Pathologies constitutionnelles de la membrane érythrocytaire - Loïc Garçon - OVH.net
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous
Pathologies constitutionnelles
de la membrane érythrocytaire
Loïc Garçon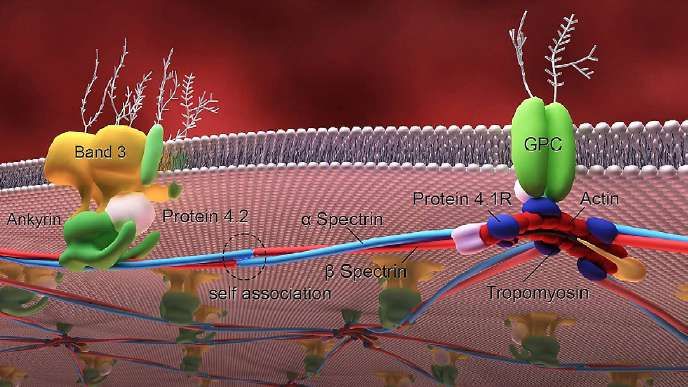
Ratio Surface/volume
La déformabilité : qualité essen4elle
Produc'on énergé'que
Chen L and Weiss L, Blood, 1973, 41 (4)
Viscosité interne du globule rouge
Viscoélasticité membranaire
Le réseau protéique sous-
membranaire
• Recouvre 65% de la surface cytoplasmique de la
double couche lipidique
• Est relié à la double couche lipidique par des
complexes protéiques transmembranaires
• Structure complexe multiprotéique composée de
protéines transmembranaires et de protéines sous-
membranaires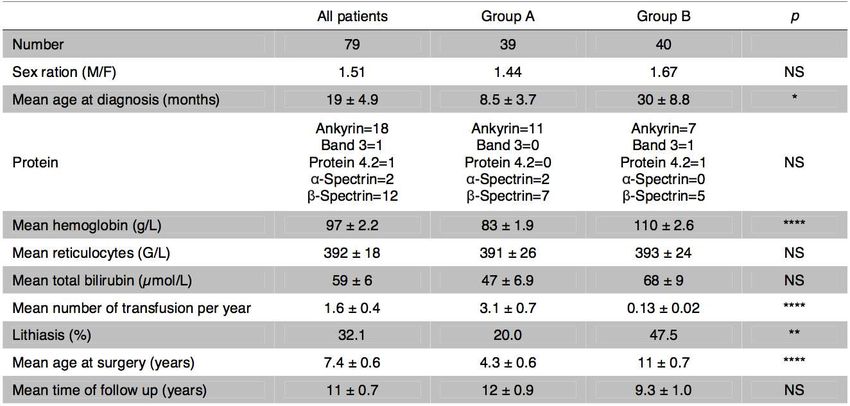
Bijleveld R et al , NJM, 2015

Les pathologies membranaires
cons2tu2onnelles
• Altération des interactions horizontales: donc
de l’élasticité érythrocytaire: Elliptocytoses
héréditaires
• Altération des interactions verticales, donc de
la STABILITE membranaire: diminution du
rapport surface/volume: sphérocytoses
héréditaires
• Altération de l’hydratation érythrocytaire:
Stomatocytoses héréditaires (hyperhydratées
et deshydratées)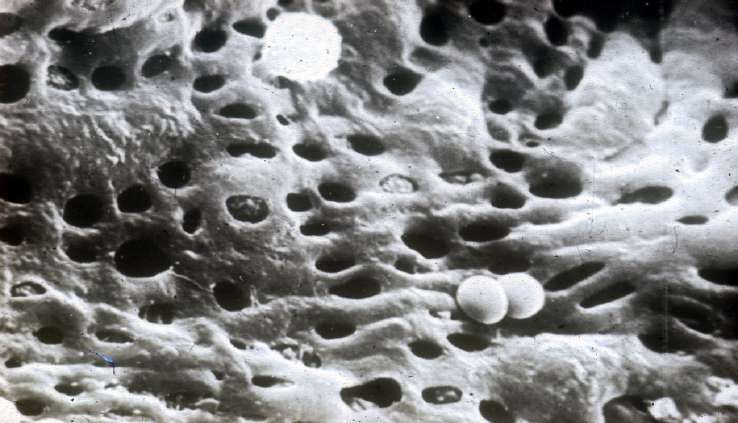
Anomalies des interactions verticales: sphérocytose héréditaire
- 1/2000 naissances en Europe et Amérique du Nord
- 1% des explorations d’INN (V. Saada et al, Pediatr Hematol Oncol. 2006)
- Dominant 75% des cas
Perro]a S et al., Lancet, 2008, 372:1411-26
Bande 3
Gène SLC4AE1(17q)
30% population caucasienne
Dominant
Protéine 4.2
Gène EPB42
50 % au Japon
Récessive
Ankyrine
Gène ANK1 (8p)
40-65% population caucasienne
Dominant (80%) ou de novo (20%)
Déficit combiné en spectrine
Spectrine α Spectrine β
Gène SPTA(1q) Gène SPTB(14q)
5% population caucasienne 20% population caucasienne
Récessive, sévère Dominant ou de novo
Peut-être associée à des polymorphismes α-LEPRA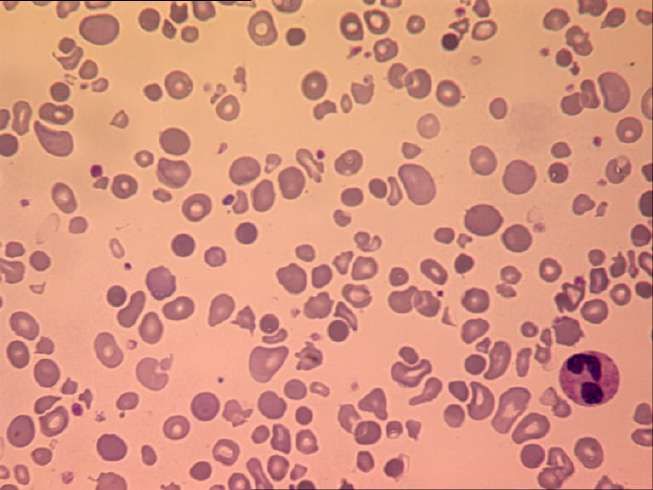
Physiopathologie
Spectrin, ankyrin, or
protein 4.2 deficiency
Spectrin, ankyrin, or Low pH
Spectrin, ankyrin, or High macrophage
protein 4.2 deficiency
protein 4.2 deficiency contact
Release of microvesicles Low pH
