Malpositions vasculaires Ventricule droit à double issu (VDDI) - Le point de vue du cardiopédiatre Dr Daniela Laux, UE3C M3C-Centre des ...
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous

Malpositions vasculaires
Ventricule droit à double issu (VDDI)
Le point de vue du cardiopédiatre
Dr Daniela Laux, UE3C
M3C-Centre des Malformations Congénitales Cardiaques complexes
VD
AP
AO
OD
Dr Daniela Laux, UE3C-Paris et M3C-CCML
Cardiopathies congénitales humaines Fréquence Incidence Communication interventriculaire (CIV) 30% 1500 Communication interauriculaire (CIA) 8% 400 Sténose pulmonaire (SP) 7% 350 Persistance du canal artériel (PCA) 7% 350 Coarctation de l’aorte (CoA) 6% 300 Tétralogie de Fallot (T4F) 6% 300 Transposition des gros vaisseaux (TGV) 5% 250 Sténose aortique (SA) 5% 250 Canal atrioventriculaire (CAV) 4% 200 Atrésie pulmonaire à septum intact (APSI) 2% 100 Atrésie pulmonaire à septum ouvert (APSO) 2% 100 Atrésie tricuspide (AT) 2% 100 Tronc artériel commun (TAC) 2% 100 Retour veineux pulmonaire anormal (RVPA) 2% 100 Malpositions vasculaires (MV) 1% 50 Interruption de l’arc aortique (IAA) 1% 50 Ventricule unique (VU) 1% 50 Anomalie d’Ebstein 1% 50 Discordances AV et VA 1% 50 Autres 6% 300

VDDI : Définition anatomique difficile
• Règle des 50%...
• « Septum conal au-dessus
du VD »...
• Discontinuité mitro-Ao ou
mitro-AP…..
Mahle et al. City 2008
Une seule définition :
VDDI = 2 gros vaisseaux au-dessus du VD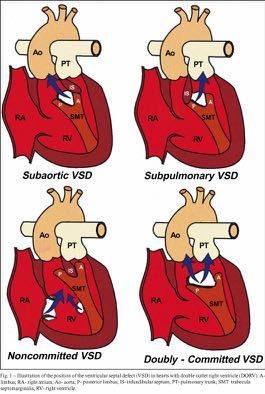
Rappel rapide Embryologie et anatomie

Cœur normal
Ao
AP
Rotation
CT « normale »
O
VD Ao AP
VG
Rotation
« inversée »
TGV
Early looping Convergence Rotation
Courtesy L.Houyel
Interaction crête neurale / Aire cardiaque antérieure
Défaut de migration des cellules de la crête neurale Second champ
cardiaque
Crête
neurale
Défaut d’adjonction de myocarde
par l ’aire cardiaque antérieure CT
O
Défaut d’élongation de la voie d’éjection
VD
Défaut de convergence et de wedging
VG
CARDIOPATHIES CONOTRUNCALES
Courtesy L.Houyel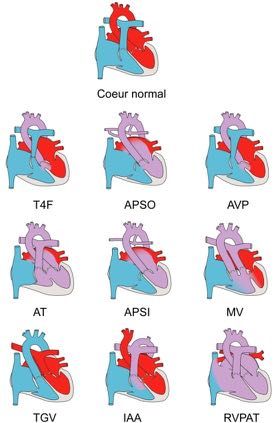
Deux groupes principaux
Implications anatomiques
• Groupe 1 (VDDI tardifs) = outflow tract defects
la CIV sera toujours de l’outlet
(sous-aortique, sous-pulm, doubly committed)
• Groupe 2 (VDDI précoces)/ =
la CIV sera autre (membraneuse, inlet,
musculaire) et le septum conal sera intact
Van Praagh et al. Cœur 1982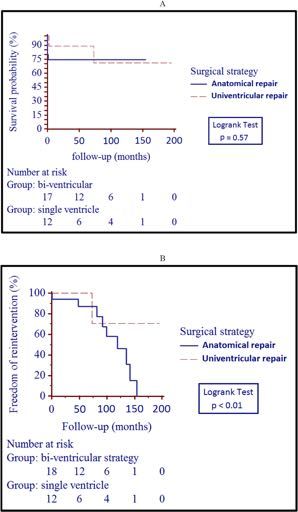
AP Anomalie de formation du septum conal
CIV de la voie d’éjection (outlet)
GROUPE 1
• Y de la bande septale = Zone de fusion
entre le septum conal et le septum
interventriculaire primitif
• Pas de fusion à ce niveau: hypoplasie ou
malalignement du septum conal
AP
SC
• CIV de la voie d’éjection
• (cardiopathies conotruncales)
Courtesy L.Houyell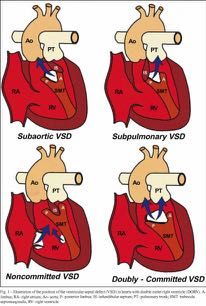
GROUPE 2 CIV pm, l’inlet ou musculaire
Septum membraneux
entre cusp CD et
