorder. Grade 1A (96%)
3 Diagnos)c tes)ng for WD in suspected pa)ents should include liver func)on
tests (serum transaminases, conjugated and total bilirubin; alkaline
phosphatase and prothrombin )me/INR), serum ceruloplasmin, and 24-hour
urinary copper. Grade 1A (96%)
4 The Ferenci scoring system should be applied to children for diagnosis of WD.
Muta)on analysis of the ATPB7 gene may facilitate the diagnosis. Grade 1A
(91%)
JPGN 2018;66: 334–344RECOMMANDATIONS ESPGHAN
1 La maladie de Wilson doit faire par)e du diagnos)c différen)el de tout enfant
de plus d’un an présentant n’importe quel signe de maladie hépa)que: de la
découverte asymptoma)que de transaminases élevées à la cirrhose avec
hépatosplénomégalie, ascite et/ou insuffisance hépa)que aigue (Niveau 1A,
accord 86%)
2 La maladie de Wilson devrait éliminée chez tout adolescent avec un trouble
inexpliqué cogni)f, psychiatrique ou du mouvement (Niveau 1A, accord 96%)
3 Les tests diagnos)cs des pa)ents chez qui on suspecte une maladie de Wilson
devraient inclure des fonc)ons hépa)ques (transaminases, bili totale et directe,
phosphatase alcaline et INR), céruloplasmine sérique, cuivre urinaire sur
collecte de 24h (Niveau 1A, 96%)
4 Le score de Firenci devrait être calculé chez les enfants pour le diagnos)c de
la maladie de Wilson. La recherche de la muta)on du gène ATPB7 peut faciliter
le diagnos)c
Traduc)on libre de JPGN 2018;66: 334–344ADO CATATONIQUE
LA FIN DE L’HISTOIRE
• Transfert en gastroentérologie pédiatrique:
o Cuivre urinaire très augmenté
o Biopsie hépa)que J 35: fibrose et stéatose
o Traité avec du zinc
o Test géné)que:
Pa)ent porteur de la muta)on ATPB7
Frère aussi, asymptoma)que
• Hospitalisa)on 6 mois plus tard en psychiatrie pour trouble maniaque
o Bipolaire primaire ou secondaire à maladie de Wilson?LES POINTS RETENUS • La maladie de Wilson peut se présenter uniquement avec des symptômes neuro-psychiatriques chez l’adolescent • Les fonc)ons hépa)ques et le dosage de la céruloplasmine sont les premiers tests à faire pour l’éliminer
Un garçon de 5 ans est référé pour une arthrite sep)que de la hanche
PRÉSENTATION CLINIQUE
• Un garçon de 5 ans préalablement en bonne santé est admis pour boiterie
intermiQente depuis 3 semaines avec fièvre objec)vée mais inconstante
• À l’examen ini)al, l’enfant est en BEG, T à 38,1 buccal
• L’examen locomoteur révèle une légère boiterie de la jambe gauche avec
douleur élicitée lors de mise en tension de la hanche
• Le reste de l’examen physique est en)èrement normal
• FSC normale (leuco à 7.98, Hb à 112, pt à 337)
• VS à 51
• CRP à 52,3SUITE D’INVESTIGATION ET ÉVOLUTION
• Rx bassin et fémurs normaux
• Écho de la hanche gauche montre la présence d’un épanchement ar)culaire
• Scin)graphie osseuse montre une légère capta)on de l’épine iliaque inférieure
gauche (ostéomyélite?) de même qu’une légère capta)on diaphysaire des
fémurs (plus marquée à gauche) s’étendant sur 7 à 8 cm orientant davantage
vers un processus trauma)que qu’infec)eux
• Traitement avec Céfazolin IV pour infec)on ostéo-ar)culaire très probable
(Kingella kingae ?)
• Le lendemain l’enfant va beaucoup mieux, mise en charge et amplitudes de
mouvement sont normaux.