Low pH H
Highglucose
macrophage
Déstabilisation de la Highbi-couche
macrophage Lowlipidique
contact
Release of microvesicles concentration
Release of microvesicles
Spectrin, ankyrin, or Vésiculation deErythrostasis
la membrane
contact
High oxidants
Low glucose
Haemolysis
H
protein 4.2 deficiency Low glucose concentration
concentration
concentration Low pH
Erythrostasis High oxidantsHigh macro
Déficit en Spectrine, Erythrostasis High oxidants
concentration
Reduced Reduced
Release of microvesicles Splenic
concentration Splenic contact Fu
Ankyrinesurface-to-volume
ou 4.2 ratio cellular deformability trapping conditioning Low glucose
of
Reduced Reduced Splenic Splenic concentratiF
Reduced Reduced Splenic Splenic Further loss
High oxidan
surface-to-volume ratio cellular deformability trapping conditioning of
surface-to-volume ratio cellular deformability trapping conditioning Erythrostasis
of membrane
concentrati
Reduced Reduced Splenic Splenic
surface-to-volume ratio cellular deformability trapping conditionin
Release of microvesicles Liu, Derick, Agre and Palek, 1990
Tail of osmotic
Release of microvesicles
Déficit Release
endeficiency
Bande 3 of microvesicles fragility curve
Band-3
Lipid bilayer Tail of osmotic
Spectrin Tail of osmotic
Ankyrin Band-3 deficiency Perte de Release
surface,offragilityvolume
curve
microvesicles constant
fragility curve
Band-3 deficiency
Lipid bilayer
Lipid bilayer Band 3
Défaut d’interactions verticales
Spectrin Diminution ratio S/V Tail of osmotic
Spectrin
Ankyrin fragility curve
Ankyrin membrane - cytosquelette Band-3 deficiency
Band 3 Lipid bilayer
Band 3Figure 2: Pathophysiological effects of hereditary spherocytosis è Sphérisation du GR
Spectrin21
Modified from Gallagher and colleagues with permission.
Ankyrin
Figure 2: Pathophysiological effects of 3 hereditary spherocytosis
Moindre déformabilité
ure 2: Pathophysiological effects of hereditaryBand
spherocytosis
apparent
Modified fromin the homozygous
Gallagher and colleagues21 orwithcompound
permission. heterozygous described.46,47 ANK1 gene deletion might be
odified from Gallagher and colleagues21 with permission.
state. These patients Figure 2:have severe disease.
