REVUE DE L'ANNÉE EN MÉDECINE VASCULAIRE - Le sommet à votre portée
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous
07/05/2019
REVUE DE L’ANNÉE
EN MÉDECINE VASCULAIRE
VINCENT BERGERON MD FRCPC
7 mai 2019
PLAN
■ Lipides
– REDUCE-IT Lignes directrices américaines 2018
traitement de l’hypercholestérolémie
– ODYSSEY OUTCOME
■ Anti-plaquettaires
Lignes directrices américaines 2019
– ASCEND prévention primaire
■ AODs
– LIGNES DIRECTRICES CANADIENNES CAT
– AVERT
– CASSINI
– AUGUSTUS Mise à jour guide clinique sur la FA
– MANAGE
■ Diabète
– DECLARE-TIMI 58
■ Sous-étude PAD ACC mars 2019
1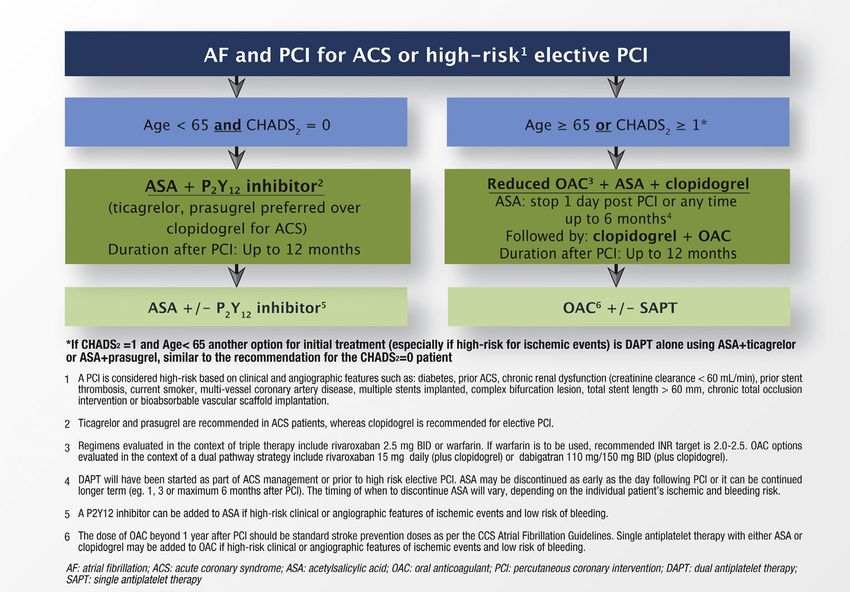
07/05/2019
REDUCE-IT
*
1,7 mmol/L +/- 10% (1,5 mmol/L)
2 mmol/L après répartition de
NEJM 2019;380:11-22 60% population
ICOSAPENT ETHYL vs HUILE VÉGÉTALE
■ Supériorité, multicentrique, internationale, contrôlée, double aveugle, répartition
aléatoire, 8,000 patients entre novembre 2011 et août 2016
■ Prévention secondaire et primaire (max 30%)
– * TG 1,7 à 5,6 mmol/L et C-LDL 1 à 2,6 mmol/L sous statine x 4 semaines et
– 45 ans et maladie CV établie ou
– Hommes >55 ans ou femmes >65 ans diabétiques ou
– Diabétiques >50 ans avec facteur de risque additionnel:
■ Tabac, HTA, HS-CRP, C-HDL bas, IRC, rétinopathie, MAU ou ITH abaissé
■ Exclusion: défaillance sévère, maladie hépatique sévère, A1c > 10%, PCI prévue,
pancréatite
■ Amarin Pharma: toutes les étapes de la conduite de l’étude
REDUCE-IT – paramètres d’évaluation
NEJM 2019;380:11-22
■ Critère combiné primaire:
– Mortalité cardiovasculaire
– Infarctus myocardique non fatal
– AVC non fatal
– Revascularisation coronarienne
– Angine instable
■ Critère secondaire principal: MACE traditionnel
■ Critères secondaires
2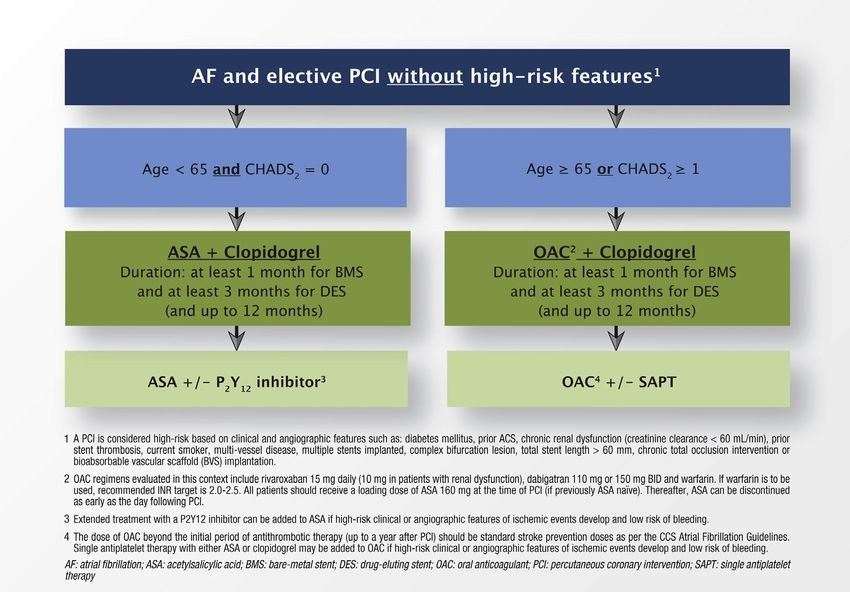
07/05/2019
REDUCE-IT – population
NEJM 2019;380:11-22
Âge médian 64 ans
Femmes 29%
IMC 30,8 kg/m2
TG médian 2,44 mmol/L
C-LDL médian 1,91 mmol/L
C-HDL médian 1,03 mmol/L
Caucasiens 90%
Prévention secondaire 71%
Diabète 58%
REDUCE-IT – résultats
NEJM 2019;380:11-22
n-3 placebo p
Efficacité primaire 17,2% 22%
07/05/2019
REDUCE-IT – effets indésirables
NEJM 2019;380:11-22
n-3 placebo p
Fibrillation auriculaire 5,3% 3,9% Significatif
Hospitalisation pour FA ou flutter 3,1% 2,1% 0,004
Œdème périphérique 6,5% 5,0% Significatif
Saignements sérieux 2,7% 2,1% 0,06
ACCEPTED MANUSCRIPT
PT
RI
U SC
JACC mars 2019
AN
M
4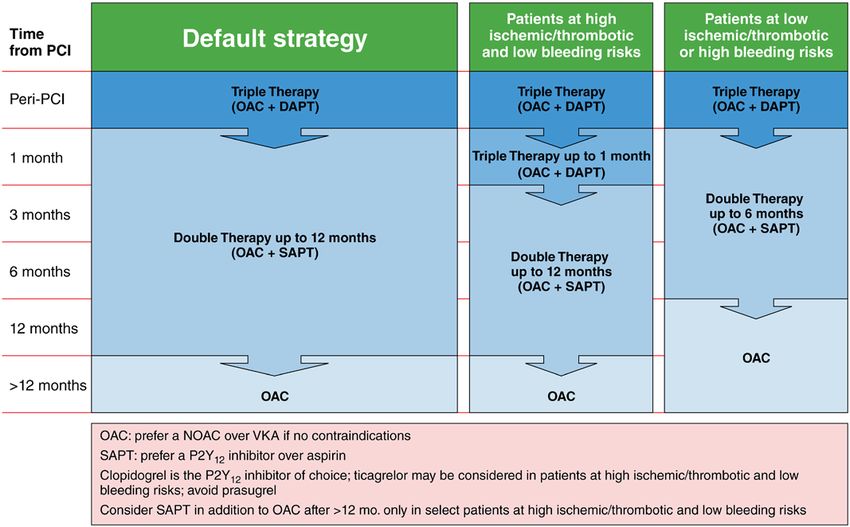
07/05/2019
Grundy SM, et al.
2018 Cholesterol Clinical Practice Guidelines
REDUCE-IT – conclusion
†The term Hispanics/Latinos in the United States characterizes a diverse population group. This includes white,
black, and Native American races. Their ancestry goes from Europe to America, including among these, individuals
NEJM
from the 2019;380:11-22
Caribbean, Mexico, and Central and South America.
