DIU oncogériatrie cancer bronchique non à petites cellules (CBNPC) stade IV
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous

THERANOSCAN
GRC-UPMC
DIU oncogériatrie
cancer bronchique non à petites cellules (CBNPC) stade IV
sans addiction oncogénique PARTIE I
Dr Armelle Lavolé
avec addiction oncogénique PARTIE II
Dr Anne-Marie Ruppert
Service de Pneumologie et d’Oncologie Thoracique
Hôpital Tenon
anne-marie.ruppert@aphp.fr
armelle.lavole@aphp.fr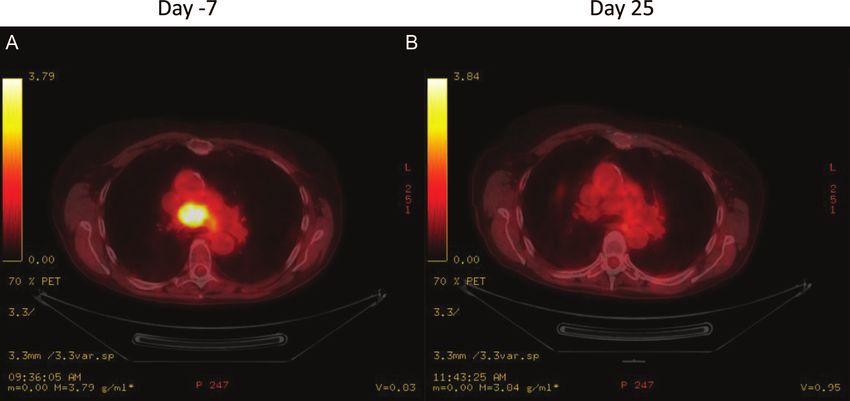
THERANOSCAN
GRC-UPMC
DIU oncogériatrie:
CBNPC de stade avancé sans addiction oncogénique
PARTIE I
Armelle Lavolé
Service de Pneumologie et d’Oncologie Thoracique
Hôpital Tenon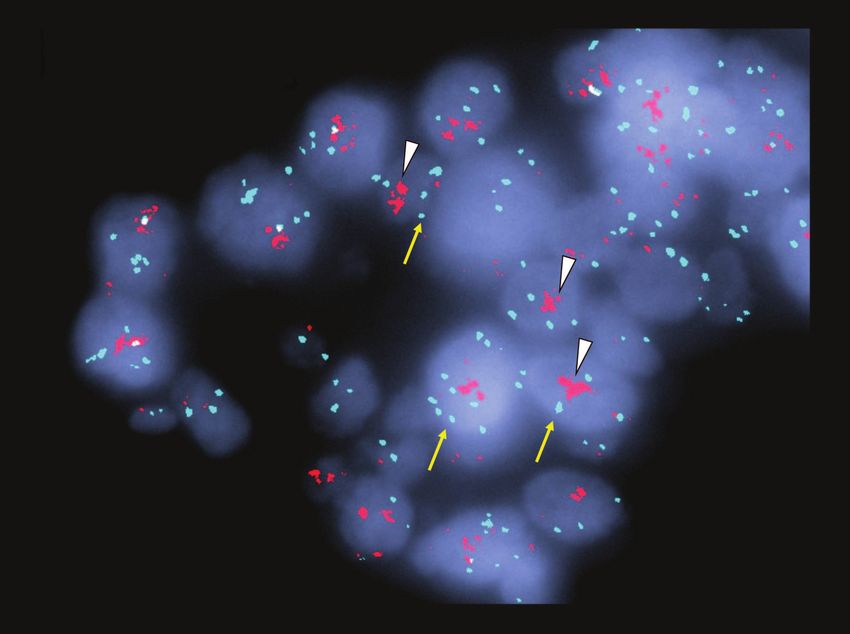
Généralités cancer du poumon • 35% > 75 ans • 14% > 80 ans • Projection 2050: >50% auront > 75 ans • Types histologiques: adénocarcinome, épidermoïde, grandes cellules • Pronostic en fonction du stade • Stade IV: médiane survie globale environ 10-12 mois
Peu d’essais dédiés chez les patients >75 ans
• Exclusion > 70 ans (30% > 65 ans)
• PS >=2
• Métastases cérébrales
• Comorbidités
• Les essais dédiés: ELDERLY, MODEL
• Sous groupes, cut off souvent à 65 ans
4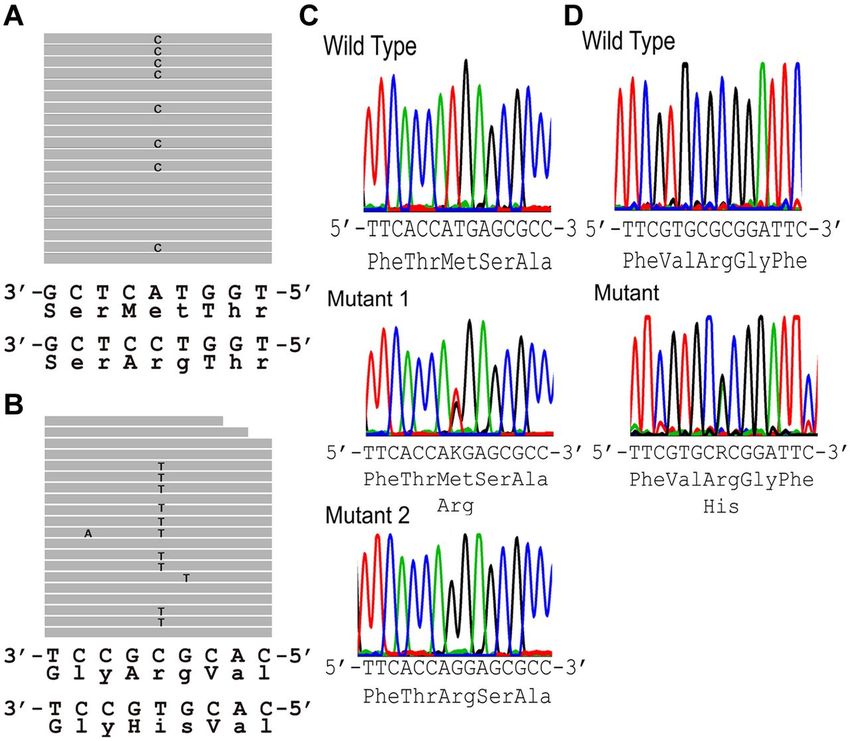
CBNPC NON EPIDERMOIDE
(ou NON FUMEUR EPIDERMOIDE mais très rare)
1ère étape incontournable: recherche d’une addiction oncogénique
28 plateformes de génétique moléculaire
5-10%; 60% si non fumeur