Pathophysiological Homozygous
effects of hereditary spherocytosis contiguous gene syndrome with manifes
apparent
pparent in and in
compound
the homozygous
D’après
the homozygous
S. Pero.a, or heterozygous
compound
Modifi ed
Lancet from
2008
or compound
defects have
heterozygous
Gallagher and colleagues heterozygous
with described.
permission.
21 described.
46,47
ANK1 geneANK1
been spherocytosis,
46,47
mentalgene
deletion deletion
retardation,
might might
be part of be
typical
a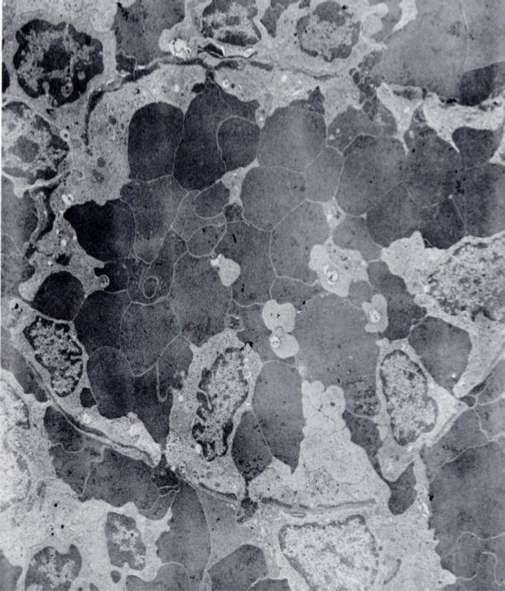
Low glucose
concentration
Erythrostasis High oxidants D’après S. Perotta, Lancet 2008
concentration
Reduced Reduced Splenic Splenic Further loss
Séquestration cordons spléniques
surface-to-volume ratio « Conditionnement
conditioning splénique
cellular deformability trapping of membrane»
ê pH
êGlucose
Release of microvesicles é Oxydants
êATP Tail of osmotic
fragility curve
Band-3 deficiency
Lipid bilayer
Spectrin
é contact avec macrophages
Ankyrin
Band 3
2: Pathophysiological effects of hereditary spherocytosis
fied from Gallagher and colleagues21 with permission.
arent in the homozygous or compound heterozygous described.46,47 ANK1 gene deletion might be part of a
e. These patients have severe disease. Homozygous contiguous gene syndrome with manifestations of
compound heterozygous defects have been spherocytosis, mental retardation, typical faces, and
ciated with null mutations and variants are hypogonadism.
ciated with low-expression alleles.33–36 For example, Ankyrin-1 plays a pivotal role in the stabilisation of the
α-LEPRA (low-expression allele Prague) allele membrane, providing the main membrane binding site
duces about six-fold less of the correctly spliced for the spectrin-based membrane skeleton. Since it links
ectrin transcript than does the healthy allele.33 The β spectrin to band 3, ankyrin deficiency leads to a
ence of two null α-spectrin alleles is speculated to proportional reduction in spectrin assembly on the
