REPRISE DU SKI APRES CHIRURGIE DU LIGAMENT CROISE ANTERIEUR (LCA) - J.C ROLLIER Clinique d'Argonay Annecy
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous
REPRISE DU SKI APRES
CHIRURGIE DU
LIGAMENT CROISE ANTERIEUR
(LCA)
J.C ROLLIER
Clinique
d’Argonay
Annecy
WWW.ARTHROSPORT-ARGONAY.COM
« RETURN TO SKI » APRES CHIRURGIE DU LCA
un sport
contraignant
pour le genou
des impératifs
biologiques ,
mécaniques
et
anatomiques
CONTRAINTES AU NIVEAU DU GENOU
Une multitude
de
traumatismes
à haute
énergie
RISQUE RE RUPTURE LCA 19%
(compétition)
RUPTURE DU LCA A SKI
MECANISME
hyperextension
rechercher lésions associées
Être capable de contôler ces mouvements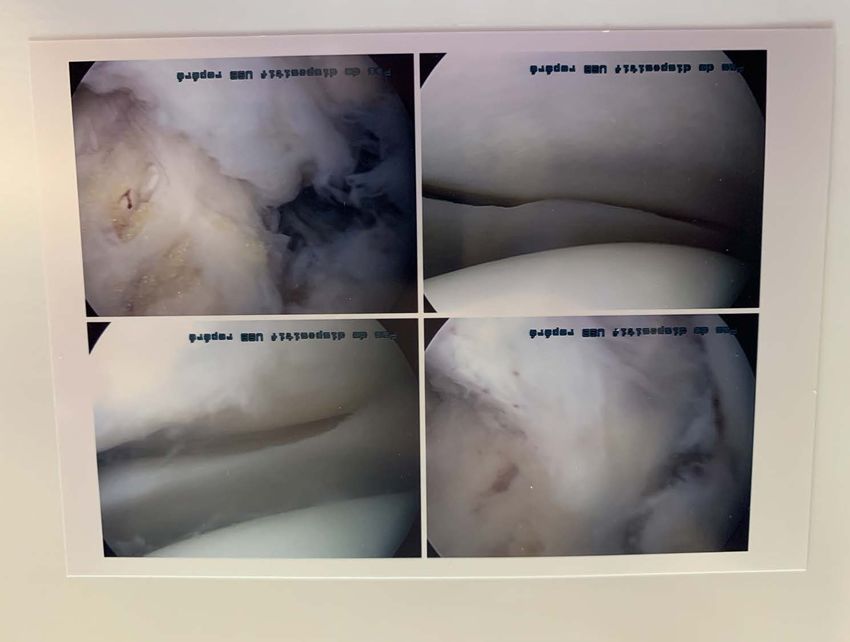
RUPTURE DU LCA A SKI
MECANISME + FREQUENT
CHUTE ARRIERE
avec PERTE D’ APPUI sur 1 SKI
HYPERFLEXION
et ROTATION INTERNE
QUELQUES DONNEES DE LA LITTERATURE
RUPTURES LCA
Facteurs favorisants
SURCHARGE PONDÉRALE
BMI >25
PENTE TIBIALE
> 12°
The Combined Effect of Body Mass Index and Tibial Slope Angles on Anterior Cruciate
Ligament Injury Risk in Male Knees: A Case-Control Study
Volkan Kizilgoz and all .Clin Med Insights Arthritis Musculoskelet Disord 2019,12
REPRISES CHIR
Facteurs favorisants
958 16% douleurs antérieures (KJ < 2
reconstruction ans)matériel (DIDT)
9,7% douleurs sur
s 8,8% raideur
7,2% lésion méniscale
39% complications 5,7% re-rupture (DIDT)
28% de reprises
3% rupture controlateral
(KJ)
Complications After Anterior Cruciate Ligament Reconstruction and Their Relation to the Type
of Graft: A Prospective Study of 958 Cases. Rousseau R and all. Am J Sports Med 2019 Aug 12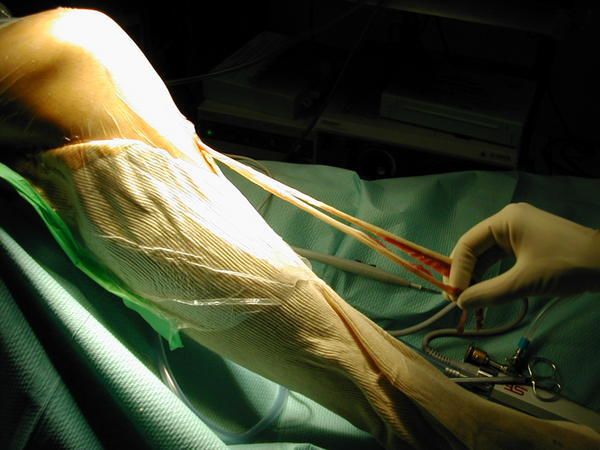
RE RUPTURE
Facteurs favorisants
711 reprises 3,8% ski
14201 (5%) 5% foot
reconstruction Délai moyen
6 ans 6,1 % Hand
s
RISQUE 5X + élevé
< 18 ans que > 35 RISQUE 1,8 X + élevé avec DIDT que
KJ
ans
2,8 X si < 18ans
Similar risk of ACL graft revision for alpine skiers, football and handball players: the graft
revision rate is influenced by age and graft choice. Ekeland A and all. Br J Sports Med 2019 Aug 9
LA FEMME ?
