Cancer de verge avancé ou métastatique - Mise au point THIERY-VUILLEMIN Antoine (MCUPH Oncologie Médicale CHRU Besançon)
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous
Cancer de verge
avancé ou métastatique
Mise au point
THIERY-VUILLEMIN Antoine (MCUPH Oncologie Médicale CHRU Besançon)
a.thieryvuillemin@mac.com
Objectifs • Epidémiologie • Guidelines • Thérapies systémiques • Etude PULSE
Epidémiologie
Pour année 2013
Répartition des personnes
ayant une hospitalisation en
lien avec le cancer
Répartition par localisations
tumorales des personnes
atteintes de cancer traitées
par chirurgie
Répartition par localisations
tumorales des personnes
traitées par chimiothérapie
~ 1-2% de l’activité prostate
Extraction régionale BPC =
4 patients traités par DCF depuis 2012, pas de PIC
INCA 2014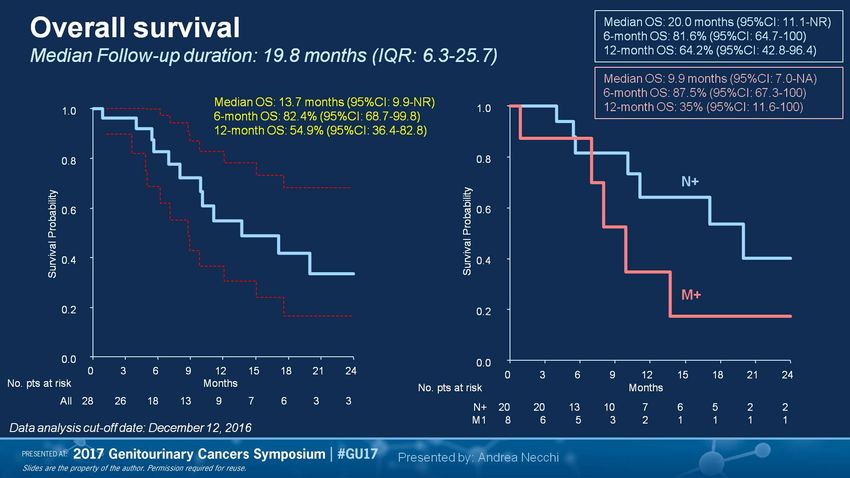
Epidémiologie Onco-Uro
n de l’incidence
Projection de
et de
l’incidence
la mortalité
et de la mortalité
r urologique
par cancer
en France
urologique
en 2010
en France en 2010
X. Rébillard*, P. Grosclaude,
X. Rébillard*,
T. Lebret,
P. Grosclaude,
J.-J. Patard,
T. Lebret, J.-J. Patard,
C. Pfister, P. Richaud,C.J.Pfister,
Rigaud,P.L.Richaud,
Salomon,J.M.Rigaud, + fréquent
SouliéL. Salomon, M. Soulié
et les membres du CCAFU
et les membres du CCAFU
Verge
les de l’incidence
Les estimations
Testis
et de la mortalité
nationales decer
l’incidence
jusqu’enet2005
Rein
de la(Francim)
mortalitéet des
Vessie
cerdonnées
jusqu’ende2005
mortalité
Prostate
(Francim) et des données de mortalité
n 2010, présentées
par cancer ci-dessous,
urologiquesont
en 2010, présentées
observées surci-dessous,
la France sont
entière observées
jusqu’en 2007
sur la(Inserm-
France entière jusqu’en 2007 (Inserm-
on des données
issues d’incidence
d’une modélisation
obser- des données
CepiDC) [1]d’incidence
(Tableau 1).obser- CepiDC) [1] (Tableau 1).