EGFR mutations
ROS
EML4-ALK translocations
KRAS mutations
HER2 ex20 mutations
BRAF mutations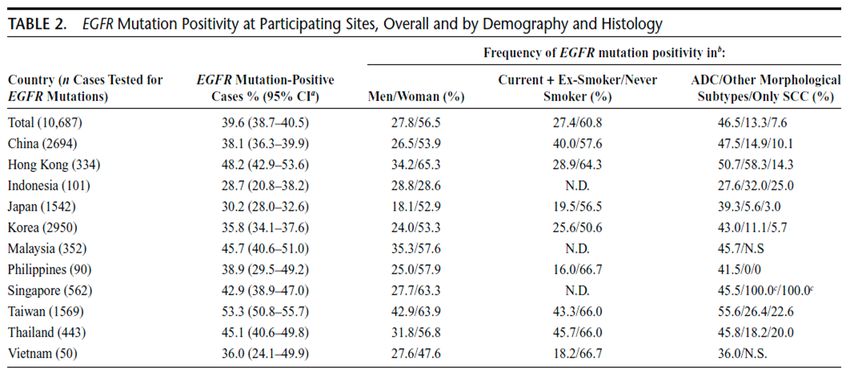
• Historique: 1990 à 2015
• 2015: le tournant de l’immunothérapie
6
Les standards de 90 à 2005
PS: 0-1 et < 75 ans , ADC et EPI
Cl > 60 et fonction VG normale
Bithérapie:
Cisplatine
Ligne 2, 3…
+ Décès
Gemcitabine Docétaxel
Pemetrexed
Taxane
Vinorelbine
SURVEILLANCE P Gemcitabine
Vinorelbine SG
4 à 6 cycles Survie sans progression Erlotinib
*carbo si PS 2/ins renale/ins cardiaque Survie globale = 8 mois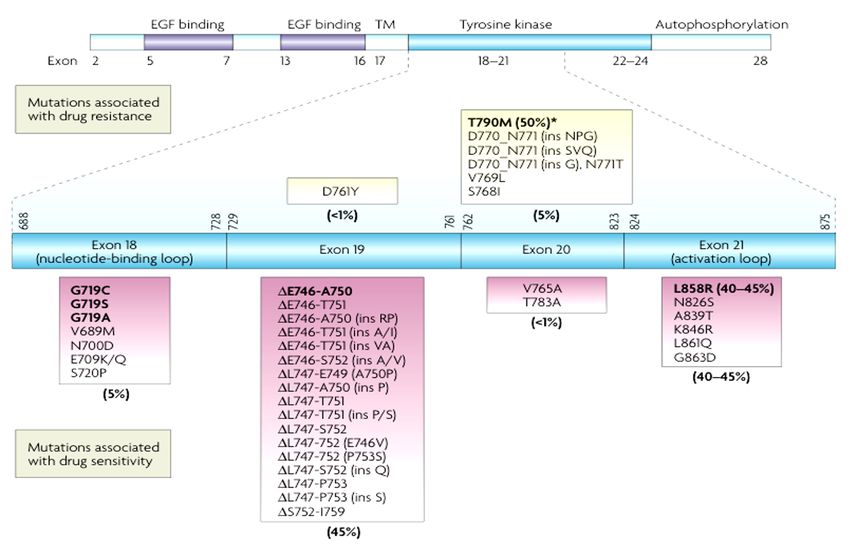
PS facteur pronostique essentiel
CHIMIOTHERAPIE
IMMUNOTHERAPIE
CHIMIOTHERAPIE?
IMMUNOTHERAPIE?
CHIMIOTHERAPIE DELETERE
SOINS DE SUPPORT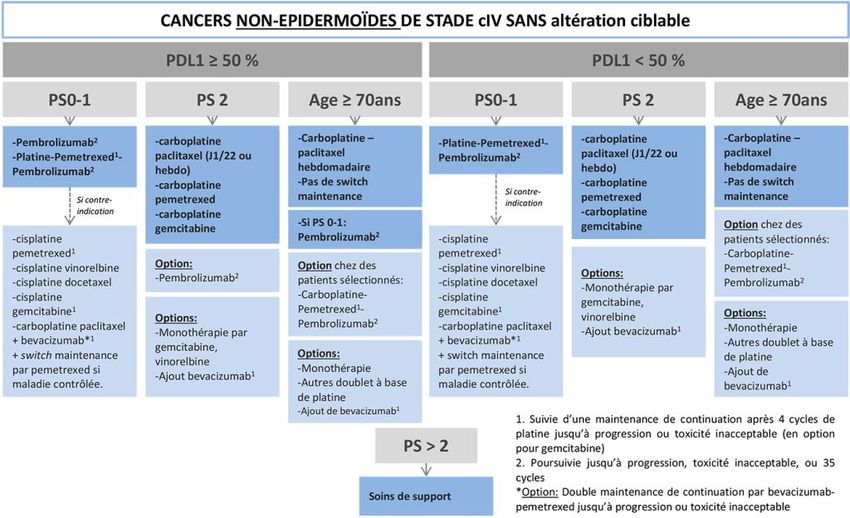
2010-2015: carcinome non épidermoïde
1/ pemetrexed associé au cisplatine
2/ bévacizumab associé à un doublet à base de platine
3/ stratégies de maintenance avec le pemetrexed (2009)
Survie globale = 12 mois
Scagliotti JCO 2008 Sandler NEJM 2006 Manegold JCO 2009
2010-2015: carcinome non épidermoïde
1/ pemetrexed associé au cisplatine
2/ bévacizumab associé à un doublet à base de platine
3/ stratégies de maintenance avec le pemetrexed (2009)
Scagliotti JCO 2008 Sandler NEJM 2006 Manegold JCO 20092010-2015: carcinome non épidermoïde
1/ pemetrexed associé au cisplatine
2/ bévacizumab associé à un doublet à base de platine