ASCVD indicates atherosclerotic cardiovascular disease; BP, blood pressure; CAC, coronary artery calcium; CAD,
coronary artery disease; CK, creatine kinase; CVD, cardiovascular disease; DASH, Dietary Approaches to Stop
Hypertension; DM, type 2 diabetes mellitus; FDA, U.S. Food and Drug Administration; HDL-C, high-density lipoprotein
■ Premier succès dans le traitement du risque résiduel lié à l’hypertriglycéridémie
cholesterol; LDL-C, low-density lipoprotein cholesterol; MESA, Multi-Ethnic Study of Atherosclerosis; MetS,
■ Données
metabolic syndrome; reproductibles?
and PCE, pooled cohort equations.
■ Spécifique à la formulation utilisée?
■ Hypertriglyceridemia
4.5.2. Effet relié à la dose?
■ Mécanisme d’action?
Recommendations for Hypertriglyceridemia
– La
Referenced diminution
studies 18% de
that support triglycéridémieare
recommendations n’explique pas in
summarized le Online
bénéfice
Data Supplements 31
– Effet indésirable du placebo? and 32.
COR LOE Recommendations
■ Effets secondaires indésirables: fibrillation auriculaire
1. In adults 20 years of age or older with moderate hypertriglyceridemia
■ « Trop beau pour (fasting
être vrai?
or »nonfasting triglycerides 175 to 499 mg/dL [1.9 to 5.6 mmol/L]),
clinicians should address and treat lifestyle factors (obesity and metabolic
I B-NR
syndrome), secondary factors (diabetes mellitus, chronic liver or kidney
disease and/or nephrotic syndrome, hypothyroidism), and medications
that increase triglycerides (S4.5.2-1).
2. In adults 40 to 75 years of age with moderate or severe
hypertriglyceridemia and ASCVD risk of 7.5% or higher, it is reasonable to
Downloaded from http://ahajournals.org by on November 26, 2018
reevaluate ASCVD risk after lifestyle and secondary factors are addressed
IIa B-R
and to consider a persistently elevated triglyceride level as a factor favoring
initiation or intensification of statin therapy (see Section 4.4.2.) (S4.5.2-2–
S4.5.2-6).
Lignes directrices américaines
3. In adults 40 to 75 years of age with severe hypertriglyceridemia (fasting
triglycerides ≥500 mg/dL [≥5.6 mmol/L]) and ASCVD risk of 7.5% or higher,
IIa
novembreB-R
2018
it is reasonable to address reversible causes of high triglyceride and to
initiate statin therapy (S4.5.2-3–S4.5.2-5, S4.5.2-7, S4.5.2-8).
4. In adults with severe hypertriglyceridemia (fasting triglycerides ≥500 mg/dL
[≥5.7 mmol/L]), and especially fasting triglycerides ≥1000 mg/dL (11.3
mmol/L)), it is reasonable to identify and address other causes of
hypertriglyceridemia), and if triglycerides are persistently elevated or
IIa B-NR
increasing, to further reduce triglycerides by implementation of a very low-
fat diet, avoidance of refined carbohydrates and alcohol, consumption of
omega-3 fatty acids, and, if necessary to prevent acute pancreatitis, fibrate
therapy (S4.5.2-7, S4.5.2-9).
Synopsis
Two categories of elevated triglycerides consist of moderate hypertriglyceridemia (fasting or nonfasting
triglycerides 150-499 mg/dL [1.6-5.6 mmol/L]) and severe hypertriglyceridemia (fasting triglycerides ≥500
mg/dL [≥5.6 mmol/L]). In the former, excess triglycerides are carried in VLDL. In the latter, most patients
Page 52
5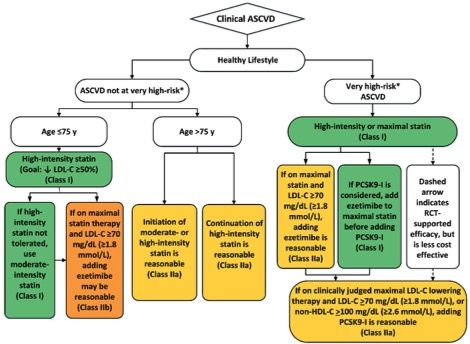
07/05/2019
ODYSSEY OUTCOMES
NEJM 2018;379:2097-2107
ALIROCUMAB vs PLACEBO
■ Supériorité, multicentrique, internationale, contrôlée, double aveugle, répartition
aléatoire, 18,000 patients entre novembre 2012 et novembre 2015
■ Syndrome coronarien aigu 1 à 12 mois (médiane 2,6 mois):
– C-LDL > 1,8 mmol/L ou
– Non-HDL > 2,6 mmol/L ou
– Apo-lipoprotéine B > 0,8 g/L
■ Exclusion: AVC hémorragique, défaillance, TG > 4,5 mM, hépatite, DFG < 30, etc.
■ Sanofi et Regeneron Pharmaceuticals
– Sélection des sites, supervision de l’essai et collecte de données
■ Pré-répartition 2 à 16 semaines > 2 semaines sous:
– Titration de la statine Atorvastatine > 40 mg par jour
88%
– Utilisation injecteur Rosuvastatine > 20 mg par jour
La plus haute dose tolérée
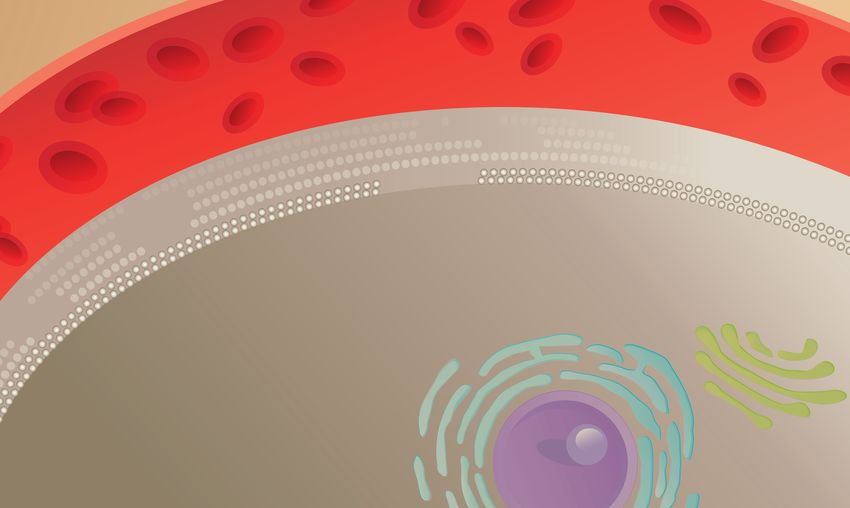
En présence de la PCSK9, le R-LDL est dégradé et ne
revient pas à la surface cellulaire
Le C-LDL sérique se lie aux récepteurs des LDL. À la suite de
cette internalisation, le récepteur est recyclé. Plasm a
LDL
PCSK9
LDL
R-LDL
R-LDL
Endocytose
Hépatocyte
Autoclivage
Endocytose de PCSK9
Endosom e
Recyclage
du R-LDL
Endosom e
Appareil
Dégradation de LDL de Golgi
Réticulum
endoplasmique
Dégradation par PCSK9, Noyau (RE)
LDL et R-LDL
© 2013 Amgen Canada Inc. Tous droits réservés
Qian YW, et al. J Lipid Res 2007;48:1488-1498.
Horton JD, et al. J Lipid Res 2009;50(suppl):S172-S177.
6
07/05/2019
L’anticorps monoclonal se lie à la PCSK9 et inhibe la
liaison au récepteur des LDL
Le fait d’entraver l’activité de la PCSK9 inhibe la Anticorps
monoclonal
dégradation intracellulaire du R-LDL LDL
anti-PCSK9
Plasm a
R-LDL
Recyclage
du R-LDL
Endocytose
Hépatocyte
Autoclivage
Endosome de PCSK9
Lysosome
Dégradation de LDL Appareil
de Golgi
Réticulum
endoplasmique
Noyau (RE)
© 2013 Amgen Canada Inc. Tous droits réservés
Qian YW, et al. J Lipid Res 2007;48:1488-1498.
Horton JD, et al. J Lipid Res 2009;50(suppl):S172-S177.