38deans
Can- TS
couverts par un Registre67 ans H 72 ans H 74 ans H
75 ans
nts couvertsvées H Registre
par sur
un les départements de Can-
30 ans TNS 70 ans F 77 ans F dépistage
e cas et de décès des1.cancers
Tableau Nombreurologiques
de cas et de
et des
décès
principaux
des cancers
autres
urologiques
cancers pour
et des
l’année
principaux
2010 autres
en cancers pour l’année 2010 en
ondants standardisés
France et monde
taux correspondants
(pour 100 000 standardisés
personnes-années).
monde (pour 100 000 personnes-années).
dence Incidence Mortalité Mortalité
mbre de cas Taux standardisés
Nombre monde
de cas Nombre
Taux
de standardisés
décès Taux
mondestandardisés
Nombre monde
de décès Taux standardisés monde
Rein
7 Hommes
13,7 7037 2492 13,7 4,0 2492 4,0
5 Femmes
5,6 3505 1296 5,6 1,4 1296 1,4
Vessie Population âgée
2 Hommes14,9 8942 3514 14,9 5,2 3514 5,2
8 Femmes2 1798 1157 2 1 1157 1
77 Prostate128,8 71 577 8791 128,8 11,2 8791 11,2
0 7,0
Testicules 2220 87 7,0 0,2 87 0,2
Tous cancers
000 Hommes381,8 203 000 84 500381,8 141,8 84 500 141,8
500 Femmes264,2 154 500 62 000264,2 77,5 62 000 77,5
00 Sein 100 52 500 11 500100 16,2 11 500 16,2
Nombre
Côlon de cas et de décès des cancers urologiques et des principaux
00 autres cancers
Hommes
36,5 21pour
000 l’année
92002010
36,5 en France
14,1 9200 14,1
Rébillard et al AFU 2010, RDP 2007
00 Femmes
24,5 19 000 8200 24,5 8,3 8200 8,3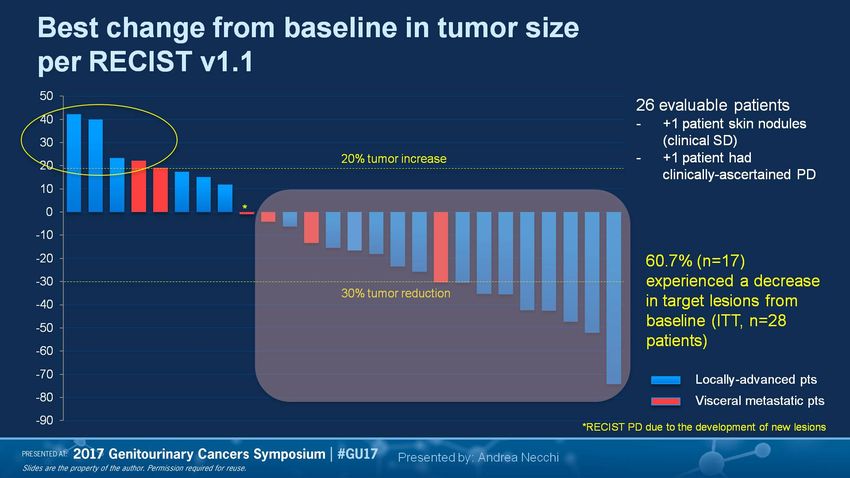
Profil
• Âge
• Comorbidités
• Co-médications
• Fonction rénale (Platine)
• Infection
• Loco-régionale
• HPV / VIH
• Pronostic sombre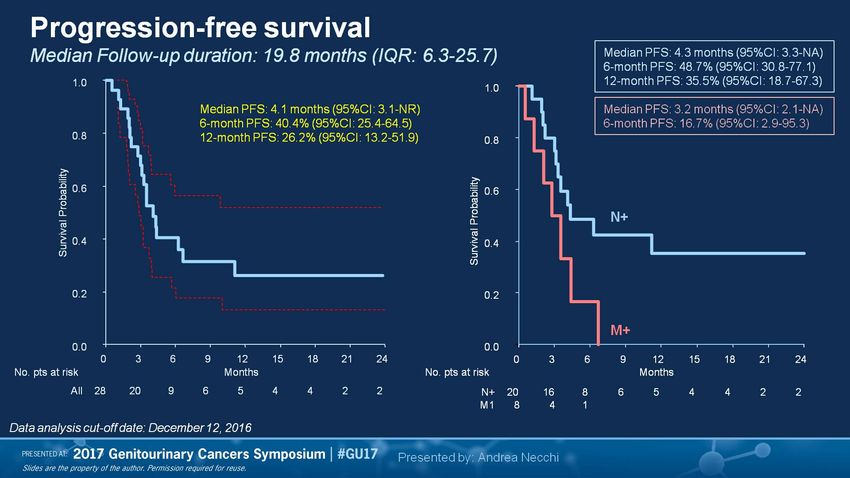
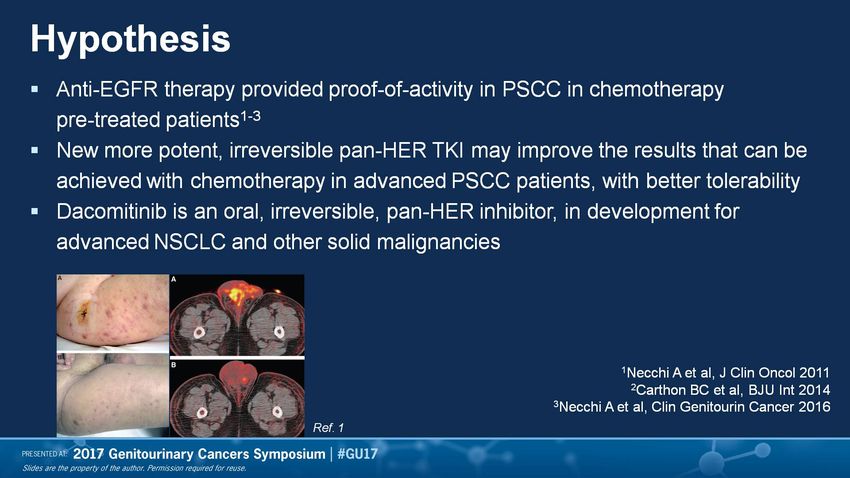