• L’enfant s’est cependant plaint la nuit suivante d’une douleur exquise à la jambe
droite, auto-résolu)veIRM HANCHES ET MEMBRES INFÉRIEURS
• AQeinte mul)focale qui touche les diaphyses et les métaphyses des fémurs,
crêtes iliaques, ailes iliaques, régions supra-acétabulaires, rameaux pubiens,
sacrum et rachis…
• Compa)ble avec métastases ou processus proliféra)fDIAGNOSTIC FINAL Leucémie lymphoblasBque aigüe
POURTANT TOUS SES BILANS DE BASE SONT NORMAUX! • Formules sanguines incluant fro~s normal • Acide urique, LDH normaux • Rx pulmonaire normal • Échographie abdominale normale
LLA: PRÉSENTATION CLASSIQUE • Hépatomégalie • splénomégalie • Lymphadénopathie • Fièvre inexpliquée • Pâleur • Ecchymoses ou saignements • Douleurs musculosquele~ques
LLA: AUTRES MODES DE PRÉSENTATION
• Symptômes neurologiques (HTIC)
• AQeinte tes)culaire
• Symptômes compressifs d’une masse médias)nale (syndrome veine cave
supérieure, douleurs thoraciques, dyspnée, toux, stridor, wheezing, dysphagie)Rhabdomyolyse: soluté pour la nuit svp! OK…?
ADOLESCENT AVEC RHABDOMYOLYSE
• Appel de la résidente en médecine interne pour adolescent de 17 ans avec
CK augmentées suite à anesthésie générale pour travaux dentaires.
Avait déjà subi anesthésie prolongée sans problème l’année dernière.
• Asperger, inves)gué pour retard moteur en bas âge, pas de consanguinité,
origine Ukrainienne, famille juive ashkenase
• Labos:
CK 10 000
Myoglobine 1924
Créa)nine 79
Calcium 0,89
Phosphore 0,36
Magnésium 0,31RHABDOMY0LYSE
Quelle que soit l’é)ologie:
Perte de l’intégrité de la membrane musculaire →
Éléva)on du sodium et du calcium intracellulaire → mort
cellulaire →
Relâchement dans le plasma de composants intracellulaire:
CK, myoglobine…
→ Complica)ons rénales
Préven)on: hydrata)on 2-3 ml/kg/h
Clinical Decisions in Pediatric Nephrology, Springer 2008
American journal of emergency medecine 2005, 23, 1-7LE NON-DIT
• Anesthésie interrompue ré CO2 expiré augmenté subitement
de 40 à 100, avec augmenta)on de la TA rapide de 80/40 à
140/80
• Température reste toujours normale
• Diagnos)c de l’anesthésiste:
Hyperthermie maligne
• Rx: Dantrolène IV stat et transfert en milieu hospitalier
• Antécédents familiaux:
Oncle maternel décédé durant une anesthésie à 14 ansHTTPS://WWW.MHAUS.ORG/
CONSULTATIONS • Anesthésie • Néphrologie • Neurologie
HYPERTHERMIE MALIGNE
• Incidence: pédiatrique 1/15 000 > adulte1/40 000
• Surtout, mais pas seulement, chez les jeunes hommes..
• 50% des pa)ents ont déjà eu une anesthésie à un agent précipitant
sans problème
• Précipité par les gaz anesthésiants, et la succinylcholine
• Signes précoces: augmenta)on CO2 expiré, tachycardie,
rigidité musculaire et hyperthermie
• Complica)ons sévères si dantrolène retardé ou omis
• Géné)que: muta)on du récepteur ryanodine (Ryr1)
Morgan & Mikhails’s Clinical Anesthesiology, 6th edi)on, Lange, 2018HYPERTHERMIE MALIGNE LA FIN DE L’HISTOIRE • Labos
ÉVOLUTION CK
90000
80000
70000
60000
50000
Normale
40000
CK Pa)ent
30000
20000
10000
0
1 2 3 4 5 6ÉVOLUTION MYOGLOBINE
2500
2000
1500
Normale
1000 Myoglobine Pt
500
0
2 3 4 5HYPERTHERMIE MALIGNE LA FIN DE L’HISTOIRE • CK ad 78 000 en 24h, créa)nine maintenue avec soluté • Soluté jusqu’à CK < 5000 • Bracelet Medic Alert® suggéré au départ de l’hôpital • Aver)r toute la famille du problème • Retour des CK à la normale en 2 semaines • EMG néga)f • Muta)on Ryr1 fréquente de l’Europe de l’Est retrouvée chez le garçon • Référé en géné)que adulte