cusp non coronaire
* Mitrale
Septum Surface
admission septale
lisse
Piliers
Septum
musculaire
Vue du ventricule gauche Courtesy L.Houyel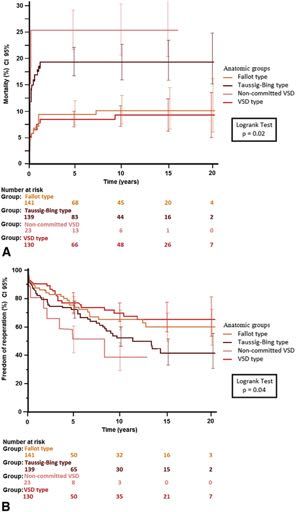
Présentation clinique VDDI et associations génétiques
Anomalies chromosomiques et cardiopathies
fœtales : 548 cardiopathies-18.5%
• Canaux atrioventriculaires 32/68 47%
– 28 T21; 3 T18; 1 XXX
• Anomalies conotroncales 23/91 25%
– 20 del22q11; 1 T21; 2 anomalies de structure
• VDDI 7/38 18%
• Communications interventriculaire 12/74 16%
– 9 trisomies, 2 del22q11, 1 del5
• Obstacles gauche à SIV intact 12/130 9.2%
– 6 XO; 3 T18; 3 anomalies de structure
• VU et atrésie tricuspide 2/24 8%
– 2 T18
• Transposition des gros vaisseaux 0 0%
• Obstacles droits à SIV intact 0 0%
Série de NeckerSyndrome de Di George
- cardiopathies conotroncales
- anomalie des arcs, aorte à droite
- microdélétion du chromosome 22q1.1
- Gène Tbx1
IAA TAC T4F APSO AVP CIV MVAssociation CHARGE
• Colobome
• Heart defect
• Atrésie des choanes
• Retard de développement
• Génitales anomalies
• Ear anomalies
– Agénésie des canaux semi-circulaires
– Hypoplasie des lobes olfactifs
Gène CHD7 : 70 %Trisomie 18 Trisomie 13 Dysplasie polyvalvulaire CIV PCA CIV, CIA, PCA, CAV T4F Malposition vasculaire Cardiopathie obstructive gauche CAV Malposition vasculaire Dysplasie polyvalvulaire Ventricule unique
Présentation clinique
Diagnostic
Pathophysiologie
Anomalies associésVDDI, une malformation hétérogène…
Fallot-type
PA stenosis
VSD-type
Complex forms
TGA-type Non-committed
(Taussig-Bing) VSD
Lev M et al J Thorac Cardiovasc Surg 1972Types de VDDI en fonction de la physiologie:
– VDDI type CIV + discontinuité mitro-aortique
• Rose, symptômes d’hyperdébit
– VDDI type Fallot (CIV sousaortique)
• Cyanose progressive, malaise possible
– VDDI type TGV + CIV (CIV souspulmonaire)
• Cyanose, nécessité d’un Rashkind?
– VDDI type TGV + CIV + sténose pulmonaire
• Cyanose, Rashkind pour pouvoir attendre de réparerDiagnostic prénatal • Pas de chiffres sur le taux de détection en France • Malposition vasculaire = anomalie des 3 vaisseaux/ voies d’éjection • DAN VDDI= – Recherche anomalies extracardiaques – Discussion d’amniocentèse – Discussion d’IRM fœtale (Charge) – Poursuite de la grossesse ou IMG ? – Organisation de la naissance: Où et comment?
IUFD occurred in two (4.4%) fetuses with the AVSD-
type DORV, left isomerism and complete heart block.
Twenty-six
Ingoneonates (57.8%) a,were
Gottschalk born alive.
*, Judith NNDa, Tina Menzel, Ulrike Herberg, Johannes Breuer,
S. Abel
occurred in three (6.7%) cases, including one neonate
Ulrich Gembruch, Annegret Geipel, Konrad Brockmeier, Christoph Berg and Brigitte Strizek
with trisomy 18 and another one with a suspected genetic
V were diag-
at first diag- Prenatal diagnosis, associated findings and
syndrome. Both neonates died after compassionate care.