ethal. Blood smears from patients with severe membrane despite normal spectrin synthesis.48 The
ectrin deficiency contain many microspherocytes, deficiency of one protein is strictly associated with the
racted erythrocytes, and abnormal poikilocytes deficiency of the other and the extent of protein deficiency
e 2).24,33 is related to the clinical severity. A high reticulocyte count
he biochemical phenotype of combined spectrin and might mask a reduction Molnar Z.inand
ankyrin-1
Rappaportin biochemical
H, Blood, 1972, 39 (81-98)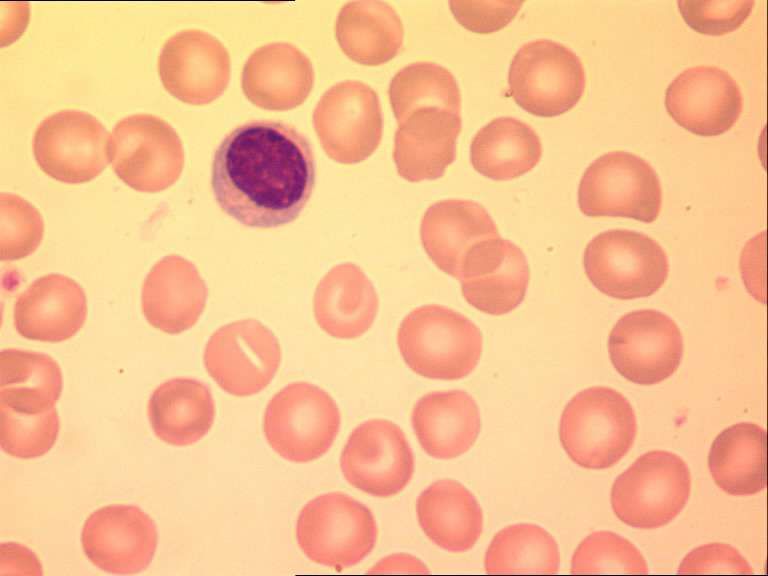
Sévérité et Mineures Modérées Modérément Sévères
fréquence 30% 60-70% sévères 10% 3-5%
Hb N > 8 g/dl 6 – 8 g/dl < 6 g/dl
Réticulocytes 6% > 10 %
Bilirubine 17 - 34 μmol/l 34-51 μmol/l > 51 μmol/l
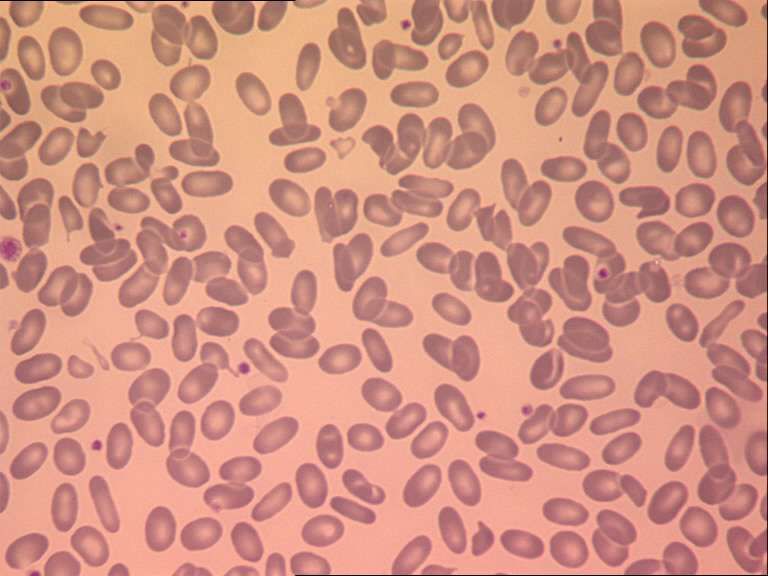
Frottis Microsphérocytes
Sphérocytes
sanguin et poikilocytose
Dépendance
Transfusions 0-1 2 >2
transfusionnelle
Transmission AD AD, de novo AR
Ankyrine
β-spectrine
α-spectrine
Bande 3 formes hétérozygotes formes homozygotes
D’après S. Perotta, Lancet 2008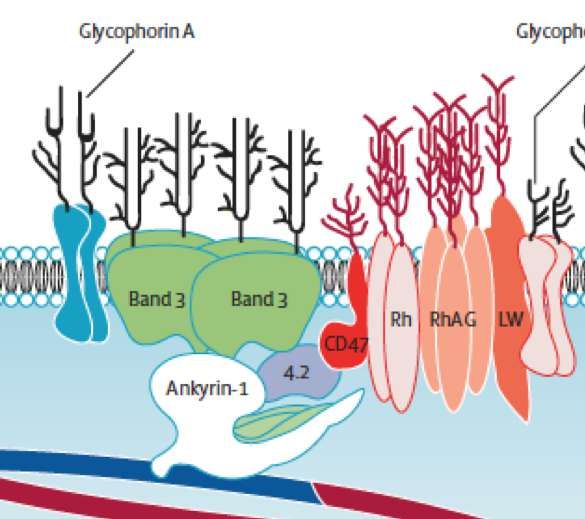
Sphérocytose Héréditaire
Formes particulières
Delhommeau F et al, Blood, 2000
- Formes néonatales
-Formes sévères
-Bande 3 homozygote
- Mutations nulles
- Parfois associées à des acidoses tubulaires distales
-Formes récessives
- Homozygotie/hétérozygote composites pour des mutations SPTA
-Facteurs associés modulant le phénotype clinique
-AssociaBon trait AS et de SH: risque d’infarctus splénique.Frottis cytologique
Non spécifiques
- AH immulogiques
- CDA II
- Hémolyses mécaniques
- PPH
- Choc thermique
-Toxiques (venins), stress oxydatif aigu
-Hypophosphatémie, intoxication au zinc
-In vitro, sang vieilli
Mariani et al, Haematologica, 2008Indices érythrocytaires Valeur diagnostique dans les SH
Cynober T et al, Int J of Lab Hematol, 1996,
>4% CHD:
Meilleur discriminateur:
Sévérité
-100% SH
-0% des contrôles
60fL 120fL 28g/dL 41g/dLTests de confirmation
-Test de résistance osmotique (Parpart et al, 1947)