3/ stratégies de maintenance avec le pemetrexed (2009)
Scagliotti JCO 2008 Sandler NEJM 2006 Manegold JCO 2009bévacizumab *Avastin attention CI
Carboplatine
Paclitaxe (4 cycles)
ECOG
N=850
Carboplatine SG: 12,3 vs 10,3
Paclitaxel (4 cycles)
Bévacizumab 15 mg/kg jusqu’à P
Cisplatine
Gemcitabine SSP: 6,1 ms
AVAIL
N=1043 Cisplatine
Gemcitabine
SSP: 6,7 ms
Bévacizumab 7,5 et 15 mg:kg
jusqu’à P
SG identique
Sandler NEJM 2006 Manegold JCO 2009
SSP: 6,7 vs 6,1 msSujet « âgé » et bevacizumab ? Etudes de sous groupes Etude de AVAIL: > 65 ans (n=284) plus de comorbidités, plus de thrombopénie bénéfice survie globale avec 7,5 mg/kg Etude ECOG: >70 ans (n=224, 26%) Ramalingam JCO 2008 plus toxicité grade 3-5 pas de bénéfice sur la survie globale (15 mg/kg)
2010-2015: carcinome non épidermoïde
1/ pemetrexed associé au cisplatine
2/ bévacizumab associé à un doublet à base de platine
3/ stratégies de maintenance avec le pemetrexed (2009)
Scagliotti JCO 2008 Sandler NEJM 2006 Manegold JCO 2009Concept de la MAINTENANCE: continuer une chimiothérapie après l’induction à base de PLATINE
jusqu’à progression de la maladie
Platine
« STOP and GO » P produit Y
Produit X
4 à 6 cures
SG
Switch maintenance
Platine Produit Y
P
Produit X Produit
X
4 cures Maintenance « de continuation »Le pemetrexed en maintenance augmente la survie globale
dans la population générale (moyenne 65 ans)
Switch maintenance (JMEN) Maintenance « vraie » (PARAMOUNT)