The third neonate died due to low cardiac output failure
postnatal outcome of fetuses with double outlet
after cardiac surgery at the age of 15 days.
A with VSD. CHD occurred in four (8.9%) cases, including two
right ventricle (DORV) in a single center
alysis. Only cases with trisomy 17 mosaicism and Cornelia de Lange
all 46 cases syndrome, respectively. Both received compassionate
Gottschalk et al.:
J. Perinat. Med. 2019;Double outlet right ventricle in the fetu
47(3): 354–364
atal diagno-
llot type, 27
Table 1: Outcome of 45 cases with DORV according to the
https://doi.org/10.1515/jpm-2018-0316 anomalies, 30 (66.7%) had DORV
extracardiac anomalies and 13 a,*, Judith S. Abela, Tina Menzel, U
Ingo Gottschalk
associated condition.
Received September 18, 2018; accepted November 26, 2018; (28.9%) had chromosomal 46
or syndromal anomalies. Ulrich Gembruch, Due Annegret Geipel, Konrad Brockm
he non-com-
previously published online December 20, 2018 to their complex additional anomalies, five (11.1%) Prenatal of our diagnosis, associa
SD type with
Trisomy 18
Abstract
n TOP IUFD NND CHD Alive
6 5 1
Top
17
45 fetuses IUFD
2
had Exclusion
multiple malformations
1
NND and were highly
CHD
3 Gottschalk et al.:4Double
2010-2017
postnatal Alive
outlet right19
outcome 361
of fetus
suspicious for non-chromosomal genetic syndromes, ventricle in the fetus
Trisomy 13
Objective: To assess
Trisomy 17 mosaicism
1
1
1
the spectrum 1of associated anoma- although molecular diagnosis could not be provided. right Surgery ventricle
Dis- 1
pending (DORV) in a
genetic Triploidy 69XXXlies, the intrauterine
1 1 course, postnatal outcome and 1.0
orders of laterality occurred in 10 (22.2%) fetuses. There
https://doi.org/10.1515/jpm-2018-0316 an
22q11 microdeletion 1 1
management of fetuses with double outlet right ventricle were 17 terminations of pregnancy (37.8%), Received
0.8
two (4.4%) September 18, 2018; accepted November 26, 2018; (2
Cumulative survival
Biventricular
Cornelia de Lange syndrome 1 1 previously publishedrepair
online December 20, 2018 to
(DORV). intrauterine and seven (15.6%) postnatal deaths. Nineteen 7
0.6
Kleefstra syndrome 1 1 Abstract 45
r additional
Methods:
syndromeAll cases1 of DORV diagnosed prenatally over a of 22 (86.4%) live-born children with an intention to treat
0.4
Johanson-Blizzard 1 Single ventricle
su
c anomalies Multiple malformation syndrome 7 5 1 1 Objective: To assess the spectrum of associated anoma- al
period of 8 years were retrospectively collected in a single were alive at last follow-up. The mean follow-up among 11 course, postnatal outcome and or
0.2 palliation
4.4%) cases. lies, the intrauterine
Heterotaxy 10 2 2 6
tertiary referral15center. All additional prenatal findings 0 survivors 30 was 32
50 months (range, 2–72). Of 21 children who
0.0
management of fetuses with double outlet right ventricle w
hout mitral Isolated 2 1 2 10 10 20 40 60 70 80 90
(DORV). in
or extracar- Total were assessed and 45 correlated
17 2 with 3 the4 outcome.
19 The accu- had already undergone postnatal surgery, eight
Figure 1: Outcome of 46 cases with
Time, months
prenatally diagnosed double outlet right (38.1%)
ventricle (DORV).
Methods: All cases of DORV diagnosed prenatally over a of
racy of prenatal diagnosis was assessed. TOP,Figure
termination of pregnancy;
achieved
2: Kaplan-Meier IUFD,survival
biventricular
curve for observed intrauterine
of 46 casesfetal
repair with death; NND, neonatal death; CHD, death in infancy or childhood.
and 13 (61.9%) periodreceived
of 8 years were retrospectively collected in a single w
ses, includ- TOP, termination of pregnancy; IUFD, intrauterine fetal death; NND, prenatally diagnosed double outlet right ventricle.
tertiary referral center. All additional prenatal findings su
neonatal death;Results:
CHD, deathForty-six
in infancy orcases of DORV were diagnosed The pre- univentricular palliation. One recently born child is still
dotted line represents term.