- Avantages: Large utilisation
-Inconvénients: manque de sensibilité, nécessité de témoins adaptés Dépendent
S:V
-Pink Test (Test de lyse in vitro)/AGLT (Zanella et al, 1980; Bucx et al, 1988)
- Avantages: Simplicité, peu de volume sanguin, sensibilité (96%)
-Inconvénients: spécificité variable
-Test de cryohémolyse (Streichman et Gescheidt, 1998)
-Explore les propriétés mécaniques des SH
-Sensibilité variable : seulement 53% dans une étude (Mariani et al, 2008)
-Cytométrie de flux: marquage au 3’EMA (King et al, 2000)
- Ektacytométrie (Bessis et al, 1975)
- SDS-PAGECytométrie en flux:
Marquage à l’éosine 5-maleimide (EMA)
M.J. King et al, Bri0sh Journal of Haematology, 2000, 111, 924–933.
Interac0on prédominante entre EMA et certaines protéines de la membrane érythrocytaire: Bande 3
(80%) et protéines du groupe Rhésus (CD47, RhAG, Rh proteins)
-Kar R et al, Int Journal of Lab Hematol, 2008
Série de 200 pa0ents dont 20 HS, 20 probables, 20 AHAI, 20 contrôles
- Sensibilité: 96.4%
- Faux posi0fs dans 3 AHAI et un CDA II
- Spécificité:94.2%
-Stoya et al, 2006
- Sensibilité 96%
- Spécificité 99%
-King MJ et al, Bri0sh Journal of Haematology,
Série de 174 pa0ents
- Sensibilité 93%
- Spécificité 99%
- Faux posi0fs
- CDAII
- Pas dans 8 AHAIEktacytométrie
(M Bessis et N Mohandas, Blood cells 1975 ; 1 : 307-13)
Laser
Echantillon
Index de déformabilité (ID) = grand axe - petit axe
grand axe + petit axePoint hypo: déformabilité nulle ID max
en milieu hypoosmolaire Milieu isoosmolaire Point hyper:
Correspond à la fragilité osmo;ique DEPEND de S mesuré en milieu hyperosmolaire
DEPEND DU RAPPORT S:V CONSTANT DANS HS Reflet de l’état d’hydratation érythrocytaire
Osmolarité croissanteSDS PAGE: électrophorèse des protéines de membrane
Diagnos;c posi;f Diagnostic differentiel
P T P T
Sensibilité variable+++,
En général 70-80%
Spécificité
P P T
Aspect qualitatif :
anomalie de migration de la Band 3
Dr Ghazal, CHU Bicêtre dans les CDA IIMadame M.