ODYSSEY OUTCOMES – intervention
NEJM 2018;379:2097-2107
0,4 0,6 1,3 1,8
C-LDL (mmol/L)
7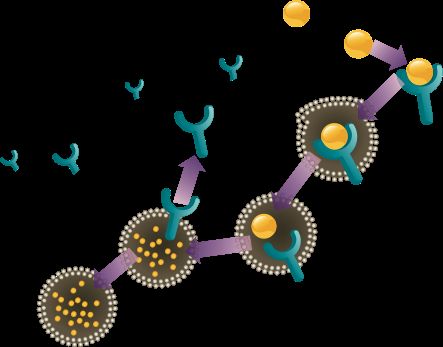
07/05/2019
ODYSSEY OUTCOMES – résultats
NEJM 2018;379:2097-2107
Alirocumab Placebo p
Efficacité primaire 9,5% 11,1% < 0,001
Critères d’évaluation secondaires
• Événements coronariens 12,7% 14,3% 0,001
• Décès coronariens et infarctus myocardique 8,4% 9,5% 0,006
• Événements cardiovasculaires (incluent PCI) 13,7% 15,6% < 0,001
• Décès toute cause, infarctus, AVC 10,3% 11,9% < 0,001
• Décès coronariens 2,2% 2,3% 0,38
C-LDL moyen
• 4 mois 1,0 mmol/L 2,4 mmol/L
• 12 mois 1,2 mmol/L 2,5 mmol/L
• 48 mois 1,7 mmol/L 2,7 mmol/L
ODYSSEY OUTCOMES– conclusion
NEJM 2018;379:2097-2107
■ Réduction des événements coronariens non fatals
■ Effet de classe
■ Cible C-LDL: 0,6 à 1,3 mmol/L
– Éviter C-LDL < 0,4 mmol/L
■ Ratio coûts-bénéfices
8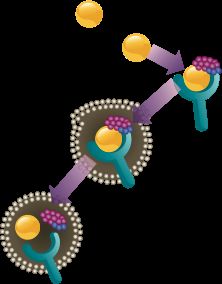
dansky, M.D., Andrew Farmer, D.M.,
scular cause, excluding Roger McPherson, B.M., F.R.C.Ophth., 07/05/2019
y outcome was the first Andrew Neil, D.Sc., F.R.C.P., David Simp-
ht-threatening bleeding son, Richard Peto, F.R.S., F.Med.Sci., Co-
lin Baigent, F.F.P.H., F.R.C.P., Rory Collins,
us bleeding). Secondary F.R.S., F.Med.Sci., Sarah Parish, D.Phil.,
and Jane Armitage, F.R.C.P., F.F.P.H.) as-
sume responsibility for the overall con-
Lignes directrices américaines
tent and integrity of this article. The affili-
novembre 2018
uring a mean follow-up ations of the members of the writing
committee are listed in the Appendix.
Très haut risque
ntly lower percentage of Address reprint requests toSCADr. < 12Armitage
mois
group (658 participants at the Medical Research Council, ATCD Infarctus
ATCD AVC Popula-
Maladie artérielle Trial
symptomatique
erval [CI], 0.79 to 0.97; tion Health Research Unit,> 65Clinical ans
Service Unit and Epidemiological Studies
4 participants (4.1%) in Unit, Nuffield DepartmentPACofouPopulation
HF hétérozygote
angioplastie
acebo group (rate ratio, Health, Richard Doll Bldg., Old HTA
DiabèteRoad Cam-
ess being gastrointesti- pus, Roosevelt Dr., Oxford OX3 DFGe 157LF,
à 59United
Tabagisme actif
mL/L
Kingdom, or at ascend@ndph C-LDL.>ox2,6.ac .uk sous
mmol/L or traitement
o significant difference jane.armitage@ndph.ox.acATCD .uk.défaillance
ncidence of gastrointes-T h e n e w e ng l a n d j o u r na l o f m e dic i n e
* A complete list of the members of the
spectively) or all cancers ASCEND Study Collaborative Group is
se outcomes is planned. provided in Supplementary Appendix 1,
Original
available Article
at NEJM.org.
Drs. Bowman and Mafham and Drs. Collins,
ho had diabetes and no Parish, and Armitage contributed equally
caused major Effects
bleedingof toAspirin for Primary Prevention
this article.
in Persons
by the bleeding hazard. with Diabetes Mellitus
This article was published on August 26,
END Current Controlled The 2018, at NEJM.org.
ASCEND Study Collaborative Group*
er, NCT00135226.) N Engl J Med 2018;379:1529-39.
DOI: 10.1056/NEJMoa1804988
A BS T R AC T
Copyright © 2018 Massachusetts Medical Society.
BACKGROUND
Diabetes mellitus is associated with an increased risk of cardiovascular events. The members
Aspirin use reduces the risk of occlusive vascular events but increases the risk of (Louise Bowma
M.D., Karl Wal
bleeding; the balance of benefits and hazards for the prevention of first cardiovas- vens, Ph.D., G
cular events in patients with diabetes is unclear. Barton, Kevin
M.D., Richard H
METHODS D.Phil., Aleksan
len Young, Ph
We randomly assigned adults who had diabetes but no evident cardiovascular dis- Fang Chen, M.D
1529
tober 18, 2018 ease to receive aspirin at a dose of 100 mg daily or matching placebo. The primary M.B., Ch.B., E
efficacy outcome was the first serious vascular event (i.e., myocardial infarction, Amanda Adler,
dansky, M.D.,
l of Medicine stroke or transient ischemic attack, or death from any vascular cause, excluding Roger McPher
any confirmed intracranial hemorrhage). The primary safety outcome was the first Andrew Neil, D
uary 30, 2019. For personal use only. No other uses without permission. 9
major bleeding event (i.e., intracranial hemorrhage, sight-threatening bleeding son, Richard Pe
l Society. All rights reserved. lin Baigent, F.F.
07/05/2019
ASCEND
NEJM 2018; 379: 1529-39
AAS vs PLACEBO
■ Supériorité, multicentrique, Royaume Uni, contrôlée, double aveugle, répartition
aléatoire, 15480 patients entre juin 2005 et juillet 2011
■ Hommes et femmes > 40 ans sans maladie cardiovasculaire chez qui il y avait une
incertitude sur les bénéfices de AAS.
■ Exclusions: indication ou contre-indication claire à utiliser AAS
■ Financée par British Heart Foundation
■ Conception et conduite de l’étude: investigateurs indépendants de l’Université d’Oxford
■ Bayer: comprimés de AAS et placebo. Commentaires sur conception étude et manuscrit
■ Période pré-répartition 8 à 10 semaines
■ AAS 100 mg avec enrobage entérique
ASCEND – critères d’évaluation
NEJM 2018; 379: 1529-39
■ Critère combiné d’efficacité primaire:
– Infarctus myocardiques non fatals
– AVC non fatals
– * Accidents ischémiques transitoires (ajouté en cours d’étude)
– Mortalité de toute cause vasculaire
■ Critère de sécurité primaire:
– Tout saignement majeur
■ Intracrânien
■ Intra-oculaire menaçant la vision
■ Gastro-intestinal
■ Tout saignement sérieux:
– Hospitalisation, transfusion, fatal
10M.D., Karl Wallendszus, M.Sc., Will Ste-
ds for the prevention of first cardiovas- vens, Ph.D., Georgina Buck, M.Sc., Jil
07/05/2019
nclear. Barton, Kevin Murphy, Theingi Aung
M.D., Richard Haynes, D.M., Jolyon Cox
D.Phil., Aleksandra Murawska, M.Sc., Al-
betes but no evident cardiovascular dis- len Young, Ph.D., Michael Lay, D.Phil.
Fang Chen, M.D., Ph.D., Emily Sammons
daily or matching placebo. The primary M.B., Ch.B., Emma Waters, M.B., B.S.
cular event (i.e.,ASCEND myocardial – population
infarction, Amanda Adler, M.D., Ph.D., Jonathan Bo-
ath from any vascular cause, excluding dansky,
NEJM 2018; 379: 1529-39 M.D., Andrew Farmer, D.M.
Roger McPherson, B.M., F.R.C.Ophth.
he primary safety Femmes
outcome was the first Andrew Neil,
Âge moyen 63 ans
38%
D.Sc., F.R.C.P., David Simp-
emorrhage, sight-threatening
IMC moyen bleeding son, Richard 30 kg/mPeto,
2 F.R.S., F.Med.Sci., Co-
lin Baigent,55%F.F.P.H., F.R.C.P., Rory Collins
or other serious bleeding).