fts, cerebral childhood. were assessed and correlated with the outcome. The accu- ha
natally. The mean gestational age at first diagnosis care.was
The third waiting infant fordiedsurgery.
because Allofchildren predicted prenatally
global respiratory
racy of prenatalto
palliation,
diagnosis was assessed.
and all children predicted to achieve
ac
Results: Forty-six cases of DORV were diagnosed pre- un
21 + 4 weeks (range, 13–37). A correct prenatal insufficiencydiagno- need afteracardiac
single surgery
ventricle at thepalliation,
age of 3 monthsand all children lar repair,
natally.
pre-
The ultimately
mean gestational received thediagnosis
age at first predicted wastypw
sis of DORV was made in 96.3% of the cases. If the rela- dicted to achieve
and the fourth infant died because of renal and biventricular repair,
Figure 4: ultimately
cardiacDORV, TGA type,
21 + 4 received
with subpulmonary
weeks (range, VSD and overriding
Within the biventricular repair grou
13–37). A correct prenatal diagno- ne
Précision globale du diagnostic prénatal de « VDDI » dans cette série:
tion of the great arteries, the position of the ventricular failure afterthe thepredicted
second step typeof of surgery.
Norwood palliation
pulmonary trunk.
AfterLV,surgery,
leftat the 14
ventricle;
sis of DORV was made in 96.3% of the cases. If the rela- di
of
right 18
RV, received (77.8%)
ventricle;
tion of the great
Ao, aorta; *subpulmonary VSD.
either
TP, overridingone-stage
arteries,
pulmonary trunk;
the positioncomplete repair or
of the ventricular th
septal defect (VSD) and additional cardiac anomalies age ofare children
11 months (Table were1). healthy without any impairment. monary
septal defect(AP) shunting, right-ventricle-to-p
96,3% ( 1 erreur)
taken into account, the prenatal diagnosis was correct in Conclusion:
Nineteen of the 45 children DORVwith is aarare confirmed
and oftendiagno- complex artery
92.6%
cardiac
(VSD) and
of the with
cases.aOne
additional cardiac
(RV-PA) conduit, VSD patch or VSD
case wascon-
anomalies are ch
taken into account, the prenatal diagnosis was correct in Co
postnatally classified an
Among the 26 liveborns postnatally
Détails du diagnostic VDDI pris en considération:
92.6% of the cases. One case was postnatally classified sis of DORVanomaly
script, resulting
were alivethat at the
cantime of writing ofprenatally
be diagnosed the manu-
firmed with
diagnosis aortic
high
asDORV,
of arch
preci-
transposition
iesadditional
there reconstruction,
of the
were the great arteries
following
or arterial switch operation, depending on
typesbanding of pulmo
with subpulmonary si
as transposition of the great arteries with subpulmonary sion.inDORV an overall survival rate
is frequently of 42.2%.
associated of After
DORV:
with one
major VSD
(3.8%) and
VSD was
type,excluded
two from
(7.7%) further
Fallot analysis.
type, A total of 41 an
position des gros vx, CIV, anomalies associées: 92,7% (2 erreurs)
VSD and was excluded from further analysis. A total exclusion
of 41 ofanomalies,
TOP, IUFD and casesto
leading in awhichhighparents
17 (65.4%) TGA type,
opted and
intrauterine
four (15.4%) AVSD
(91.1%) fetusesnon-committed
two (7.7%)
of DORV
typepostnatal
with DORV hadVSD
and their postnatal hemodynamic
with heterotaxy (Figures 3 and 4).
andadditional cardiac lo
major
ap
for compassionate care, the “intention-to-treat group” One of those eight infants had an additiona al
(91.1%) fetuses with DORV had major additional cardiac loss rate due to terminations or declined postnatal Ingo Gottschalk
ther-
and Judith S. Abel contributed equally to this work.