Adressée à 21 ans pour anémie:
• Splenomégalie
• Ictère
• Lthiase biliaire asymptoma?que
• Transfusée à deux reprises:
• FCS
• Grossesse
Adressée à 21 ans pour anémie:
• Hb= 9g/dL
• Réticulocytes= 160 G/L
• Plaquettes et leucocytes normaux
• LDH élevée, haptoglobine effondrée,
bilirubine libre à 25 µmol/LUn exemple de diagnostic différentiel
- Test de Coombs négatif
- Pas d’autres causes extra-
corpusculaires
- Pas d’HPN
- Pas d’hémoglobinopathie, de
déficit enzymatique…
• Ektacytométrie: « courbe
subnormale, mais diminution de
l’index de déformabilité et
résistance globulaire un peu
diminuée »
Sphérocytes
Sphérocytose héréditaire?Myélogramme
Prise en charge thérapeu0que Recommendations regarding splenectomy in hereditary hemolytic anemias, Haematologica, Aug 2017, Working Group on Red Cells and iron,
Indications de la splénectomie
FORMELLE :
formes sévères POSSIBLE :
et modérément sévères formes modérées
Dépendance NON INDIQUEE :
Retentissement sur qualité de
transfusionnelle formes mineures
vie :
Asymptomatiques
ê performances scolaires
Splénomégalie douloureuse
Ictère marqué
Après 5-6 ans ++ Laparoscopie > Laparotomie
Risque infectieux Complications post-opératoires
Durée d’hospitalisation
Place de la splénectomie
Durée de convalescence
subtotale avant 5 ansSplénectomie subtotale • But : – Surseoir à splénectomie totale – Moindre risque infectieux • Mais : – « Repousse » splénique – Persistance hémolyse de fond
Suivi à long terme après splénectomie subtotale
Pincez, Guitton et al. Blood 2016
Formes sévères Formes modéréesRéponse hématologique
•90% réponse
•8 rechutes
Rate fonctionnelle ≥ 1 an : 96%
îî besoins transfusionnels
Pincez, Guitton et al. Blood 2016Repousse splénique
•volume x 5
Totalisation splénectomie
•20 patients (25%)
•8.4 1,2 ans après SST
Groupe A :
•17 patients (47%)
•dont 8 rechutes
Groupe B :
•3 patients (8%)
Pincez, Guitton et al. Blood 2016Intérêt de la Splenectomie Sub-Totale
Groupe A (formes sévères) Groupe B (formes modérées)
•îîî besoins transfusionnels •Evite splénectomie totale pour
•8 rechutes nécessitant formes peu sévères
totalisation
•Mais âge > 5-6ans (hors risque
infectieux)
è Candidats idéaux à SST
MAIS :
•Persistance hémolyse à bas bruit
•Lithiases chez 16/46 patients non cholecystectomisés
•43% groupe A vs. 15% groupe B ; p=0.04Anomalies de l’hydratation « Stomatocytoses »
Régulation de l’hydratation érythocytaire (dire
primitif ou secondaire: F
Regula'on du volume érythocytaie et CCMH: essen'el
- Déformabilité
- viscosité interne
Teneur en hémoglobine Eau et contenu solublePseudo-hyperkaliémie familiale
(PHF)
Mutations HTZ le plus souvent du gène ABCB6 (Antigène Lan)
Screening de 327 dons de sang:
La mutation la plus fréquente R276W: 0,3%
Andolfo et al Haematologica, 2016Stomatocytoses à cellules hyperhydratées:
OHSt
Entrée ++++ du Na+, sor0e plus modérée du K+
Entrée d’H2O: HYPERHYDRATATION
Autosomique dominante ou mutations de novo Indices érythocytaires (ADVIA 2120)
Rares++
Petite série de 4 cas (CHU Bicêtre):
-Hb: 10.7 g/dL
-VGM 129 fL
-CCMH 24%,
-Réticulocytose 11%
60fL 120 fl 28 41
Volume ChromieFro$s sanguin: très nombreux stomatocytes
OSMOTIC GRADIENT EKTACYTOMETRY SDS-PAGE
Dr Picard Dr Fénéant-Thibaut
DI (CHU Bicêtre) (CHU Bicêtre)
Control
0.40
0.20
Omin O’
OHSt
0.40
0.20
200 300 400Perrotta S et al., Lancet, 2008, 372:1411-26
Dehydrated Hereditary Stomatocytosis
DHSt (OMIM #194380 )
Autosomal dominant Red Cell Indices
K leak, barely balanced and Na+ entrance
+
60 120 fl
31 Pa:ents (CHU Bicêtre) Volume
-Hb: 137 g/L
-MCV 99 fL
-CCMH 36.7%
-Ré:culocytes 7% Chromia
-StomatocytesPleiotropic syndrom associated with DHSt
S. Grootenboer et al., Blood 2000 ; 96 : 2599-2605
DHSt Pseudo
hyperkalemia