• NON EPIDERMOIDE
• CBNPC
• 4 cisplatine + pemetrexed puis placebo ou pemetrexed si
• 4 Platine + gemcitabine ou taxane puis PS 0-1
placebo ou pemetrexed
16.9 mois vs 14 mois ADC
13,4 mois vs 10,6 mois
Ciuleanu, Lancet 2009; …………….Sujet âgé et première ligne?
Vinorelbine > BSC
phase III ELVIS: Elderly Lung Cancer Vinorelbine Italian study
74 ans (70-86) PS 0/1: 75%
Amélioration des symptômes
Survie à 1 an: 14% vs 32%
Neutropénie grade 3-4: 10%
Vomissements grade 2-3: 9%
Constipation grade 2-4: 18%
Alopécie grade 3: 4%
17 Gridelli C et al The Oncologist 2001Sujet âgé: bithérapie en première ligne?
4 cycles carboplatine et paclitaxel
70-89 ans hebdomadaire
PS 0-2 L2: erlotinib
n=456 patients
5 cycles gemcitabine ou vinorelbine
18 Lancet 2011, Quoix et alCaractéristiques des patients
77 ans 72% PS 0-1
85% MMSE >23
50% ADC 33% EpidermoïdeDoublet plus toxique
Grade 3-4
48% vs 12,5%
Neutropénie fébrile
9,4% vs 2,7%Doublet plus efficace: changement des pratiques 10,3 vs 6,2 mois p
Schéma
Sujet âgé et switch maintenance?
IFCT-1201 MODEL
Induction Maintenance 2ème ligne
Surveillance Prog
A
Paclitaxel – Carboplatine
Erlotinib
Inclusion
x 4 cycles R*
• CBNPC III-IV B
Non-
épidermoïde Pemetrexed Prog
• Sans addiction
• Age ≥ 70 et < 90 ans épidermoïde Gemcitabine Prog
• MMS > 23
• PS 0-2
* Patients répondeurs ou stables ERJ 2020, Quoix et alSchéma
Sujet âgé et switch maintenance?