a
consisted of 22 fetuses, all were born alive (Table 2). artery anomaly and died at the
*Corresponding author: Dr. med. Ingo Gottschalk, Bereich
age of 15 ve
da
apy. Without additional anomalies, the prognosis is good,
für Pränatale Medizin und Gynäkologische Sonographie,
Twenty-one of those infants already underwentDiscussion surgery, of low cardiac Köln,
Universitätsfrauenklinik output failure
Kerpenerstr. 34, 50931after
Cologne,aortic Ke a
a
Ingo Gottschalk and Judith S. Abel contributed equally to this work. although approximately 60% of children will have
Germany; single
and Division of Prenatal Medicine, University of Cologne, ve
three died and 18 survived. One infant is still awaiting
Figure 3: DORV, VSD type, with subaortic VSD and overriding aorta. struction andE-mail:
Cologne, Germany, banding of pulmonary arteries
ingo.gottschalk@uk-koeln.deDiagnostic postnatal • Identification/confirmation du type de VDDI – Type CIV sousaortique -> chir 3-6 mois – Type TGV -> chir néonatal – Type Fallot -> chir 3-6 mois – Uncomitted –> open to discussion • Description des lésions associées – Sténose sous-pulmonaire – Sténose sous-aortique – Cleft ou fente mitrale – Straddling (mitral, tricuspide, les 2) – Hétérotaxie: VDDI-CAVc
Diagnostic préopératoire Les enjeux de l’imagerie
Objectif de l’imagerie
• Comprendre l’anatomie du VDDI
• Décrire toutes les lésions anatomiques de la
position de la CIV jusqu’aux anomalies associées
• Décider d’une stratégie thérapeutique adaptée à
l’anatomie
En pratique
Comment faut-il réparer le cœur ?Que veut savoir le chirurgien?
Réparation uni- ou biventriculaire ?
– Hypoplasie d’un des ventricules
– CIV multiples non accessibles ou partiellement
accessibles
– Anomalies des insertions des valves
atrioventriculaires à travers la CIV p.ex.
straddling ou insertion complexe
FONTAN Intraventricular baffle repair
+/- Switch operationQue veut savoir le chirurgien?
Relation de la CIV avec les gros vaisseaux:
– Sous-aortique
– Sous-pulmonaire
– Doubly-committed
– Non committed
En pratique
Comment créer un tunnel VG vers la valve sigmoïde la
plus proche sans obstacle sous-aortique ?Que veut savoir le chirurgien?
• Eléments clés du tunnel VG-aorte:
– Distance entre la valve tricuspide et la valve pulmonaire
pour faire passer le tunnel sans obstacle
– Nécessité d’élargissement de la CIV (diamètre CIV = aorte)
• Etat de la voie pulmonaire: valve normale, sténose ou
atrésie…
Est-ce qu’elle peut être utilisée
en position pulmonaire [patch infundibulaire]
ou en aortique [Switch]
ou faut-il la reconstruire [REV, Nikaidoh, Rastelli…]?Modalités d’imagerie
Imagerie 3D
Echographie 2 D Printing 3D D
Scanner/IRM cardiaque
La base d’aujourd’hui
Le complément d’imagerie
L’ avenir ?Imagerie en coupe Scanner/IRM • Intérêt du scanner en préopératoire – Coronaires (rotation troncale/ Bex Nikaidoh) – Artères pulmonaires – Collatérales aorto-pulmonaires – retours veineux systémiques et pulmonaires • Intérêt de l’IRM: – Taille des ventricules – Evaluation fonctionnelle
VDDI et CIV sous-aortique
Celui qui ne pose pas/peu de problème
VSD-type DORVVDDI et CIV sous-aortique
Tu
n
ne
lVDDI + CIV sous-aortique
AO
AP
VG
VDVDDI + CIV sous-pulmonaire
Celui qu’il faut réparer comme une
TGV plus ou moins complexe
TGA-type DORVVDDI + CIV sous-pulmonaire
Aorte
AP
Tunnel
Switch artériel
Tunnel VG-néo-ao
Chen et al. 2008VDDI + CIV sous-pulmonaire
VDDI + CIV non committed
Celui pour lequel la décision
thérapeutique peut être complexe…AP
VD
Ao
VG APDevenir après réparation
Complications à long terme • Sténose sous-aortique (tunnel VG-aorte) • Réfection voie droite (sténose, fuite avec dilatation VD, changement de tube ..) • Complications coronaires (switch) • Dysfonctionnement des valves atrioventriculaires
Impact of anatomic characteristics and initial biventricular
surgical strategy on outcomes in various forms of
double-outlet right ventricle
• Early outcome (< 30 days):
Olivier Villemain, MD,a Emre Belli, MD,b Magalie Ladouceur, MD,a Lucile Houyel, MD,b
Zakaria Jalal, MD,a Virginie Lambert, MD, PhD,c Mohamed Ly, MD,b Pascal Vouh!e, MD, PhD,a and
Damien– Bonnet,
Mortality:
MD, PhDa 7,4%
– Reoperation
ABSTRACT (cardiac indications): 6% n = 433
Objectives: Surgical management of various forms of double-outlet right
ventricle uses a variety of approaches depending on the underlying anatomic
form. In this study, we sought to determine the risk factors of mortality and
reoperation in those with double-outlet right ventricle undergoing biventricular 10 years : 86,2%
repair, according to anatomic characteristics and initial surgical strategy.