Perinatal
Edema
Hyperferritinemia
Not transfusion related
Lead to 0ssular complica0ons
Can reveal the diseaseIndications of Ektacytometry
n= 103, 49 families
Chronic
hemolysis
29%
Familial
screening
52%
Thrombotic events
(8%)
Perinatal oedema
6%
Iron overload
5%Clinical and Biological features
Familial tes6ng
N=54
80
70
60
% des patients
50
40
30
20
10
0
NSCH
NSCH Thrombosis
Thrombosis Perinatal
PO Hyperferritinemia
Hyperferritinemia
OedemaAge at HX diagnosis
16
14
12
Number of patients
10
8 15
14 14 13
6 11
4 8 8
2 5
0
160 9
90
80
70
60
Mean Age
50
40
30
20
10
0
NSCH PO 1 Hyper Thrombosis
ferritinemiaHematological features at diagnosis
18 120 450
16 400
100
14 350
12 80 300
Most of the times,
10 250
HX induces a
60
8 200
compensated
13,5
98,9
hemolysis
6 40 150
252
4 100
20
2 50
0 0 0
Hemoglobin
1 MCV
1 Reticulocytes
1
(g/L) (fL) (G/L)Other biological / clinical features
P50 evaluation Hyperferritinemia
(Dr Kiger- Dr Picard, e-poster 1082) n=55
No transfusion dependant anemia
Absent Present
53% 47%
14 by phlebotomy
6 by DFO
6 by DFX
1 by DFPPerinatal edema
17 (13 families)
Mostly from the 2nd trimester
Hydrops fetalis: 66% of patients
2 MFIU - 1 IMG – 1 death early after birth
40 % prematurity (half before 32 SA)
Transfusion in Utéro : 30 % of patients (Hb 7,1 g/dL – 19,1 g/dL)
Favorable outcome in less than 1 month in 50 % of patients
NO RELAPSE except 1 patient with lymphoedema at adult age17 thrombotic events 12 patients with thrombotic events
120
2 100
4 Non
Pulmonary
Embolie embolism
pulmonaire
splenectomized
2 PVT
TVP 80
Thrombose
Portal thrombosis
porte
AVC 60
Cerebral stroke
2
3 HTAP
Pulmonary hypertension Splenectomized
40 83%
Infarctus splénique
Spleen infarct
4 20
0
1
11 Patients were splenectomized
-Mean Age at splenectomy: 23,6 (10-41 yo)
-10/11 Patients experienced thrombotic events
-Mean delay of thrombotic events after splenectomy:
9 years (14 days-27 years)Force mécanique
Piezo1 est exprimé à la membrane du GR
(Andolfo et al, Blood, 2012)
. Bagriantsev et al.. 2014
ìCa2+
Mutations « gain de fonction »
(Albuisson et al, Nat Com, 2013)
Gardos channel KcL cotransporteur
Fuite cationique
Deshydratation
Rôle dans d’autres pathologies érythrocytaires?
PSickle? (Gallagher et al, 2014)CONCLUSION
-Pathologies rares
-Y penser à tout âge!
-Autosomique dominante
-Modes de présentation inhabituelle (hémochromatose...)
-Hémolyse compensée fréquente
-Diagnostic à éliminer avant toute splénectomie
-Frottis
-Indices érythrocytaires
-Ektacytométrie
-Biologie moléculaire
RISQUE TRHOMBOTIQUE MAJEUR APRES SPLENECTOMIEAnomalies des interactions horizontales:
Elliptocytose héréditaire
Bijleveld R et al , NJM, 2015Anomalies des interactions horizontales:
Elliptocytose héréditaire
Anomalie membranaire avec présence de 20 à 100% d’elliptocytes
Transmission autosomique dominante
Prévalence : 1-2% dans certaines régions d’Afrique et aux Antilles, 15 à 20 fois plus rare en Europe.
HPP
HE
-Mutations SPTA1: 75% des cas
-La plupart des mutations sont dans la partie N-ter de la spectrine alpha,
-Altérant les sites d’oligomérisation
-Mutations 4.1: 4.1 (-) HE N-ter C-ter
-- Nombreux elliptocytes (100%)
-Asymtomatique à l’état hétérozygote
-Mutations SPTB
-Rares Site d’autoassociation Site joncJonel
-- Parfois très symptomatiques meme à l’état HTZ
Localisées en général dans la région C-terminaleElliptocytose héréditaire simple (HE)
-90% des cas
-Asymptomatique jusqu’à hémolyse très modérée
-Ex: (4.1)- HE; mutations SPTA1
-Diagnostic sur frottis sanguin
TémoinPyropoïkilocytose héréditaire (PPH)
-Tableau d’anémie hémolytique parfois sévère, transfusion dépendant
PPH
- Mutations SPTB
- Forme homozygote (4.1R)
-Hétérozygote composite SPTA1