IFCT-1201 MODEL
Induction Maintenance 2ème ligne
n=166
n=627 Surveillance Prog
A
Paclitaxel – Carboplatine
Erlotinib
R*
n=119
Inclusion
x 4 cycles
• CBNPC III-IV n=328 B
Non-
épidermoïde Pemetrexed Prog
• Sans addiction
• Age ≥ 70 et < 90 ans épidermoïde Gemcitabine Prog
• MMS > 23
• PS 0-2 n=43
* Patients répondeurs ou stables ERJ 2020, Quoix et alCaractéristiques des patients
76 ans 85% PS 0-1
64% ADC 28% Epidermoïde
24Switch maintenance plus hématotoxique
Grade 3-4
35% vs 1,2%
25Switch maintenance toxique
Asthénie
grade 3-4
12% vs 0,6%
26La switch maintenance n’augmente pas la survie globale
non recommandée chez patients de 75 ans et +
27• Historique: 1990 à 2015
• 2015: le tournant de l’immunothérapie en L2
pas d’essais dédiés, études de sous groupe
28CheckMate (PD1)la prise“Trees“
trials, nivolumabdans
L’immunothérapie and IMpower
en charge trials, atezoluzimab
du cancer du (PD-L
poumon
Recommandations
NIVOLUMAB
de traitement
ATEZOLIZUMAB
PEMBROLIZUMAB
KEYNOTE trials, pembrolizumab (PD-1) “Seas“ trials, durvalumab (PD-L1)Nivolumab en L2 et plus vs docetaxel
2015 2015
CM 017 PDL1 indifférent CM 057
mai 2015 et septembre 2015 NEJM 30Pembrolizumab en L2 vs docétaxel
PDL1 >1%
KN 010
Décembre 2015, LANCET 31Atézolizumab en L2 vs docétaxel
OAK
Décembre 2016 LANCET 32Anti PD1/PDL1 moins toxique que docetaxel
Grade 3-4 antiPD1/PDL1 contrôle
CM017 057 7% vs 55% nivolumab docetaxel
KN 010 13% vs 35% pembrolizumab docetaxel
OAK 37% vs 54% atézolizumab docetaxel
Moins toxique 33Anti PD1/PDL1 plus efficace que docetaxel PS 0-1
CM 017 CM 057 KN 010 OAK
Survie globale 34ADC, Réfractaire platine,
Apparition syndrome cave sup
Nivolumab en 12/2016 ……
12/2016
03/2021
03/2017Efficace sous groupe >65 ans, ? >75 ans
CM 057
KN 010
OAK
Faveur immunothérapie
36• Historique: 1990 à 2015
• 2017: le tournant de l’immunothérapie: L1 immunothérapie seule
37Pembrolizumab Nivolumab
comparé à une bithérapie à base de platine
PDL1 >50% 22C3 pharmDx PDL1 >5% 28-8 ab
KEYNOTE 024 CHECK MATE 026
38Pembrolizumab moins toxique que doublet à base de platine
PDL1 >=50%
Grade 3-4
26% vs 53%
Plus d’effets immunologiques
grade 3-5: 9,7% vs 0,7% 39Survie sans progression PDL1>50% meilleure dans le bras pembrolizumab
KEYNOTE 024 CHECK MATE 026
Survie sans progression 40Aussi dans le sous groupe > 65 ans
HR 0,45
41Pembrolizumab plus efficace que doublet à base de platine
PDL1 >=50%
KEYNOTE 024 CHECK MATE 026
Survie globale 42• Historique: 1990 à 2015
• 2018: le tournant de l’immunothérapie: L1 les combo
•
43Pembrolizumab et chimiothérapie en L1
KEYNOTE 189 KEYNOTE 407
44Population: PDL1 indifférent IHC 22C3pharmaDx assay, KN 189 EGFR/ALK négatifs
65 ans
PS 0-1
EGFR/ALK négatifs
PDL1 = 50%: 32%
VIH -
4 cis/carbopemetrexed+ pembro ou placebo 35 cy 4 carboplatine paclitaxel + pembro ou placebo 35 cy
puis maintenance pemetrexed + pembroou pemetrxed+ placebo maintenance pembro ou placebo
KEYNOTE 189 KEYNOTE 407 45KEYNOTE 189 NON EPIDERMOIDE KEYNOTE 407 EPIDERMOIDE Pas plus d’effets secondaires en général mais plus d’arrêts liés au tt dans le bras combo
KEYNOTE 189 NON EPIDERMOIDE KEYNOTE 407 EPIDERMOIDE
Plus d’effets secondaires immunologiques mais peu de grades sévères
47Survie sans progression augmentée dans le bras combo
KEYNOTE 189 KEYNOTE 407
48Aussi dans le sous groupe >65 ans
HR 0,63
HR 0,75
49Survie globale augmentée dans le bras combo
KEYNOTE 189 NON EPIDERMOIDE KEYNOTE 407 EPIDERMOIDE
NR vs 11,3 mois cross over 31,7%
15,9 vs 11,3 mois
cross over 41%ADC
Efficace quel que soit PDL1
KEYNOTE 189
PFS
PD-L1Aussi dans le sous groupe >65 ans
KEYNOTE 189 NONHR 0,64
EPIDERMOIDE KEYNOTE 407 EPIDERMOIDE
HR 0,74
52Un essai dédié en cours IFCT 1805 ELDERLY
53FDA: 4 essais de phase III
• toxicité 3-5 chez 70 ans et +: 71,7% vs 58,4%
• Corticoïdes EIAI chez 70 ans et +: 51,9% vs 41,5% 70 ans = toxicité et efficacité identique
Vraie vie: Felipe EJC 2020 = identique
54NON EPIDERMOIDE stade IV sans addiction oncogénique PDL1 >=50% PDL1
EPIDERMOIDE stade IV sans addiction oncogénique PDL1 >=50% PDL1
THERANOSCAN
GRC-UPMC
DIU oncogériatrie:
CBNPC de stade avancé avec addiction oncogénique
PARTIE II
Anne Marie Ruppert
Service de Pneumologie et d’Oncologie Thoracique
Hôpital TenonLa présence d’une mutation oncogénique conditionne la
première ligne dans le CBNPC
18 679 patients in 2012
+Nouveaux biomarqueurs: ROS, MET Barlesi Lancet 2016Chez qui faut-il rechercher les mutations?