Methods: Between 1992 and 2013, 433 patients were included in the study.
Double-outlet right ventricle was classified as double-outlet right ventricle with
subaortic ventricular septal10defect
years :associated
38,2% with subpulmonary obstruction in Freedom from reoperation according
33% of patients (n ¼ 141), with subaortic ventricular septal defect without strategy.
subpulmonary obstruction in 30% of patients (n ¼ 130), with subpulmonary
ventricular septal defect in 32% of patients (n ¼ 139), and with noncommitted Central Message
ventricular septal defect in 5% of patients (n ¼ 23). Three types of repairs The initial surgical strategy did no
late outcomes of DORV with bi
were performed: (1) intraventricular baffle repair, n ¼ 149 (34%); (2) intraven- repair.
tricular baffle repair with right ventricular outflow tract reconstruction, n ¼ 163
(38%); and (3) intraventricular baffle repair with arterial switch operation, Perspective
n ¼ 121 (28%). The outcomes of DORV with bi
Results: Thirty-day overall mortality was 7.4%. Early reoperation was needed in repair remain unclear. Between
2013, 433 consecutive patients were
6% of the cases. Early mortality was higher in the intraventricular baffle repair tively included. Early mortality wa
with arterial switch operation group (P ¼ .01). Survival at 10 years was 86.2%, the IVR-ASO group. Late mortality a
and freedom from reoperation at 10 years was 61.4%. At last follow-up (median, operation rates were similar in the d
5.7 years; 95% confidence interval, 4.5-6.6), mortality and reoperation rates were ventricular surgical strategy groups
similar in the different surgical strategy groups. Late reoperation and late
JTCS 2016 Villemain et al.
significantly higher in DORV witImpact of anatomic characteristics and initial biventricular
surgical strategy on outcomes in various forms of
double-outlet right ventricle
Olivier Villemain, MD,a Emre Belli, MD,
Non committed
b
VSD Magalie
Type Ladouceur, MD,a Lucile Houyel, MD,b
Zakaria Jalal, MD,a Virginie Lambert, MD, PhD,c Mohamed Ly, MD,b Pascal Vouh! e, MD, PhD,a and
Damien Bonnet, MD, PhDa
ABSTRACT
Objectives: Surgical management of various forms of double-outlet right
ventricle uses a variety of approaches depending on the underlying anatomic
form. In this study, we sought to determine the risk factors of mortality and
reoperation in those with double-outlet right ventricle undergoing biventricular
repair, according to anatomic characteristics and initial surgical strategy.
Methods: Between 1992 and 2013, 433 patients were included in the study.
Double-outlet right ventricle was classified as double-outlet right ventricle with
subaortic ventricular septal defect associated with subpulmonary obstruction in Freedom from reoperation according
33% of patients (n ¼ 141), with subaortic ventricular septal defect without strategy.
subpulmonary obstruction in 30% of patients (n ¼ 130), with subpulmonary
ventricular septal defect in 32% of patients (n ¼ 139), and with noncommitted Central Message
ventricular septal defect in 5% of patients (n ¼ 23). Three types of repairs The initial surgical strategy did no
late outcomes of DORV with bi
were performed: (1) intraventricular baffle repair, n ¼ 149 (34%); (2) intraven- repair.
tricular baffle repair with right ventricular outflow tract reconstruction, n ¼ 163
(38%); and (3) intraventricular baffle repair with arterial switch operation, Perspective
n ¼ 121 (28%). The outcomes of DORV with bi
Results: Thirty-day overall mortality was 7.4%. Early reoperation was needed in repair remain unclear. Between
2013, 433 consecutive patients were
6% of the cases. Early mortality was higher in the intraventricular baffle repair tively included. Early mortality wa
with arterial switch operation group (P ¼ .01). Survival at 10 years was 86.2%, the IVR-ASO group. Late mortality a
and freedom from reoperation at 10 years was 61.4%. At last follow-up (median, operation rates were similar in the d
5.7 years; 95% confidence interval, 4.5-6.6), mortality and reoperation rates were ventricular surgical strategy groups
similar in the different surgical strategy groups. Late reoperation and late
JTCS 2016 Villemain et al.
significantly higher in DORV witImpact of anatomic characteristics and initial biventricular
surgical strategy on outcomes in various forms of
double-outlet right ventricle
Olivier Villemain, MD,a Emre Belli, MD,b Magalie Ladouceur, MD,a Lucile Houyel, MD,b
Zakaria Jalal, MD,a Virginie Lambert, MD, PhD,c Mohamed Ly, MD,b Pascal Vouh!e, MD, PhD,a and
Damien Bonnet, MD, PhDa
ABSTRACT
Objectives: Surgical management of various forms of double-outlet right
ventricle uses a variety of approaches depending on the underlying anatomic
Non committed
form. In this study, VSD
we sought to Type
determine the risk factors of mortality and
reoperation in those with double-outlet right ventricle undergoing biventricular
repair, according to anatomic characteristics and initial surgical strategy.