Tabagisme (déjà ou actif)
AAS avant l’étude
Secondary F.R.S., F.Med.Sci.,
35% Sarah Parish, D.Phil.
ancer. Durée médiane du diabète 7 ans
and Jane Armitage, F.R.C.P., F.F.P.H.) as-
Médications
• Statines sume responsibility
75% for the overall con-
• ACEi ou ARB tent and integrity of this article. The affili-
59%
• Bêta-bloqueurs 13%
ndomization. During a mean follow-up
• IPP ations of the members of the writing
14%
committee are listed in the Appendix
d inAspirin
a significantly lower percentage
for Primary Prevention in Diabetes Mellitus
of Address reprint requests to Dr. Armitage
n the placebo group (658 participants at the Medical Research Council, Popula-
% confidence interval [CI], 0.79 to 0.97; tion Health Research Unit, Clinical Tria
ment to the use of Service
aspirin Unit
at a and
doseEpidemiological
of 100 mg Studies
sDiscussion
occurred in 314 participants (4.1%) in Unit, Nuffield Department
daily for 7.4 years resulted in a risk of seriousof Population
3.2%)persons
olving in thewhoplacebo
had diabetes group (rateevents
vascular ratio, Health,
that was 12%Richard
lower than Dollthat
Bldg., Old Road Cam-
with
pus, Roosevelt Dr., Oxford OX3 7LF, United
stmost of the excess
cardiovascular being gastrointesti-
disease, assign- placebo but also in a risk of major bleeding that
Kingdom, or at ascend@ndph.ox.ac.uk or
ng. There was no significant difference
ASCEND – événements vasculaires jane.armitage@ndph.ox.ac .uk.
group in the incidence of gastrointes-
scular Event
15 * A complete list of the members of the
nd 158 [2.0%],
100
respectively) or all cancers ASCEND Study Collaborative Group is
90 Rate ratio, 0.88 (95% CI, 0.79–0.97)
ollow-up for these P=0.01
outcomes is planned. provided in Supplementary
Placebo Appendix 1
80
Participants with Event (%)
10 available at NEJM.org.
70 Aspirin
Drs. Bowman and Mafham and Drs. Collins
ts in persons
60
who
5 had diabetes and no Parish, and Armitage contributed equally
50
ry, but it also caused major bleeding to this article.
40
ounterbalanced 0by the bleeding hazard. This article was published on August 26
30
nd others;
20
ASCEND
0 Current
1 2 Controlled
3 4 5 2018,
6 at NEJM.org.
7 8 9
rials.gov10 number, NCT00135226.) N Engl J Med 2018;379:1529-39.
DOI: 10.1056/NEJMoa1804988
0
0 1 2 3 4 5 Copyright
6 ©7 2018 Massachusetts
8 9 Medical Society.
Years of Follow-up
11
7740 7618 7486 7342 7188 7001 5771 3890 2200 1430d in a significantly lower percentage of Address reprint requests to Dr. Armitage
n the placebo group (658 participants at the Medical Research Council, Popula-
07/05/2019
% confidence interval [CI], 0.79 to 0.97; tion Health Research Unit, Clinical Tria
Service Unit and Epidemiological Studies
s occurred in 314 participants (4.1%) in Unit, Nuffield Department of Population
3.2%) in the placebo group (raten eratio,
w e ng l a n d jHealth,
o u r na l Richard
m e dic i n e Doll Bldg., Old Road Cam-
The of
most of the excess being gastrointesti- pus, Roosevelt Dr., Oxford OX3 7LF, United
Kingdom, or at ascend@ndph.ox.ac.uk or
ng. There was no significant difference jane.armitage@ndph.ox.ac.uk.
Type of Event
Aspirin
(N=7740)
Placebo
(N=7740) Rate Ratio (95% CI) P Value
no. of participants with event (%)
group in the incidence of gastrointes-
Vascular Outcomes
Nonfatal myocardial infarction
* A complete list of the members of the
191 (2.5) 195 (2.5) 0.98 (0.80– 1.19)
nd 158 [2.0%], respectively) or all cancers ASCEND Study Collaborative Group is
Nonfatal presumed ischemic stroke
Vascular death excluding intracranial hemorrhage
202 (2.6)
197 (2.5)
229 (3.0)
217 (2.8)
0.88 (0.73– 1.06)
0.91 (0.75– 1.10)
ollow-up for these outcomes is planned.
Any serious vascular event excluding TIA 542 (7.0) 587 (7.6) 0.92 (0.82–1.03)
TIA provided in Supplementary Appendix 1
168 (2.2) 197 (2.5) 0.85 (0.69– 1.04)
Any serious vascular event including TIA 658 (8.5) 743 (9.6) 0.88 (0.79–0.97) 0.01
Any arterial revascularization 340 (4.4) 384 (5.0) available at NEJM.org. 0.88 (0.76– 1.02)
Any serious vascular event or revascularization 833 (10.8) 936 (12.1) 0.88 (0.80–0.97)
Major Bleeding
Drs. Bowman and1.22
Mafham and Drs. Collins
ts in persons who had diabetes and no
Intracranial hemorrhage
Sight-threatening bleeding in eye
55 (0.7)
57 (0.7)
45 (0.6)
64 (0.8) Parish, and Armitage
(0.82– 1.81)
contributed equally
0.89 (0.62– 1.27)
Serious gastrointestinal bleeding 137 (1.8) 101 (1.3) 1.36 (1.05– 1.75)
ry, but it also caused major bleeding
Other major bleeding
Any major bleeding
74 (1.0)
314 (4.1)
43 (0.6)
245 (3.2)
to this article. 1.70 (1.18– 2.44)
1.29 (1.09–1.52) 0.003
ounterbalanced by the bleeding hazard. 0.5 0.7 1.0 1.5
This article was published on August 26
2.0
nd others; ASCEND Current Controlled
Aspirin Better
Placebo Better
2018, at NEJM.org.
Figure 2. Effect of Assignment to Aspirin Group on Components of Serious Vascular Events, the Combined Outcome of Serious Vascular
rials.gov number, NCT00135226.)
Event or Revascularization, and Major Bleeding and Its Components.
N Engl J Med 2018;379:1529-39.
The primary outcome was a serious vascular event (a composite of nonfatal myocardial infarction, nonfatal ischemic stroke or transient
DOI: 10.1056/NEJMoa1804988
ischemic attack [TIA], or death from any vascular cause, excluding confirmed intracranial hemorrhage). Secondary outcomes were a seri-
ous vascular event or any coronary or noncoronary revascularization procedure. A single participant may have had multiple events and
therefore may contribute information to more than one row. The size of eachCopyright ©ratio
square for the rate 2018 Massachusetts
is proportional to the amountMedical
of Society.
statistical information that was available, the horizontal lines represent 95% confidence intervals, and the dashed vertical line indicates
the overall rate ratio for the effect of aspirin use on the first serious vascular event. An arrow on the horizontal line indicates that the
confidence interval exceeds the graph area. For composite outcomes, rate ratios and their corresponding 95% confidence intervals are
represented by diamonds. Bold entries with diamonds show totals for all data listed above them. The effect of aspirin use on the com-
ponents of the primary safety outcome of major bleeding event (a composite of intracranial hemorrhage, sight-threatening bleeding
event in the eye, gastrointestinal bleeding, or other major bleeding event) is shown with the use of the same graphic conventions.
ANTIPLAQUETTAIRES
was 29% higher. The lower risk of serious vascu- of the participants who underwent randomiza-
PRÉVENTION
lar events is similar toPRIMAIRE
the risk that was reported
previously in the Antithrombotic Trialists’ Col-
tion have allowed reliable detection of these
moderate but important effects on the incidence
laboration meta-analysis of primary prevention of vascular events and on both the severity and
16 nejm.org ■ Bénéfice
October mitigé
18,
trials of2018dans une
similar dosespopulation
of aspirinà (which
faible risque d’événement
used incidence (environ
of bleeding. 10%
Our à 10 do not sup-
findings 1529
ans) avec un bon
slightly contrôle
different des facteurs
outcome de risque
definitions; see the(lipides, HTA)
port the hypothesis that persons with diabetes
– Les Methods section in
événements Supplementary
évités sont moins Appendix
solides1). have a resistance to aspirin. Although the pro-
1 9
New England Journal of MedicineIn contrast to those previous trials, there were portional effects of aspirin use are likely to be
■ Accidents ischémiques transitoires
high rates of the use of cardioprotective treat- generalizable to the wider population of persons
L SEC ACQ on January 30, 2019. For personal use only. No other uses without permission.
■ments
Troponine
amongultra sensible
the participants in ASCEND, with with diabetes, the absolute event rates and ad-
assachusetts Medical Society. All rights reserved.