King MJ et al, ICSH Guidelines, 2015)Enzymes érythrocytaires
Le métabolisme du globule est anaérobie:
-Absence de noyaux
-Absence de mitochondrie
-Shunt de Rappaport (1):
Production de 2.3 DPG èlibère O2 aux tissus
- Glycolyse anaérobie (2):
Production d’énergie (90% de l’ATP de la cellule)
et du NADH
- Voie des Pentoses-Phosphates (3):
Production du pouvoir réducteur NADPH
(1)
(3)
(2)Le déficit en G6PD: épidémiologie
Gène sur le chromosome X
Touche les hommes hémizygotes
Femmes conductrices
400 millions de porteurs dans le monde
Se rencontre partout
Peut se révéler tard
Répartition proche de celle
du paludisme:
Protection des infestations
graves des sujets
déficitaires
- Variant Africain A-, sévérité modérée
- Variant Méditerranéen B-, sévère: FAVISME
- 8% de la population SE asiatiqueVoie des pentoses phosphates
Seule voie de production
de NADPH pour l’érythrocyte
(pas de mitochondries)
STRESS OXYDATIF
- Infection
- Médicaments
GSH réduit GSH oxydé
NADPH: pouvoir réducteur qui protège
le GR du stress oxydatifLe déficit en G6PD:physiopathologie
Stress oxydatif aigu
- Fièvre
-Infection
Stress oxydatif -Médicaments
état basal -Aliments (fèves)
GR normaux GR normaux Déficit
Déficit
Pas d’hémolyse
Pas d’hémolyse
Tableau d’hémolyse aigue déclenchée Pouvoir réducteur dépassé
Par une exposition à un stress oxydatif
- Infection bactérienne, virale
- Prise médicamenteuse: Quinine, sulfamides, acide nalidixique, Vitamine C à forte dose...
- Alimentation : Fèves (formes méditérannéennes: FAVISME)
- Sodas à base de quinineTableau clinique
• Différentes types de classes
– - I: AH chronique:sporadiques+++
– Classe II: déficit sévère (1-10% d’activité):Med
– Classe III: déficit modéré (10-60%):A-
– Classe IV: Activité normale (60-100%)
– Classe V: augmentation d’activité (150%).
• Classiquement: poussée d’hémolyse intravasculaires déclenchées par:
– -Médicaments oxydants: Primaquine, sulfamides, sulfones (AFSSAPS)
– Infections (hépatite++, CMV, typhoïde…)
– Favisme+++++
• Fièvre, urines noires, douleurs lombaires, malaise, choc, IRA
• Anémie d’abord arégénérative. Hémoglobinémie, hémoglobinurie, haptoglobine
effondrée, bili svt secondaire, LDH haute, corps de HEINZ
• Le dosage doit être contrôlé à distance+++ (Enzyme DE REFERENCE,
Hexokinase++++++)
• Biologie moléculaireUn exemple de crise hémolytique
Homme de 20 ans
Né en France
Aucun antécédent particulier
( a posteriori INN sans incompatibilité materno-fœtale,
Ayant nécessité une photothérapie pendant qqs jours)
SURVENUE BRUTALE :
•Céphalées
•Vomissements
•Asthénie
Heinz
AGGRAVATION URGENCES
URINES ROUGES
HB : 5g/dL ; Réticulocytes : 60G/L Ascendance sicilienne
Hémoglobinurie , hémoglobinémie lointaine.
Ingestion de fèvesMétabolisme énergétique du globule rouge
Le métabolisme du globule est anaérobie:
-Absence de noyaux
-Absence de mitochondrie
Glycolyse: 90% du glucose est utilisé dans cette voie: Embden-Meyerhof
Production d’ATP
Déficit enzymatique dans la voie de la glycolyse:
-Pyruvate Kinase +++ Glucose
-G6P isomérase
-Hexokinase Glucose 6 P
-Phosphofructokinase ATP NADH
-Triose phosphate isomérase
-Aldolase
-Diphosphoglycérate mutase
- Phosphoglycérate kinase
Pyruvate Fe 2+
Pompe
Na/K-ATP dépendanteDéficit en Pyruvate –Kinase
Transmission autosomale récessive.
Hétérozygotes composites.
Hétérozygotes : 1-2%
Tableau d’hémolyse chronique à prédominance splénique
Diagnostic par dosage enzymatique en dehors d’une poussée
d’hémolyse +/- biologie moléculaireMétabolisme énergétique du globule rouge:
5’ pyrimidine nucléotidase
-Enzyme de dégradation des bases
pyrimisiques
-3 ème cause d’enzympathie dans le
monde
-Inhibée par le plomb!Vous pouvez aussi lire

















