Methods: Between 1992 and 2013, 433 patients were included in the study.
Double-outlet right ventricle was classified as double-outlet right ventricle with
subaortic ventricular septal defect associated with subpulmonary obstruction in Freedom from reoperation according
33% of patients (n ¼ 141), with subaortic ventricular septal defect without strategy.
subpulmonary obstruction in 30% of patients (n ¼ 130), with subpulmonary
ventricular septal defect in 32% of patients (n ¼ 139), and with noncommitted Central Message
ventricular septal defect in 5% of patients (n ¼ 23). Three types of repairs The initial surgical strategy did no
late outcomes of DORV with bi
were performed: (1) intraventricular baffle repair, n ¼ 149 (34%); (2) intraven- repair.
tricular baffle repair with right ventricular outflow tract reconstruction, n ¼ 163
(38%); and (3) intraventricular baffle repair with arterial switch operation, Perspective
n ¼ 121 (28%). The outcomes of DORV with bi
Results: Thirty-day overall mortality was 7.4%. Early reoperation was needed in repair remain unclear. Between
2013, 433 consecutive patients were
6% of the cases. Early mortality was higher in the intraventricular baffle repair tively included. Early mortality wa
with arterial switch operation group (P ¼ .01). Survival at 10 years was 86.2%, the IVR-ASO group. Late mortality a
and freedom from reoperation at 10 years was 61.4%. At last follow-up (median, operation rates were similar in the d
5.7 years; 95% confidence interval, 4.5-6.6), mortality and reoperation rates were ventricular surgical strategy groups
similar in the different surgical strategy groups. Late reoperation and late
JTCS 2016 Villemain et al.
significantly higher in DORV witImpact of anatomic characteristics andVillemain
initial biventricular
et al
surgical strategy on outcomes in various forms of
double-outlet right ventricle
Olivier Villemain, MD,a Emre Belli, MD,b Magalie Ladouceur, MD,a Lucile Houyel, MD,b
Zakaria Jalal, MD,a Virginie Lambert, MD, PhD,c Mohamed Ly, MD,b Pascal Vouh!e, MD, PhD,a and
Damien Bonnet, MD, PhDa
ABSTRACT
Objectives: Surgical management of various forms of double-outlet right
ventricle uses a variety of approaches depending on the underlying anatomic
form. In this study, we sought to determine the risk factors of mortality and
reoperation in those with double-outlet right ventricle undergoing biventricular
repair, according to anatomic characteristics and initial surgical strategy.
Methods: Between 1992 and 2013, 433 patients were included in the study.
Double-outlet right ventricle was classified as double-outlet right ventricle with
subaortic ventricular septal defect associated with subpulmonary obstruction in Freedom from reoperation according
33% of patients (n ¼ 141), with subaortic ventricular septal defect without strategy.
subpulmonary obstruction in 30% of patients (n ¼ 130), with subpulmonary
ventricular septal defect in 32% of patients (n ¼ 139), and with noncommitted Central Message
ventricular septal defect in 5% of patients (n ¼ 23). Three types of repairs The initial surgical strategy did no
late outcomes of DORV with bi
were performed: (1) intraventricular baffle repair, n ¼ 149 (34%); (2) intraven- repair.
tricular baffle repair with right ventricular outflow tract reconstruction, n ¼ 163
(38%); and (3) intraventricular baffle repair with arterial switch operation, Perspective
n ¼ 121 (28%). The outcomes of DORV with bi
Results: Thirty-day overall mortality was 7.4%. Early reoperation was needed in repair remain unclear. Between
2013, 433 consecutive patients were
6% of the cases. Early mortality was higher in the intraventricular baffle repair tively included. Early mortality wa
with arterial switch operation group (P ¼ .01). Survival at 10 years was 86.2%, the IVR-ASO group. Late mortality a
and freedom from reoperation at 10 years was 61.4%. At last follow-up (median, operation rates were similar in the d
5.7 years; 95% confidence interval, 4.5-6.6), mortality and reoperation rates were ventricular surgical strategy groups
similar in the different surgical strategy groups. Late reoperation and late
JTCS 2016 Villemain et al.
significantly higher in DORV witthe study.