2011, Asia Pacific Region survey
Lack Lack Lack
Yatabe Y, J Thorac Oncol 2015, 10:438;Comment faut-il les rechercher? IHC : ALK, ROS NGS: EGFR,MET,RAS,HER2, BRAF… FISH: MET,ALK,ROS
Les mutations de l’EGFR
> 85%
Sharma SV, Nature Reviews Cancer 2007, 7:169Femme 76 ans, non-fumeuse, toux et dyspnée,
adenocarcinome EGFR+: L1 gefitinib
21 jours plus tard
L1 erlotinib, gefitinib ou afatinib
Survie sans progression 9 à 13 moisLes mutations de l’EGFR AMM Iressa®
IPASS, Phase III
1st line, enriched population
Asian, female, non smoker, ADC
EGFR+
59.7%
EGFR-
40.3%
Mok T N Engl J Med 2009, 361:947Toxicités
• éruptions cutanées (75 %) dont grade 3/4 : 9%
àdoxycyline, hydratation cutanée
• diarrhées (54 %) dont grade 3/4 : 6%
à lopéramide
• PID, atteinte hépatique: rare
Toxicités: gefitinib < erlotinib < afatinibMécanismes de résistance acquise sous TKI EGFR
A progression, 60% des patients développement une mutation T790M de l’exon 20
d’EGFR (biopsie liquide ou biopsie du site de progression)
Yu et al. Clin Cancer Res 2013AURA 3
December 6, 2016
Phase III L2 T790M+
osimertinib 10,1 ms
• CBNPC IV EGFR +
• Progression après
TKI EGFR
• T790M+ platinum - 4,4 ms
pemetrexed
• Efficacité supérieure de l’osimertinib à un doublet à base de platine
• AMM osimertinib dans le CBNPC T790M+ après L1 TKI EGFREGFR+ ADC IV
Quel traitement en L1 en 2021?
Q
1.Cisplatin,
pemetrexed,
bevacizumab
2.Afatinib
3.Gefitinib
4.Osimertinib
5.AutresFLAURA Phase III L1
CBNPC IV* osimertinib
Exon 19
Cross over si T790M
18,9 ms
deletion/L858
R
Erlotinib ou
L1 10,2 ms
gefitinib
*Asymptomatic brain
metastasis included
Soria et al January 11, 2018Osimertinib sujets âgés L2 T790M+
Phase II en L2 T790M+ :
• Inclusion de 36 patients, âge 79,9 ans
Objectif principal:
taux de réponse 58,8%
temps à progression 27,8 semaines
Objectif secondaire: toxicité
Nakao A, The Oncologists 2019Quel stratégie en 2021 pour les CBNPC mutés
EGFR?
Mécanismes de résistance?
L1 Osimertinib Chimiothérapie?
18,9 ms
Gefitinib
L1 Erlotinib T790M+ L2 Osimertinib Mécanismes de résistance?
Afatinib
9-13 ms 10,1 ms
Survie globale?Réarrangement
n e w e ng l a n d j ode
The u r naALK
l m e dic i n e of
FISH: standard
IHC: hyperexpression
A B
C D
EML4 exon 6b ALK exon 20
A A A A A A C A G C C A A G T G T A C C G C C GG
Figure 1. Diagnosis of an EML4-ALK–Positive Non–Small-Cell Lung Cancer in a Single Representative Patient.