■ Risquethe majority of participants
hémorragique takingéquivoque
augmenté sans statins and herence rates reflect this population of persons
blood pressure–lowering therapy. Hence, the pres- with well-treated diabetes. Overall, on the basis
■ NNT = ent
NNH (100)
trial même
provides chez assessment
a direct populationofà the
risque
bal- élevé
of the absolute percentage differences between
ance
■ Rôle des IPP? of the benefits and hazards of aspirin use the groups in the incidence of serious vascular
in a contemporary context. events (1.1 percentage points lower in the aspi-
In our trial, factors such as the large number rin group than in the placebo group) and in
of participants and clinical outcomes, long dura- bleeding events (0.9 percentage points higher in
tion of follow-up, the randomized, blinded design the aspirin group), 91 patients would need to be
of the trial, and the almost complete follow-up treated to avoid a serious vascular event over a
1536 n engl j med 379;16 nejm.org October 18, 2018
The New England Journal of Medicine
Downloaded from nejm.org at BIBLIOTHEQUE UNIV LAVAL SEC ACQ on January 30, 2019. For personal use only. No other uses without permission.
Copyright © 2018 Massachusetts Medical Society. All rights reserved.
12efit observed in the entire Primary Prevention Project population,
d 5-year risk of CAD. Similar results were lesser benefits were noted in the diabetic cohort.138 Further, an
nts (RR 0.82, 95% CI 0.75-0.90; P !
roke (RR 0.86, 95% CI 0.74-1.00; P !
earlier meta-analysis conducted by the Antithrombotic Trialists’ 07/05/2019
Collaboration12 failed to demonstrate any benefit for ASA in sub-
fit was noted. Although the proportional jects with diabetes, whereas a 22% relative risk reduction was ob-
vents offered by ASA were similar in the served overall. Similarly, smoking, which is used in most risk strat-
prevention trials, the absolute risk reduc- ification methods, attenuated the benefit of ASA observed in the
der of magnitude. Absolute annual risk Women’s Health Study141 and the Physician’s Health Study,134
vents, MI, and ischemic stroke in primary consistent with data indicating that smoking increases ASA resis-
.07% (NNT for 1 year 1428), 0.06% tance.147 An Antithrombotic Trialists’ Collaboration prediction
), and 0.02% (NNT for 1 year 5000), model of high-risk subjects (ie, those with a 10-year event rate
ociated with a 32% increase in the relative
CCS 2010 – AAS prévention primaire
ke (RR 1.32, 95% CI 1.00-1.75; P !
ase 0.01%) and a 54% increase in the
# 20%) receiving statin therapy suggests that the absolute benefit
of ASA in primary vascular protection is small and approximately
equivalent to the risk of major bleeding.66
xtracranial bleeding (RR 1.54, 95% CI
absolute risk increase 0.03%). The same RECOMMENDATION (Summarized in Fig. 10 )
ascular risk were also noted to increase
risk did not differ significantly in the For men and women without evidence of manifest vas-
prevention analyses, but the very low cular disease, the use of ASA at any dose is not recom-
fit of ASA in primary prevention was mended for routine use to prevent ischemic vascular events
d by bleeding. In contrast, in second- (Class III, Level A).
ascular benefit far outweighed the For men and women without evidence of manifest vas-
cular disease, the use of clopidogrel 75 mg daily plus ASA at
any dose is not recommended to prevent ischemic vascular
events (Class III, Level B).
efit of any intervention is dictated by the In special circumstances in men and women without
ted adverse events, and absolute event evidence of manifest vascular disease in whom vascular risk
ortional treatment effect of ASA is similar is considered high and bleeding risk is low, ASA 75-162 mg
ry prevention, the low event rate in pri- daily may be considered (Class IIb, Level C).
shes or possibly nullifies the absolute net
f the studies considered were conducted
use of other primary risk reduction thera-
nd inhibitors of the RAAS, which would Use of Antiplatelet Therapy in Patients With
absolute event rates and net benefit of Diabetes
events are likely to have a greater impact Working Group: Maria E. Kraw, MD, FRCP, and Rémi
ity than bleeding and the cost of ASA is Rabasa-Lhoret, MD,ACCEPTED
PhD MANUSCRIPT
nefit must apply before recommending
Arnett et aal. Cardiovascular disease is a major cause of mortality and mor-
148
y population. Although many2019 guidelines bidity foron
ACC/AHA Guideline patients with diabetes.
the Primary PreventionInofaddition to traditional
Cardiovascular risk
Disease
A for primary prevention based on age or ACCEPTED
factors such as smoking, MANUSCRIPT
systemic hypertension, dyslipidemia, and
6,143-145
the benefit in such populations dysglycaemia, atherosclerosis in patients with diabetes can be as-
2019 ACC/AHA
Arnett et al. Guideline on the Primary Prevention of Cardiovascular
2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease
Disease
4.6. Aspirin
A Report Use
of the American College of Cardiology/American Heart Association Task Force on
Recommendations
Clinical Practicefor Aspirin Use
Guidelines
Referenced studies that support recommendations are summarized in Online Data Supplements 17
and 18.
Endorsed LOE
COR by the American Association of Cardiovascular and Pulmonary Rehabilitation, the American
Recommendations
Geriatrics Society, the American Society of Preventive Cardiology, and the Preventive Cardiovascular
1. Low-dose aspirin (75-100 mg orally daily) might be considered for the
Nurses Association
PT
IIb A primary prevention of ASCVD among select adults 40 to 70 years of age who
are at higher ASCVD risk but not at increased bleeding risk (S4.6-1–S4.6-8).
2. Low-dose aspirin (75-100 mg orally daily) should not be administered on a
III: WRITING
B-R routine basis for the COMMITTEE MEMBERS
primary prevention of ASCVD among adults >70 years of
RI
Harm Donna K. Arnett, PhD, MSPH, FAHA, Co-Chair
age (S4.6-9).
Roger S.
3. Low-dose Blumenthal,
aspirin (75-100MD,
mgFACC,
orallyFAHA,
daily) Co-Chair
should not be administered for the
III:Michelle A. Albert, MD, MPH, FAHA*
C-LD primary prevention of ASCVD amongD.adults
Erin Michos,
of MD, MHS,who
any age FACC,
areFAHA*
at increased
SC
Harm Andrew B. Buroker, Esq† Michael D. Miedema, MD, MPH*
risk of bleeding (S4.6-10).
Zachary D. Goldberger, MD, MS, FACC, FAHA‡ Daniel Muñoz, MD, MPA, FACC*
Ellen J. Hahn, PhD, RN* Sidney C. Smith, Jr, MD, MACC, FAHA*
Synopsis
Cheryl D. Himmelfarb, PhD, RN, ANP, FAHA* Salim S. Virani, MD, PhD, FACC, FAHA*
For decades, aspirin has been widely administered for ASCVD prevention. By irreversibly inhibiting
U
Amit Khera, MD, MSc, FACC, FAHA* Kim A. Williams, Sr, MD, MACC, FAHA*
platelet function, aspirin reduces risk of atherothrombosis but also increases risk of bleeding,
Donald Lloyd-Jones, MD, SCM, FACC, FAHA* Joseph Yeboah, MD, MS, FACC, FAHA*
particularly in the gastrointestinal tract (S4.6-11). Aspirin is well established for secondary prevention of
AN
J. William McEvoy, MBBCh, MEd, MHS* Boback Ziaeian, MD, PhD, FACC, FAHA§
ASCVD (S4.6-12) and is widely recommended for this indication (S4.6-13). However, in primary
prevention, aspirin use is more controversial. Because persons without prior ASCVD are inherently less
likely to have future ASCVD events than are
ACC/AHA TASKthose
FORCEwith a prior history, it is more challenging for
MEMBERS
M
clinicians and patients to balance benefits
Patrick and harms
T. O’Gara, of prophylactic
MD, MACC, aspirin for primary prevention. This
FAHA, Chair
uncertainty is reflected in international guidelines,
Joshua A. Beckman, MD,where, for example,
MS, FAHA, Chair-Electaspirin is not recommended in 13
European guidelines for Glennprimary ASCVD
N. Levine, prevention
MD, FACC, FAHA, (S4.6-13)
ImmediatebutPastisChair║
recommended in prior U.S.07/05/2019
PIONEER AF PCI
NEJM 2016;375:2423-34
■ Étude ouverte multicentrique internationale
■ Patients avec fibrillation auriculaire subissant tuteur coronarien 72 heures avant répartition
Rivaroxaban 2,5 mg BID
Rivaroxaban 15 mg die AVK + AAS + P2Y12
+ AAS + P2Y12 p
+ P2Y12 (1, 6 OU 12 mois)
(1, 6 ou 12 mois)
Saignements
16,8% 18% 26,7% < 0,001
significatifs (TIMI)
MACE 6,5% 5,6% 6% NS
Thromboses tuteur 5 6 4 NS
RE-DUAL PCI
NEJM 2017;377:1513-24
■ Étude ouverte multicentrique internationale
■ Patients avec PCI dans les 120 heures avant répartition (SCA ou angor stable) avec
fibrillation auriculaire non valvulaire
AVK + P2Y12 +
DABI 150 + DABI 110 +
AAS Non infériorité
P2Y12 P2Y12
(1 À 3 MOIS)
Saignement majeur (ISTH) ou 20,2% 15,4% 26,9% oui
cliniquement significatif
Évén. thromboembolique, décès ou 11,8% 15,2% 13,4% oui
revascularisation non planifiée
Évén. thromboembolique ou décès 7,9% 11% 8,5% non
Thromboses de tuteurs 7 15 8 non
1407/05/2019
AUGUSTUS
NEJM mars 2019
APIXABAN vs WARFARINE
AAS vs PLACEBO
■ multicentrique, internationale, ouverte pour le volet AOD vs AVK, aveugle pour le
volet AAS vs PLACEBO, répartition aléatoire, 4614 patients entre septembre 2015 et
avril 2018
■ Patients recevant un tuteur coronarien dans les 14 jours avant la répartition Temps moyen
6,6 jours
■ Exclusions: anticoagulation pour une autre raison que FA, etc.