Risque de re-rupture + élevé
Skieuses X 3,1
! avec niveau
mixte X 3,1
collège X 3,9
armée X 9,7
Griffin LY. J Am Acad Orthop Surg 8: 141–150 (2000)
Stevenson H. Iowa Orthop J 18: 64–66
( 1998)CHEZ LA FEMME ?
FACTEURS DE RUPTURE
HYPERLAXITE
récurvatum
distension greffe
Joint hypermobility and ACL injury.
Vaishya R, Hasija R. J Orthop Surg (Hong Kong). 2013 Aug;21(2):
182-4.CHEZ LA FEMME
FACTEURS DE RUPTURE
VALGUS ROTATION EXT
DYNAMIQUE
deseq musc à l appui
(rotat int et ext)CHEZ LA FEMME ?
VALGUS ROTATION EXTERNE
- RUPTURE CHEZ
DANSEUSES
meilleur contrôle ischio
(rotat int)
lors sauts
≠ BASKETTEUSES
+ quadriceps
Ambegaonkar JP. Sports Health. 2011 Jan;3(1):89-96.CHEZ LA FEMME ?
VALGUS ROTATION EXTERNE
DIDT
! forces en abduction
! contraintes latérales
" contrôle neuromusculaire
! risque RE-RUPTURE
Ortiz A. Am J Sports Med. 2013 Feb;41(2):423-9.CYCLOPS
79
ARTICLES Facteurs favorisants
INCIDENCE
PRE OP PER OP POST OP
1,9 à 10,9 % • Inflammation • Echancrure •Sideration
• Perte de étroite musculaire
mobilité • Tunnel tibial
anterieur
Incidence and risk factors for cyclops syndrome after anterior cruciate ligament reconstruction:
A systematic literature review. Noailles T. Orthop Traumatol Surg Res 2019 Aug 9LIGAMENT ANTERO LATERAL
90 LCA ISOLE
reconstruction 2 GROUPES LCA + LAL
s
HYPERLAXITE
MEILLEUR CONTRÔLE TIROIR ANT (ARTHROMETRE)
MEILLEUR CONTRÔLE PIVOT SHIFT
MOINS RE RUPTURE (21,7% VS 3,3%)
PAS DIFFERENCE SCORES FONCTIONNELS
Combined Reconstruction of the Anterolateral Ligament in Patients With ACLInjury and Ligamentous
Hyperlaxity Leads to Better Clinical Stability and a Lower Failure Rate Than
Isolated ACL Reconstruction. Helito CP and all. Arthroscopy 2019 Aug 14LIGAMENT ANTERO LATERAL
62 Pas diff pre op
reconstruction 26 lésions LAL
(IRM) pivot shift
s
LCA Résultats
ISOLE identiques
No difference in postoperative rotational laxity after ACL reconstruction in patients with
and without anterolateral capsule injury: quantitative evaluation of the pivot-shift test
at 1-year follow-up.