C D
Panel A shows the results of a break-apart fluorescence in situ hybridization assay of tumor cells from a patient with
AUTHOR:
rearrangement of the gene encoding Kwak
anaplastic lymphoma kinase (ALK). RETAKE: 1st probe hybridizes to the region
The greenex F, 35 ans, CBNPC ALK+
Crizotinib CBNPC ALK+
PROFILE 1014
2 mois après
Solomon BJ, et al. N Engl J Med 2014Quel traitement à progression?
ASCEND-5
Ceritinib, 5,4 ms
Chemotherapy, 1,6 ms
Shaw Lancet Oncol 2017
Ceritinib phase II
Alectinib
Shaw Lancet Oncol 2016
Alectinib phase II
Alectinib
JCO 2016
Plusieurs inhibiteurs d’ALK de 2ième generation ont prouvé leur efficacité; Ceritinib et
alectinib, ont une AMM après progression sous crizotinibBrigatinib en L2 après crizotinib Lorlatinib en L2 après crizotinib
Brigatinib et lorlatinib : options thérapeutiques
A T.Shaw and al. Lancet Oncol 2017 Dong-Wan KIM and al. JCO 2017Q
ALK+ CBNPC stade IV
Quel traitement en L1 en 2021?
1.Chimiothérapie
2.Brigatinib
3.Alectinib
4.Ceritinib
5.LorlatinibALEX
Alectinib en 1ière L:? OUI
Alectinib, 25,7 ms not reached
Crizotinib, 10,4 months
Essai ALEX : SSP alectinib > crizotinib, et moindre toxicité
S. Peters and al. NEJM 2017AMM AMM Pas de prix Pas d’AMM
Quel stratégie en 2020 pour les CBNPC ALK+?
L1 Alectinib
Mechanismes de résistance ?
Crizotinib Ceritinib Ceritinib
L1 L2
Alectinib L3? Alectinib
Brigatinib Brigatinib
Lorlatinib Lorlatinib
Survie globale?
Gainor, Shaw Cancer discov Oct 201730 ans, Non fumeuse, ROS 1+
Réarrangement ROS 1 1% of NSCLC
Diagnosis: FISH
Traitement standard L1 : crizotinib
Shaw, NEJM 2015Réarrangements ROS 1 : crizotinib
78% Non fumeurs, 56% femmes, âge médian
53 ans, 86% >= 1 pré ttt
Best response N = 50
ORR, n (%) 36 (72%)
CR, n (%) 3 (6)
PR, n (%) 33 (66)
SD, n (%) 9 (18)
DCR, n (%) 45 (90%)
DOR, median (95% CI), mo 17.6 (14.5–NR)
PFS, median (95% CI), mo 19.2 (14.4–NR)
OS, median (95% CI), mo 12.7 (7.3–16.9)
Shaw, NEJM 2015autres ITKs active CBNPC ROS 1
Entrectinib
53 pts crizotinib naif
ORR 77%,
PFS médiane 24,6 m
Ceritinib
Pas d’AMM
30/32 pts crizotinib naif
ORR 62%
PFS médiane 9,3m
Lorlatinib
21/69 pts crizotinib naif
ORR 62% naive et 35% préttt
PFS médiane 25,3 vs 13,8
Cabozantinib, alectinib: études en cours
Lim JCO 2017, Shaw Lancet Oncol 2019, Drilon Cancer Disc 201771 ans, 4 PA ADC stade IV diagnostiqué en 2015 Mutations (ras - braf - 1EGFR - erbB2 - PIK3CA - ; % cellules tumorales 5%) IHC ros 1 -, cmet 2+, ALK2 1+ FISH met -, FISH ALK – L1: cisplatine pemetrexed bevacizumab 3 Pleuroscopie: pas de mutation - % cellules tumorales 30%
L2: nivolumab (11/2015-01/2017) 4 Adenopathies axillaires Cytoponction: % cellules tumorales 30% Pas de mutation L3: docetaxel (02-2017 -08/2017)
8/2017, gynécomastie, douleurs abdominales
cytoponction mammaire :adenocarcinoma TTF1 +
ras - braf + V600 E EGFR - erbB2 - PIK3CA - ; % cellules tumorales
80%
ros 1 - ALK - met - PD L1 > 50%
5Mutations Braf : 3% CBNPC 50% mutations V600 E (non fumeurs) mutuellement exclusive des mutations EGFR ou réarrangements ALK ou ROS 1
Phase II BRAF V600E:
trametinib - dabrafenib
Patients prétraités Patients naifs
CR 3,5% CR 6%
PR 60% PR 58%
DCR 79% DCR 75%
Planchard Lancet Oncol 2016/2017Phase II BRAF V600E:
trametinib and dabrafenib
Patients pré-traités Patients naifs
SSP 9,7 mois SSP 10,9 mois
Planchard Lancet Oncol 2016/20179/2017, traitement dabrafenib - trametinib Début traitement à 6 mois
eligibility criteria for enrollment in the MET-enriched molec- starting crizotinib revealed a dramatic 49.3% decrease in