■ Financement par BMS et Pfizer
– Gestion des données
■ Gestion de l’étude et analyse des données par un centre académique indépendant
AUGUSTUS – paramètre d’évaluation
NEJM mars 2019
■ Saignements majeurs
– Décès
– Organe critique
■ Intra-crânien, spinal, oculaire, articulaire, péricardique, rétropéritonéal, musculaire
(compartiment)
– Chute Hb 20 g/L
– Transfusion 2 culots globulaires
■ Saignements cliniquement significatifs
– Hospitalisation, intervention médicale ou chirurgicale, visite médicale non
planifiée, changement de thérapie anti-thrombotique
1507/05/2019
AUGUSTUS – population
NEJM mars 2019
Âge moyen 70 ans
Femmes 30%
Caucasiens 92%
CHA2DS2-VASc moyen 4
HASBLED moyen 3
événement index
• SCA et tuteur(s) 38%
• SCA traité médicalement 24%
• Tuteur(s) électif(s) 38%
Clopidogrel 93%
AVK: Temps dans l’intervalle thérapeutique 59%
Délai moyen après événement index 6,6 jours
AUGUSTUS – résultats AOD vs AVK
NEJM mars 2019
Apixaban 5 mg BID AVK p
Saignements majeurs et cliniquement 10,5% 14,7%07/05/2019
AUGUSTUS – résultats AAS vs placebo
NEJM mars 2019
AAS placebo
Saignements majeurs et cliniquement 16,1% 9,0%07/05/2019
CCS 2018:
CARACTÉRISTIQUES HAUT RISQUE
■ Diabète ■ Multipes tuteurs
■ ATCD SCA ■ Lésion complexe de la bifurcation
■ DFGe < 60 mL/min ■ Longueur totale de tuteur > 60 mm
■ ATCD thrombose tuteur ■ Intervention sur thrombose
chronique
■ Fumeur
■ Maladie multi-vasculaire
226 Canadian Journal of Cardiology
Volume 34 2018
CCS 2018
* Rivaroxaban 15 mg die ou
Dabigatran 150 ou 110 mg BID ou
AVK
Figure 3. Recommendations for patients with AF without high-risk features who undergo elective PCI. ACS, acute coronary syndrome; AF, atrial
fibrillation; ASA, acetylsalicylic acid; BID, twice daily; BMS, bare-metal stent; CCS, Canadian Cardiovascular Society; CHADS2, Congestive Heart
Failure, Hypertension, Age, Diabetes, Stroke/Transient Ischemic Attack; DES, drug-eluting stent; INR, international normalized ratio; OAC,18
oral
anticoagulant; PCI, percutaneous coronary intervention; SAPT, single antiplatelet therapy.antithrombotic management 07/05/2019
Downloaded from http://ahajournals.org by on April 28, 2019
percutaneous coronary interv
Figure 3. Recommendations for patients with AF without high-risk features who undergo elective PCI. ACS, acute coronary syndrome; AF, atrial
fibrillation; ASA, acetylsalicylic acid; BID, twice daily; BMS, bare-metal stent; CCS, Canadian Cardiovascular Society; CHADS , Congestive Heart 2
anticoagulant; antagonist
et al percutaneous coronary intervention; SAPT, single antiplatelet therapy. oral
Antithrombotic anticoagulan
Failure, Hypertension, Age, Diabetes, Stroke/Transient Ischemic Attack; DES, drug-eluting stent; INR, international normalized ratio; OAC, oral
AngiolilloPCI, Therapy in AF Patients After PCI
not have AF, ASA used in addition to very low dose OAC
as the oral anticoagulant of c
evaluated for long-term stroke prevention in patients with AF.
cally higher
(rivaroxaban
ticagrelor
2.5 mgamong patientsmajor
BID) reduced
compared with
who CV
those
were treated
events.
treated with
It iswith The
clopi-
Strategy
(oral
standard
Duration
stroke anticoagulant
(Double
of
Versus Triple
prevention
Therapy
dose ofTherapy)
rivaroxaban plus
and
singl
in patients
STATE OF THE ART
important to note that rivaroxaban 2.5 mg BID has not been with AF is 15 mg or 20 mg daily. Consideration could be
dogrel, consistent CCS 2018
with the data from PLATO and its
higher antiplatelet effect. Thus, more data on the
by
Randomized the
clinical time
trials have of hospital
shown
of double antithrombotic therapy, consisting of OAC in
37
that a strategy discha
use of ticagrelor in combination with OAC are war- whereas
combination with a P2Yextending(without aspirin),the starteduse at o 12
ranted. This expert consensus suggests tailoring the the time of hospital discharge is associated with sig-
intensity of P2Y -inhibiting therapy according to risk. therapy)
nificantly should
lower risk of bleeding
12
be considere
complications without
Therefore, among patients at high ischemic/throm- an apparent tradeoff in thrombotic events compared
botic (eg, patients with acute coronary syndromes) thrombotic
with triple therapy. and low
Accordingly, bleeding
this consensus 6,7,9,40
and low bleeding risks, ticagrelor may represent a
reasonable treatment option. Ticagrelor should be
present document provides a
recommends double therapy for most patients (de-
fault strategy; Figure 2). In patients in whom double
administered as a 180-mg loading dose and 90-mg therapynew expert
is considered, aspirinconsensus–derive
is recommended in the
twice daily maintenance dose; a 60-mg twice daily peri-PCI phase. Given the irreversible binding of aspirin
maintenance dose regimen immediately after PCI has to the management
COX-1 enzyme, residual platelet of patientsinhibitory ef- with
not been studied. Circulation
This expert consensus
that if ticagrelor is chosen as the P2Y agent, con-
recommends fects persist for the
anticoagulation
(7–10 days).
life span of the
However, in selected patients
affected
undergoing
platelet
considered p 41
12
comitant aspirin not be given (ie, avoid triple thera- at high ischemic/thrombotic risk and low bleeding risk,
py), as was done in the RE-DUAL PCI trial.7 Data on *Rivaroxaban
this 2,5 mg diefinds
expert consensus ou AVK
it reasonable to continue
puis Rivaroxaban 15 mg die ou
WHITE
the combination PAPER
of prasugrel with an NOAC are very with aspirin therapy (ie, triple therapy) for a limited
Dabigatran 150 ou 110 mg BID
limited, but 1 small study found a nearly 4-fold in- period of time after hospital discharge. Although the
crease in bleeding with triple therapy with prasugrel,39 duration of aspirin treatment is at the discretion of the
and thus, the use of this agent is not recommended. Antithrombotic Therapy in Patients With Atrial treating physician, in these selected patients, it is rea-
Furthermore, this expert consensus continues to rec-
ommend against the routine use of platelet function Fibrillation Treated With Oral Anticoagulation sonable to extend aspirin therapy up to 1 month after
PCI and rarely beyond this time (Figure 2).