Hiroshima Y and all. Knee Surg Sports Traumatol Arthrosc 2019 Aug 14Prévenir
complication
s
PRE OPERATOIRE
Retour au
RETUR
niveau
antérieur
N TO Délais
corrects PER OPERATOIRE
SKI
POST OPERATOIRE
Bonnes
sensation
sPRE - OPERATOIRE
PRE - OPERATOIRE
PREVENIR LES COMPLICATIONS
Prise en charge rapide avec bilan initial
exhaustif
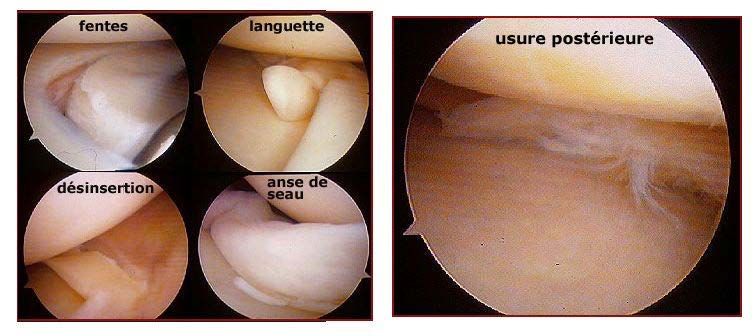
Ne pas méconnaitre une urgence chirurgicale
anse de seau méniscale
atteinte associée LLE, pfs LLI
Detecter patients à risque complication ou re-rupturePRE - OPERATOIRE
QUAND DEMANDER UNE IRM ?
Toujours faire une radio pour éliminer une
fracture
EN URGENCE si suspicion anse de seau
ou
lésion associée
SINON pas avant 3 semaines
car faux positifs et faux négatifs avant
NE PAS RETARDER LA REEDUCATIONPRE - OPERATOIRE
LCA + anse de
seau
EN 1 TEMPS dans les 10 jours
EN 2 TEMPS au delà
Risque raideur
amyotrophie
cyclopPRE - OPERATOIRE
DEFINIR UN OBJECTIF REALISABLE REEDUCATION
Volonté SPORTIVE / vie FAMILIALE et PRE OP
PRO
Selon LESIONS ASSOCIEES
suture Méniscale + 1 mois
rupture LLE ou LLI + 2 mois
Selon « ETAT » DU GENOU
pour opérer : quadriceps réveillé avec extension
active
schéma de marche acquis
mob 0-110PER - OPERATOIRE
PER - OPERATOIRE
Information
Rééducatio
n
BIEN ambulatoire
immédiate
ÊTRE
Infiltrations
cryothérapi
ePER - OPERATOIRE
QUELLE GREFFE
?
DIDT vs KJ
Dans la LITTERATURE
pas de différence à moyen et à long
terme
sur le plan fonctionnel et risqueQUELLE GREFFE PER - OPERATOIRE
?
DIDT vs KJ
+ RE RUPTURES
Avant 18 ans
Femmes + AMYOTROPHIE QUADRICIPITALE
Hyperlaxité + DOULEURS ANTERIEURSPER - OPERATOIRE
QUELLE GREFFE
?
DIDT > KJ
mais GARDER
INDICATIONS KJ
pour cas particulierPER - OPERATOIRE
QUELLE GREFFE
?
DT4
bons résultats fonctionnels
MAIS
Pas logique sur le plan
biologique
Technique plus aléatoire
(tension, longueur tunnel)
Pas > DIDTPER - OPERATOIRE
PRESERVER AU MIEUX
LES FIBRES DU LCA NATIF
FACILITATION NEURO MUSCULAIRE
MEILLEURE PROPRIOCEPTION
GAINE BIOLOGIQUE
Permanent knee sensorimotor system changes following ACL injury and surgery.
Nyland J and all. Knee Surg Sports Traumatol Arthrosc 2017 May;25(5) : 1461-1474PRESERVER LE PER - OPERATOIRE LCA NATIF
PRESERVER LE PER - OPERATOIRE LCA NATIF
LIGAMENT PER - OPERATOIRE
ANTERO
LATERAL
QUAND LE RECONSTRUIRE ?