ular cohort of the A8081001 trial (required to have MET SUVmax from baseline (Figures 2A, B) with a corresponding
mutations or MET amplification) (MET/CEP7 ratio !2.2; not 35.7% decrease in the maximum aggregate tumor measure-
MET
twice a day (the recommended phase II dose) in late May MET
polysomy). The patient started crizotinib 250 mg by mouth ment by RECIST (version 1.1) (Figures 3A, B). A follow-up
8-week PET/CT revealed continual response to crizotinib
2010. Her symptoms before starting crizotinib included per- with a 67.6% decrease in the SUVmax from baseline with a
sistent cough, fatigue, and chest tightness. Within a week of corresponding 45.2% decrease in tumor measurement by
IHCcrizotinib,
starting ne permet her pas
coughdedisappeared
sélectionner lesfatigue
and her amplifications
RECIST ou mutations
(version 1.1). She achieved maximum reduction in
aggregate tumor measurement of 54.8% on September 2010,
and she continues on study with partial response. The only
side effect attributed to crizotinib experienced by the patient
was asymptomatic grade 1 sinus bradycardia and transient
grade 1 visual disturbances characterized by intermittent
flashing lights in the peripheral visual fields. Follow-up visual
acuity and slit-lamp examination revealed no specific retinal
abnormality.
Criteria Determining MET Amplification in
A8081001 Trial
The MET copy number was determined by laboratory-
developed test using a bacterial artificial chromosome probe
containing MET sequence (CTB-13N12) labeled in Spectru-
mOrange and a commercial centromere 7 probe (Vysis/
Abbott Molecular, IL) labeled in SpectrumGreen. Five-mi-
cron sections of formalin-fixed paraffin-embedded tumor
material were prepared and an hematoxylin and eosin section
FIGURE 1. Mesenchymal-epithelial transition (MET) amplifi-
reviewed to select regions for hybridization that contained a
cation byAmplification de MET
fluorescence in situ (Techniques
hybridization (FISH).Fish)
Tumor Mutations
majority ofde METcells.
tumor (Sanger, NGSspecimen,
For each ..) individual cell
cells showResistance aux TKI EGFR ou de novo by a red
cluster of MET amplified loci represented MET and
CBNPC CEP7
plutôt signals
sous typewere analyzed in a total of 50 tumor
sarcomatoide
aggregate (white arrow). The CEP7 chromosome is repre- cells. FISH-positive groups include (1) high-level amplifica-
sented by a single blue dot (yellow arrow). Nuclei stained tion (presence of loose or tight clusters of MET signals too
with 4=,6-diamidino-2-phenylindole. numerous to count) or a MET/CEP7 ratio more than 5.0 andPhase II MET :crizotinib
Crizotinib dans les CBNPC programme ACSE
Mutation exon 14
Amplification Met
Drilon A. et al.- ASCO® 2016 - Abs 108 Moro-Sibilot Annals of Oncology 2019Capmatinib
28/69 pts crizotinib naif
ORR 68% naive et 40% préttt
PFS médiane 25,3 vs 13,8
Wolf J NEJM 2020KRAS G12C
Ruppert AM, JTO CCR 2020Phase I-II KRAS G12C :sotorasib
ATU sotorasib en L2 CBNPC G12C
Hong DS J NEJM 2020Options thérapeutiques dans les CBNPC mutés
PDL 1
Oncogenic driver
TEST
EGFR ALK ROS1 BRAF KRAS G12C MET
Alectinib
1L Osimertinib Ou Crizotinib Chimio immuno Chimio immuno Chimio immuno
Brigantinib
Selon le Selon le
2L mécanisme mécanisme Entrectinib Dabrafenib Sotorasib ATU
Capmatinib ATU
(Crizotinib)
de résistance de résistance ATU Trametinib
Chimio
Chimio Ceritinib
Afatinib Alectinib
… Lorlatinib
BrigatinibVous pouvez aussi lire