or genetic testing to guide the selection of antiplatelet
therapy.5
Undergoing Percutaneous Coronary Intervention The duration of the dual-therapy regimen and thus
timing of discontinuation of SAPT should also take into
A North American Perspective–2018 Update
Figure 4. Recommendations for patients with AF who undergo PCI for ACS or high-risk elective PCI. ACS, acute coronary syndrome; AF, atrial
fibrillation; ASA, acetylsalicylic acid; BID, twice daily; CCS, Canadian Cardiovascular Society; CHADS2, Congestive Heart Failure, Hypertension, Age,
Downloaded from http://ahajournals.org by on April 28, 2019
Diabetes, Stroke/Transient Ischemic Attack; DAPT, dual antiplatelet therapy; INR, international normalized ratio; OAC, oral anticoagulant; PCI,
percutaneous coronary ABSTRACT:
intervention. The optimal antithrombotic treatment regimen for patients Dominick J. Angiolillo,
with atrial fibrillation undergoing percutaneous coronary intervention MD, PhD
with stent implantation represents a challenge in clinical practice. In Shaun G. Goodman, MD
2016, an updated opinion of selected experts from the United States and Deepak L. Bhatt, MD,
Canada on the treatment of patients with atrial fibrillation undergoing MPH
percutaneous coronary intervention was reported. After the 2016 North John W. Eikelboom, MD
American consensus statement on the management of antithrombotic Matthew J. Price, MD
therapy in patients with atrial fibrillation undergoing percutaneous David J. Moliterno, MD
Christopher P. Cannon,
coronary intervention, results of pivotal clinical trials assessing the type of
MD
oral anticoagulant agent and the duration of antiplatelet treatment have
Jean-Francois Tanguay,
been published. On the basis of these results, this focused update on the MD
antithrombotic management of patients with atrial fibrillation undergoing Christopher B. Granger,
Downloaded from http://ahajournals.org by on April 28
percutaneous coronary intervention recommends that a non–vitamin K MD
antagonist oral anticoagulant be preferred over a vitamin K antagonist Laura Mauri, MD
as the oral anticoagulant of choice. Moreover, a double-therapy regimen David R. Holmes, MD
(oral anticoagulant plus single antiplatelet therapy with a P2Y12 inhibitor) C. Michael Gibson, MD
by the time of hospital discharge should be considered Circulation. for most patients, 2018;138:527–536.
David P. Faxon, MDDOI: 10.1161
whereas extending the use of aspirin beyond hospital discharge (ie, triple
therapy) should be considered only for selected patients at high ischemic/
thrombotic and low bleeding risks and for a limited period of time. The
present document provides a focused updated on the rationale for the
Figure 2. Management
new of antiplatelet
expert therapy in patients
consensus–derived with atrial fibrillationon
recommendations undergoing percutaneous coronary intervention (PCI) treated with
the antithrombotic
an oral anticoagulant (OAC): 2018 North American expert consensus update.
management of patients with atrial fibrillation treated with oral
A double-therapy regimen immediately after hospital discharge should be considered for most patients (default strategy). A non–vitamin K antagonist oral antico-
anticoagulation
agulant (NOAC) should be preferred overundergoing percutaneous
a vitamin K antagonist (VKA) unlesscoronary intervention.
contraindicated. 19
Single antiplatelet therapy (SAPT), preferably with a P2Y12 inhibitor,
should be started as soon as possible, including at hospital discharge. It is reasonable to extend low-dose aspirin therapy (ie, triple therapy) up to 1 month after3. Intravenous beta blockers are recommended to slow a rapid ventricular
contraindications to long-term anticoagulation and who are at high risk of thromboembolic events.
I C
response to AF in patients with ACS who do not display HF, hemodynamic
Section 6.3.4 - Catheter Ablation
instability,inorHF bronchospasm. 07/05/2019
4. If triple therapy (oral anticoagulant, aspirin, and P2Y12 inhibitor) is prescribed
Catheter ablation of AF isfor reasonable
patients with in symptomatic
AF at increased AF risk
patients with (based
of stroke HF andonreduced
CHA2DSLVEF.
2-VASc risk
score of 2 or greater) who have undergone percutaneous coronary intervention
SectionIIa7.4 - Complicating
B-NR Acute Coronary Syndrome
(PCI) with stenting for ACS, it is reasonable to choose clopidogrel in preference
If triple therapy is prescribed post-stent placement, clopidogrel is preferred over prasugrel.
to prasugrel.
NEW: New published data are available.
Double therapy with a P2Y5. In12 inhibitor
patients with andAFdose adjusted
at increased riskvitamin
of stroke K (based
antagonist
on CHAis 2reasonable
DS2-VASc risk post-stenting.
score
of 2 or greater) who have undergone PCI with stenting for ACS, double therapy
Double therapy with clopidogrel
with a P2Y and12low-dose
inhibitor rivaroxaban
(clopidogrel or (15ticagrelor)
mg daily)and maydose-adjusted
be reasonable post-stenting.
vitamin K
2850
ACC/AHA 2019
IIa B-R
Double therapy with a P2Y
antagonist is reasonable to reduce the risk of bleeding as compared with triple
12 inhibitor and dabigatran 150 mg twice daily is reasonable post-stenting.
therapy.
NEW: New RCT datawith and AF
datawho
fromare 2 registries and arisk
retrospective CardioPulse
If triple therapy is prescribed for patients at increased of strokecohort
and who study have
are available.
undergone PCI with stenting for ACS, a transition to double therapy at 4-6 weeks may be considered.
6. In patients with AF at increased risk of stroke (based on CHA2DS2-VASc risk score
of 2 or greater) who have undergone PCI with stenting for ACS, double therapy
Section 7.12 - Device Detection of AF and Atrial Flutter
IIa B-R with P2Y12 inhibitors (clopidogrel) and low-dose rivaroxaban (15 mg daily) is
reasonable
In patients with cardiac implantable
AF Pa!ents to reduce
electronic the risk of with
devices,
presen!ng bleeding as compared
atrialElec!ve
high ratePCI orwith
episodes triple
ACS(AHREs) therapy.
undergoing shouldPCI prompt
1
NEW: New published data are available.
further evaluation.
7. In patients with AF at increased risk of stroke (based on CHA2DS2-VASc risk
In patients with cryptogenic score of 2 or
stroke ingreater) who have undergone
whom long-term PCI with stenting
external ambulatory for ACS,
monitoring is double
IIa B-R Concerns
therapy with about
a P2Y12 inhibitor (clopidogrel) and dabigatran 150bleeding
mg twice daily
inconclusive implantationisofreasonable
a cardiactomonitor Concerns about high risk 3
thrombo!c reduce is
risk thereasonable to detect silent AF.
2
risk of bleeding as compared with
prevailing triple therapy.
NEW: prevailing
New published data are available.
Section 7.13 - Weight Loss
8. If triple therapy (oral anticoagulant, aspirin, and P2Y12 inhibitor) is prescribed
Downloaded from https://academic.oup.com/eurheartj/article-abstract/39/31/2847/5076806 by Universite Laval user on 29 April 2019
Weight loss and risk factor for modification
patients with AF is recommended
who are at increasedfor overweight/obese
risk of stroke (based patients
on CHA2with AF.
DS2-VASc
Time from
treatment IIb
risk score of 2 or greater) and who have undergone PCI with stenting (drug
B-R
ini!a!on eluting O or bare
A Cmetal) for ACS, a transition O to A double
C O C
therapy (oral anticoagulant
I IIa IIb and P2YIII 12 inhibitor) at 4 to 6 weeks 1 may be considered.
1 mo. Triple Therapy mo. Triple Therapy [Pa!ent at very high bleeding risk]
NEW: New published data are available.
1mo.
ACC.org/AFCompare 9. Administration of amiodarone or digoxin may be consideredDual to slow
Therapya rapid
with OAC plus
IIb C ventricular response in patients with ACS and AF associatedP2Y12 withinhibitor
severeupLVto 12 mo.
dysfunction and HF or hemodynamic instability.
5
10. Administration of nondihydropyridine calcium
3mo. IIb O A C O C antagonists may be considered
C to slow a rapid ventricular response in patients with ACS and AF only in the
Triple Therapy Dual Therapy with OAC plus
absence of significant HF or hemodynamic
up to 6 mo.
instability.
up to 6 mo. P2Y12 inhibitor up to 12 mo.
2850 (Class IIa) . CardioPulse
CardioPulse 2847
6mo.
doi:10.1093/eurheartj/ehy396
O C 13
Management of antithrombotic therapy in AF
patients presenting with
P2Y12 ACS
inhibitor up toand/or
12 mo.
EUROPE
Dual Therapy with OAC plus AF Pa!ents presen!ng with Elec!ve PCI or ACS undergoing PCI1
12mo.
undergoing PCI .
Concerns about
Downloaded from https://academic.oup.com/eurheartj/article-abstract/39/31/2847/5076806 by Universite Laval user on 29 April 2019
A Summary of the Joint Consensus Document of the European Heart Rhythm Concerns about high bleeding risk3
thrombo!c
Group onrisk
2
Association (EHRA), European Society of Cardiology Working prevailing
Beyond
Thrombosis, European Association of Percutaneous prevailing
Cardiovascular InterventionsO
12mo.