Laxité antérieure
chronique SUJETS à RISQUE
Ressaut rotatoire +LIGAMENT PER - OPERATOIRE
ANTERO
LATERAL
PRISE EN CHARGE IDENTIQUE
Recupération plus lente de la flexion
Respecter la raideur externe jusqu’ à 3
mois
Traiter les douleurs externes spécifiques
TENODESE EXTERNE au FASCIA
LATAPOST - OPERATOIRE
REEDUC
POST - OPERATOIRE
PHASE INITIALE IMMEDIATE
0-45 jours
OBJECTIF
ne pas exclure la jambe
opérée
ne pas perdre les
FAVORISER LE FONCTIONNEL
automatismes
travail du déroulement du pas
travail de l appui sur la jambe
opérée
MARCHER NORMALEMENT APRES 15 à 21 JOURSPHASE INITIALE POST - OPERATOIRE
0-45 jours
REVEIL MUSCULAIRE
RECUPERATION DES AMPLITUDES
RODAGE
NE PAS MUSCLER UNE ARTICULATION RAIDE
NE PAS RENFORCER UN MUSCLE NON REVEILLEREEDUC
POST - OPERATOIRE
2è PHASE ADAPTEE
45-90J
OBJECTIF
Favoriser les activités
quotidiennes
Rodage articulaire
Proprioception bipodale
RATTRAPER RETARD EVENTUEL
PROTEGER LES GENS A RISQUE +++3è PHASE REEDUC
POST - OPERATOIRE ADAPTEE
RE
ATHLETISATION
OBJECTIF
reconstruire l’enveloppe
musculaire
reprise des appuis, travail
extérieur
proprioception unipodale
REPRISE DE LA COURSE, MARCHE en MONTAGNE,
VELO EXTERIEUR5-12 MOIS
MUSCLE
MENTAL
ARTICULATION
OK
GREFFE FONCTIO
N
OK
GO TO SKIRETURN TO PLAY
86 % Rejouent en NBA
58 Basketteurs La saison suivante (98%)
LCA 11,6 +- 4,1 mois
3,1% re- NIVEAU INFERIEUR
rupture mais identique groupe
contrôle
Return to sport and performance after ACL reconstruction in NBA players
Joshua D harris and all July 2013.40 Patients
RETURN TO PLAY
LCA
Tampa Scale of Kinesiophobia (TSK-11)
(≥17)
4X + niveau inférieur
7X + hop test < 95%
6X + deficit quadriceps >
10%
13X + de nouvelle lésion dans les 2 ans si TSK 11 ≥ 19
Self reported fear predicts functional performance and second ACL injury after ACL
reconstruction and return to sport :a pilot study Mark V Paterno and all. Dec 2017.5-12 MOIS RETURN TO SKI TEST
ISOCINETIQUE
CRITERES MUSCLAIRES
EVALUATION OBJECTIVE
Quadriceps+IJ concentrique (lent et rapide
Quadriceps+ IJ excentrique
Ratio Quad/ IJ concentrique (lent et rapide
Ratio mixte IJ (exc) /Quad (conc) (rapide)
IMPORTANCE DE LA COURBE
(qui doit être harmonieuse)
RÔLE FONCTIONNEL et PREVENTIF5-12 MOIS RETURN TO SKI TEST
ISOCINETIQUE
CRITERES MUSCLAIRES
OBJECTIF
Quadriceps + IJ concentrique (lent et rapide) <
10-15%
Quadriceps + IJ excentrique < 10-15%
Ratio Quad/ IJ concentrique (lent et rapide) 0,5 à 0,7
Ratio mixte IJ (exc) / Quad (conc) (rapide) 0,9 à 1,1
REPERER ANOMALIES SPECIFIQUES SUR LA COURBE
REPETER APRES 1 à 3 MOIS
Selon MOTIVATION et OBJECTIFS SPORTIFSDifférents RETURN TO SKI
scores
CRITERES PSYCHOLOGIQUES
RECHERCHE DE PATIENTS A RISQUE
EVALUER LA PROGRESSION
PSYCHO / FONCTION
AIDE DE L’HYPNOSE
TRAVAIL DE GROUPE
Evaluation post trauma et
pré-opGENOUILLERE RETURN TO PLAY
A
REPRISE
28 Patients Hop test attelle
opérés Force atterrissage
Facilite symétrie Hop
test
Augmente force impact
ds 3er mois
Hop testing symmetry improves with time and while wearing a
functional kneebrace in anterior cruciate ligament reconstructed athletes.
Peebles AT and allDifférents
RETURN TO SKI
scores
CRITERES FONCTIONNELS
COFRAS
SAUTS (impulsion, réception)
COURSE
K-START
STABILISATION
ESCALIERS
ACCROUPISSEMENT
REPETER et CORRELER avec PSY
&MUSCLERETURN TO SKI ✔ ✔ ✔✔
RETURN to SKI KINE SANTE FORMATION
CHAMONIX
(S. BALMAT)
SUR LE TERRAIN
OBJECTIF
Redonner confiance et des outils pédagogiques
GROUPES DE NIVEAU DETECTER PERSONNES A
RISQUE
MONITEURS / KINES /
PREVENIR APPREHENSION
CHIR
DONNER DES BASES
TECHNIQUES DE REPRISERETURN to SKI
RETURN TO SKI
Planification
n
depuis
e m e n t
i c a t i o l’accident
p a g n
Com m u n Accom
Technique Evaluation IDENTIFIER PERSONNES
chirurgicale objective
et A RISQUE
rééducation Avant Prise en charge spécifique
adaptée repriseVous pouvez aussi lire