LES POINTS RETENUS • Lors d’un épisode de rhabdomyolyse la créa)nine ini)ale est un facteur pronos)c important • Le soluté est nécessaire jusqu’à ce que les CK < 5000 • Le pa)ent avec hyperthermie maligne est souvent normothermique • Dans l’hyperthermie maligne il faut exclure les causes musculaires possiblement associées
Tachypnée persistante chez un garçon de 4 mois
PRÉSENTATION CLINIQUE
• Garçon de 4 mois, né à terme, poids 3,525, AVS, aucune complica)on néonatale
• Tachypnée et )rage remarqués vers 3 mois de vie
• Première consulta)on, Rx pulmonaire démontre de légères opacités linéaires
lobe inférieur gauche d’allure mécanique (atélectasie) et un peu de
péribronchite
• Essai tx avec amoxil: aucune améliora)on
• Essai avec prévacid car étouffements aux boires: améliore étouffements mais
tachypnée persiste
• Finalement admis pour suite d’inves)ga)on, d’autant plus qu’il commençait à
avoir un ralen)ssement pondéral malgré apports inchangés
• Examen physique normal sauf pour tachypnée fluctuante avec RR de 45-60/min,
)rage intercostal et quelques crépitants inspiratoires. Satura)on à l’éveil et à
AA est de 95%SUITE ET INVESTIGATION • FSC et biochimie incluant gaz capillaire normaux • Test à la sueur normal • Recherches microbiologiques (PCR viral, bactérien, chlamydia) néga)ves • Bilan immunologique normal • TSH normal • Écho cardiaque normal • Scopie ORL normale • Étude de déglu))on normale • Oxymétrie nocturne à AA anormale • Ph-métrie sans tx anormale (Ph < 4 sur 8% du temps)
ÉVOLUTION • Support nutri)onnel avec TNG pour raQrapage pondéral • Tx empirique avec azythromycine • Oxygène en permanence à 0,6 l/min
CT-SCAN THORACIQUE
• Aspect en verre dépoli symétrique touchant les segments postérieurs et apicaux
des deux lobes supérieurs, de même que le lobe moyen et la lingula, le tout
typique d’un…NEHI
NEUROENDOCRINE CELL HYPERPLASIA OF
INFANCY
• Maladie rare décrite en 2005
• Proliféra)on de cellules neuroendocriniennes dans les voies aériennes distales
(infiltrat inters))el)
• É)ologie inconnue
• Présenta)on insidieuse chez un nourrisson au préalable normal dans les premiers
mois de vie de tachypnée et de )rage
• Souvent aQribué ou mis en évidence lors d’une IVRS
• Souvent aQribué au RGO et micro-aspira)ons (qui est très souvent associé lorsque
recherché)
• Peu de toux
• Retard pondéral fréquent
• Hypoxémie devient invariable mais n’est pas toujours présente au début
• Outre la tachypnée et le )rage, on entend souvent des crépitants inspiratoires à
l’ausculta)onDIAGNOSTIC DIFFÉRENTIEL • Infec)ons aigues ou chroniques • Asthme • Immunodéficience • Dyskinésie ciliaire • Fibrose kys)que • Cardiopathie • Hypothyroïdie (brain-lung-thyroid syndrome par muta)on NKX2.1) • Pneumopathies inters))elles
CT-SCAN
ÉVOLUTION • Support en oxygène à moyen long terme • Support nutri)onnel • Tx du RGO si présent • Généralement bon pronos)c
EN CONCLUSION Démontrer que l’art de la médecine repose davantage sur une judicieuse ges)on de l’incer)tude que sur des connaissances scien)fiques sta)ques Se sensibiliser au fait que même si la médecine n’est pas une science exacte, son applica)on nécessite rigueur et précision Encourager à réviser au fil du temps notre liste personnelle de diagnos)cs qu’on ne veut pas manquer Reconnaître qu’en médecine on n’aQeint jamais une « zone de confort » et qu’il faut constamment demeurer à l’affut!
Merci!
Vous pouvez aussi lire

















