Downloaded from https://academic.oup.com/eurheartj/article-abstract/39/31/2847/5076806 by Universite Laval user
(EAPCI) and European Association of Acute Cardiac Care (ACCA) endorsed by the
OAC alone
Heart Rhythm Society (HRS), Asia-Pacific Heart Rhythm Society (APHRS), Latin
Time from
America Heart Rhythm Society (LAHRS),
treatment
and Cardiac Arrhythmia Society of
Southern Africa (CASSA) ini!a!on O A C O A C O C
1:Periprocedural
administra!on of aspirin and clopidogrel during PCI Therapy
is recommended
1 mo. Triple Therapy 1 mo. Triple [Pa!entirrespec!ve of the
at very high bleeding risk]
OSinceOral an!coagulant with
VKA (TTR>70%) or NOAC
treatment1mo.
publication of the 2014 joint consensus document
strategy;
dealing Michael as dual
Haude therapy,
(Germany), and Kurtpotent P2Y12
Huber (Austria). inhibitors (ticagrelor) may be combined with dabigatran
In addition,
Dual Therapy with OAC plus
with the management of antithrombotic therapy in atrial fibrillation a group of 22 reviewers co-ordinated by Tatjana Potpara (Serbia)
A(AF)
Aspirin : High(ACS)
2
patients presenting with acute coronary syndrome atherothrombo!c
and/ riskintroducing
revised the manuscript (For Elec!ve PCI,and
many suggestions use SYNTAX score; for ACS, GRACE score >140; sten!ng of the le"
criticisms,
P2Y12 inhibitor up to 12 mo.
main, proximal manuscript.
or undergoing percutaneous coronary (PCI) or valve interventions,
which represented an effort of the European Society of Cardiology
LAD, proximal bifurca!on; recurrent MIs; stent thrombosis etc.) and low bleeding risk
which contributed to the quality and comprehensiveness of the
CWorking
Clopidogrel 3mo.
Group (ESC) on Thrombosis, European Heart
3: Bleeding
Association (EHRA), European Association
Rhythm O A C O C
risk can be es!mated using the HAS-BLED score; correct modifiable bleeding risk factors
of Percutaneous
Triple Therapy Dual Therapy with OAC plus
Cardiovascular Interventions (EAPCI) and European Association of
up to 6 mo. P2Y12 inhibitor up to 12 mo.
Acute Cardiac Care (ACCA),1 endorsed by the Heart Rhythm
Society (HRS) and Asia-Pacific Heart Rhythm Society (APHRS) (Class IIa) .
there have been additional data from observational cohorts,
randomized controlled trials and advances in percutaneous
6mo.
Gregory Y.H. Lip
interventions.
Professor of Cardiovascular Medicine
New guidelines have also been published, as well as new drugs, devi-
C
OJean-Philippe Collet (France)
University of Birmingham, UK ACTION Study Group Institut de Cardiologie
ces, and interventional techniques in AF, ACS management, and PCI.2,3 Dual Therapy with OAC plus
Groupe Hospitalier Pitié-Salpêtrière 47-83,
E-mail: g.y.h.lip@bham.ac.uk
P2Y12 inhibitor up to 1275013,
mo. Paris, France. Michael Haude (Germany)
Atrial fibrillation management
Price-Evans has also evolved
Chair of Cardiovascular towards a more inte-
Medicine Boulevard de l'Hôpital,
grated or(from
holistic approach
1 Feb 12mo.
2019)that includes the following components: .
Tel: +33.1.42.16.29.62
Email: michael.haude@uni-due.de
University of Liverpool, UK Fax : +33.1.42.16.29.31
• ‘A’ Avoid stroke
Email: with Anticoagulation;
gregory.lip@liverpool.ac.uk
• ‘B’ Better symptom
Tel: +44 management, with patient centred decisions on
121 5075080
Email: jean-philippe.collet@aphp.fr
rate or rhythm control; and
• ‘C’ Cardiovascular and comorbidity risk management, Beyond
The full version of this important consensus document is pub- O
including life-
lished in EP Europace.4 We hope this consensus document is user-
style changes.4 12mo. friendly, based on ranking using the EHRA ‘coloured hearts’ system
OAC alone
In recognizing this new information since the last consensus docu-
ment, a Task Force was convened by EHRA, WG Thrombosis, EAPCI, the evidence and offer consequent guidance. The ultimate aim of
Astra-Zeneca, Bayer, Lead-Up, WebMD. MH: Grant support:
that should allow physicians to easily assess the current status of
the Task Force was 1to:Periprocedural
prepare an expert administra!on of aspirin and clopidogrel during PCI is recommended irrespec!ve of the
and ACCA, with additional contribution from HRS, APHRS, Latin
America Heart Rhythm Society (LAHRS), and Cardiac O Oral an!coagulant
Arrhythmia
Biotronik, Orbus Neich, Abbott, Medtronic, Cardiac Dimensions
consensus and evidence-
with reviewing the best available scientific evidence on
based document treatment strategy; as dual therapy, potent P2Y12 inhibitors (ticagrelor) may be combined with dabigatran
Kurt Huber (Austria) VKA (TTR>70%) or NOAC
Society of Southern Africa (CASSA), to produce an updated consen-
Email:withkurt.huber@meduniwien.ac.at
this growing issue, and
2
to update the
: Highcommunity
current
atherothrombo!c Speaker’s bureau: Biotronik, Orbus Neich, Abbott, Medtronic, Lilly,
knowledge in this field,
riskspecialists
(For Elec!ve PCI, use SYNTAX score; for ACS, GRACE score >140; sten!ng of the le"
sus document, A theAspirin
the remit of comprehensively reviewing avail- not only for the cardiology but also for other
able evidence and providing up-to-date consensus recommendations who see patients with main, proximal
AF and acute or LAD,
stable proximal bifurca!on; recurrent MIs; stent thrombosis etc.) and low bleeding risk
Philips / Volcano, Cardiac Dimensions (Proctor)Consultant: Biotronik,
coronary artery dis-
for use in clinical practice. C Clopidogrel ease, particularly cardiologists, general internists, and general prac-
3: Bleeding risk can be es!mated using the HAS-BLED score; correct modifiable bleeding risk factors
The consensus document has been written by 16 authors, chaired by titioners, which have to make daily decisions on such Orbus Neich, Abbott. KH: Lecture fees from AstraZeneca, Bayer,
patients in
Gregory Y.H. Lip (UK) and co-chaired by Jean-Philippe Collet (France), clinical routine.
Conflict of interest: GYHL: Consultant for Bayer/Janssen, BMS/ Boehringer INgelheim, Bristol Myers Squibb, Daiichi Sankyo, Pfizer,
Pfizer, Medtronic, Boehringer Ingelheim, Novartis, Verseon and Daiichi- Gregory Y.H. Lip Sanofi Aventis, The Medicines Company.
Jean-Philippe Collet (France)
20
Professor of Cardiovascular Medicine
University of Birmingham, UK ACTION Study Group Institut de Cardiologie
Sankyo. Speaker for Bayer, BMS/Pfizer, Medtronic, Boehringer E-mail: g.y.h.lip@bham.ac.uk
Price-Evans Chair of Cardiovascular Medicine
Groupe Hospitalier Pitié-Salpêtrière 47-83,
Boulevard de l'Hôpital, 75013, Paris, France.
Michael Haude (Germany)
Ingelheim, and Daiichi-Sankyo. No fees are directly received personally.
(from 1 Feb 2019)
University of Liverpool, UK
Email: gregory.lip@liverpool.ac.uk
References Tel: +33.1.42.16.29.62
Fax : +33.1.42.16.29.31
Email: michael.haude@uni-due.de
Tel: +44 121 5075080
Email: jean-philippe.collet@aphp.fr07/05/2019
TEV et cancer
■ Prévalence multipliée par 5 par rapport à population générale
■ Deuxième cause de décès chez patients avec cancer (9% des décès)
■ Mortalité multipliée par 5 par rapport à population générale
■ Impact sur le traitement du cancer
■ Hospitalisations non prévues
■ Risque élevé de récidive et de saignement sous traitement
Edoxaban for Cancer-Associated Venous Thromboembolism
Hokusai VTE cancer: récidive TEV
A
100 20
90
15
Patients with Recurrent Venous
80 Dalteparin
Thromboembolism (%)
70
10
60
Edoxaban
50
5
40
30 0
0 30 60 90 120 150 180 210 240 270 300 330 360
20
10
NEJM 2018; 378: 615-24
0
0 30 60 90 120 150 180 210 240 270 300 330 360
Days
No. at Risk
Edoxaban 522 480 437 415 395 370 356 340 320 307 281 245 168
Dalteparin 524 488 452 423 389 370 358 348 333 321 282 246 174 21Vous pouvez aussi lire