Histologie // Pronostic
• Vast majority = squamous cell cancers
• Other histologic types are observed in ∼5% of cases :
melanomas, basal cell carcinomas and sarcomas
• Extension
• Clinique / Rx / TDM / PET / cytoponction ?
EAU 2017 AFU 2016 Sonpavde Annals Oncol 2013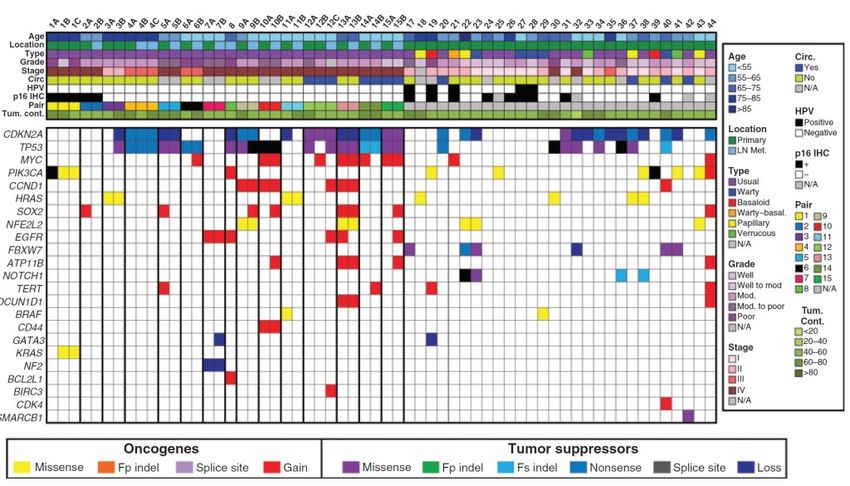
Pronostic neoadjuvant or adjuvant chemotherapy from 1990 onward at 12 centers n= 201 Necchi Clin Can Geni Can 2017
Objectifs • Epidémiologie • Guidelines • Thérapies systémiques • Etude PULSE
TNM // Extension EAU 2017
Localement Avancé EAU 2017
Arbre AFU 2016 AFU 2016
Objectifs • Epidémiologie • Guidelines • Thérapies systémiques • Etude PULSE
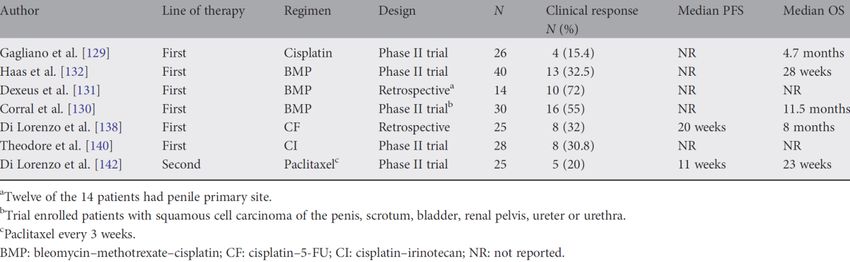
Chimiothérapies Sonpavde Annals Oncol 2013
Chimiothérapies
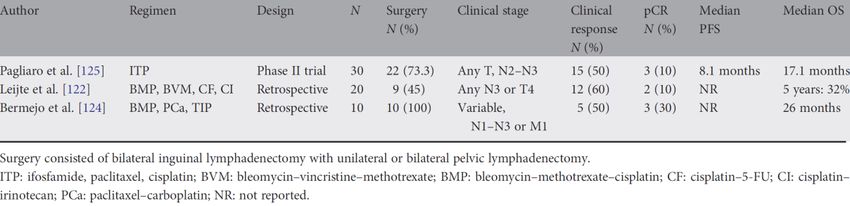
PIC néoadjuvant
-Eligible patients had stage N2 or N3
(stage III or stage IV) penile cancer without
distant metastases.
-Four courses every 3-4 weeks
ORR 50% (95% CI, 31% to 69%)
Pagliaro JCO 2010 30.0% SD, and 20% PDChimiothérapies DCF 29 pts with locally advanced or M+ squamous carcinoma of the penis • Median PFS and OS for all enrolled patients, was 7.1 mo and 13.9 mo • Median PFS and OS for the PP population (n=26, sensitivity analysis) are 6.9 and 7.7 mo Nicholson BJC 2013
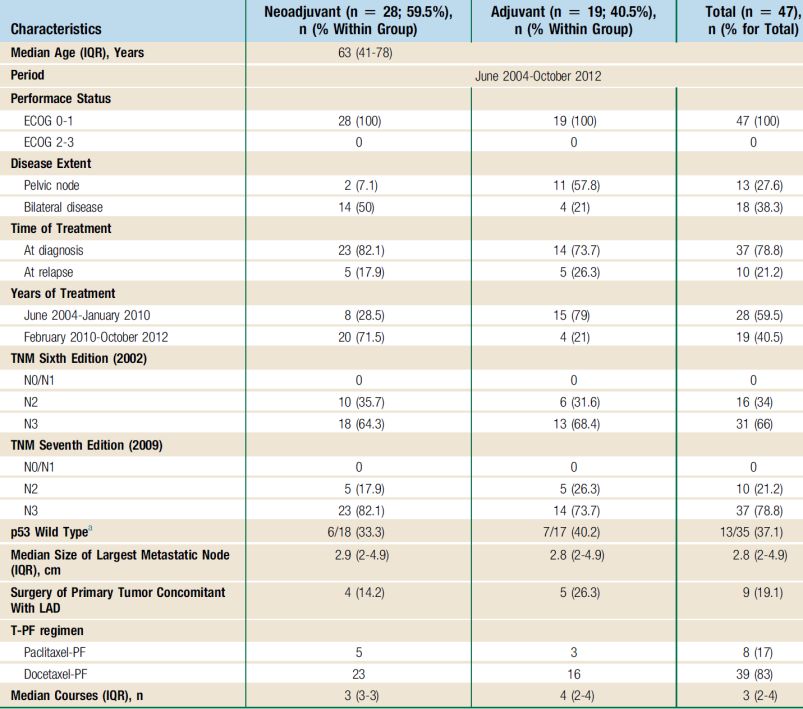
Chimiothérapies DCF neo/adjuvant 47 consecutive N2 to 3 M0 pts neoadjuvant (n = 28) or adjuvant (n = 19) Nicolai Clin Gen Can 2015
Chimiothérapies
DCF neo/adjuvant
OS PFS
Among the 28 patients who received neoadjuvant, 42.9%[ 95% CI,
26.6-60.9] achieved a major response (CR+PR) and 14.3% had pCR
at definitive pathology
Nicolai Clin Gen Can 2015Slide 4
Presented By Andrea Necchi at 2017 Genitourinary Cancers SymposiumSlide 10
Presented By Andrea Necchi at 2017 Genitourinary Cancers SymposiumSlide 11
Presented By Andrea Necchi at 2017 Genitourinary Cancers SymposiumSlide 12
Presented By Andrea Necchi at 2017 Genitourinary Cancers SymposiumSlide 13
Presented By Andrea Necchi at 2017 Genitourinary Cancers SymposiumSlide 16
Presented By Andrea Necchi at 2017 Genitourinary Cancers SymposiumBiologie moléculaire
Frequency of genomic alterations in
advanced penile cancer
Ali The Oncologist 2016
Integrative molecular
profiling of somatic genomic
alterations in PeSCCA
Mc Daniel Clin Can Res
2015Objectifs • Epidémiologie • Guidelines • Thérapies systémiques • Etude PULSE
Autres Etudes
Nombre de
Titre Primary
patients
A Phase 2, Multi-centre, Open-label Study of Avelumab
(MSB0010718C) in Locally Advanced or Metastatic Penile
24 ORR NCT03391479
Cancer Patients Unfit for Platinum-based Chemotherapy or
Progressed On or After Platinum-based Chemotherapy
Nivolumab Combined With Ipilimumab for Patients With
57 ORR NCT03333616
Advanced Rare Genitourinary Tumors
DART: Dual Anti-CTLA-4 and Anti-PD-1 Blockade in
707 ORR NCT02834013
Rare Tumors
Non-
Phase II Study for the Evaluation of Efficacy of Pembrolizumab Progression
250 NCT02721732
(MK-3475) in Patients With Rare Tumors Rate (NPR) at
27 weeksACSE
Trial design
Eligibility
--Non-clear cell renal-cell carcinomas:
papillary renal cell carcinoma,
chromophobe, renal medullary carcinoma,
Metastatic disease or
collecting duct/Bellini duct carcinoma,
unresectable locally
microphthalmia-associated transcription
advanced malignancy that
family translocation renal cell carcinoma,
is resistant or refractory Nivolumab 240 mg IV
renal cell carcinoma with a prominent
to standard therapy or for over 60 minutes
sarcomatoid component.
which standard therapy every 14 days.
--Rare head and neck cancers
does not exist or is not
--Rare skin cancers
considered appropriate
--Non-colorectal cancers with microsatellite
by the Investigator
instability determined locally by
immunohistochemistry or polymerase
chain-reaction (PCR)
--Squamous cell carcinoma of penis.
Between 20 and 50 patients will be
enrolled in each cohort
Primary Objective
ORR will be assessed per cohort by an IRC according to RECIST v1.1
NCT03012581PULSE : Rationnel
• Frequent PD-L1 expression in PSCC
• PD-L1 expression can be seen in 62.2% of primary tumors with a
strong positive correlation of PD-L1 expression in primary and
metastatic samples [Udager 2016].
• Immunotherapies targeting PD1/PDL1 axis are effective in
other SCC +/- HPV linked cancers
• Lung SCC : FDA approved pembrolizumab in 2015
• Head and neck SCC : Treatment with the immunotherapeutic
nivolumab improves survival; HPV positive patients seemed to derive
higher benefit from nivolumab than HPV negative patients [Gillison
2016].
• Morris et al has found that the immune checkpoint inhibitor nivolumab
shows promise for the majority of patients with squamous cell
carcinoma of the anal canal (SCCA). Also of note, this is the first
completed anti–PD-1 study to include HIV-positive patients as well as
patients with Hepatitis B or C. Two HIV-positive patients were enrolled
in the trial [Morris 2016].PULSE : Trial design
Vous pouvez aussi lire