Impact of anatomic characteristics and initial biventricular
surgical strategy on outcomes in various forms of
ntricledouble-outlet
with right ventricle
struction
Olivierin
Freedom from reoperation according to surgical
a b
Villemain, MD, Emre Belli, MD, Magalie Ladouceur, MD, Lucile Houyel, MD,
a c
a
b
b
a
ect without strategy.
Zakaria Jalal, MD, Virginie Lambert, MD, PhD, Mohamed Ly, MD, Pascal Vouh!
Damien Bonnet, MD, PhD a
e, MD, PhD, and
bpulmonaryABSTRACT
Objectives: Surgical management of various forms of double-outlet right
ncommitted Central Message
ventricle uses a variety of approaches depending on the underlying anatomic
form. In this study, we sought to determine the risk factors of mortality and
reoperation in those with double-outlet right ventricle undergoing biventricular
of repairs The initial surgical strategy did not influence
repair, according to anatomic characteristics and initial surgical strategy.
late outcomes of DORV with biventricular
Methods: Between 1992 and 2013, 433 patients were included in the study.
2) intraven- repair.
Double-outlet right ventricle was classified as double-outlet right ventricle with
subaortic ventricular septal defect associated with subpulmonary obstruction in Freedom from reoperation according
33% of patients (n ¼ 141), with subaortic ventricular septal defect without strategy.
n, n ¼ 163
subpulmonary obstruction in 30% of patients (n ¼ 130), with subpulmonary
ventricular septal defect in 32% of patients (n ¼ 139), and with noncommitted Central Message
operation, Perspective
ventricular septal defect in 5% of patients (n ¼ 23). Three types of repairs
were performed: (1) intraventricular baffle repair, n ¼ 149 (34%); (2) intraven-
The initial surgical strategy did no
late outcomes of DORV with bi
repair.
tricular baffle repair with right ventricular outflow tract reconstruction, n ¼ 163
(38%); and (3) intraventricular baffle repair with arterial switch operation, Perspective
n ¼ 121 (28%). The outcomes of DORV with biventricular The outcomes of DORV with bi
Results: Thirty-day overall mortality was 7.4%. Early reoperation was needed in repair remain unclear. Between
6% of the cases.repair remain unclear. Betweenbaffle 1992
repair and
s needed in
2013, 433 consecutive patients were
Early mortality was higher in the intraventricular tively included. Early mortality wa
with arterial switch operation group (P ¼ .01). Survival at 10 years was 86.2%, the IVR-ASO group. Late mortality a
and freedom from 2013, 433at consecutive
reoperation 10 years was 61.4%. patients were (median,
At last follow-up retrospec- operation rates were similar in the d
affle repair
Survival
5.7 years; 95% confidence interval, 4.5-6.6), mortality and reoperation rates were
FIGURE
similar tively
in the 2. included.
Outcomes
different according
surgical Early
to
strategy groups.mortality
surgical strategy. wasand
A, Survival
Late reoperation
JTCS
higher
according
late
ventricular surgical strategy groups
2016 Villemain et al.
in
significantly higher in DORV witcommitted
mbranous)Double-Outlet Right Ventricle With
Noncommitted Ventricular Septal Defect and
ters. Right
2 Adequate Ventricles: Is Anatomical Repair
sNCVSD
(50%). 2AADEQUATE VENTRICLES
Advantageous?
AND
Anatomical * *
Olivier Villemain, MD, Damien Bonnet, MD, PhD, Lucile Houyel, MD, Mathieu Vergnat, MD †
Magalie Ladouceur, OverallMD, survival*
Virginie(2A) and freedom
Lambert, MD, Zakaria
†
of reoperation (2B) Pascal Vouhé, MD, P
Jalal, MD, PhD, *
performed
and Emre Belli, MD ‡
according to surgical strategy
and arterial
The management of double-outlet right ventricle associated with anatomically
noncommitted ventricular septal defect constitutes a surgical challenge. The
limits for, and the specific outcomes after anatomical vs univentricular repair
defect still
was remain to be established. Between 1993 and 2011, 36 consecutive
patients presenting Central Messageright ventricle or noncommitted
with double-outlet
underwentventricular septal defect (21 inlet, 10 muscular, and 5 central perimembranous)
and 2 adequately sized ventricles underwent surgical repair at 2 centers. Right
ventricular outflow Anatomical
tract obstructionrepair,
was present associated with
in 18 of 36 patients substantial
(50%). A
all in group
total of 21 patients had undergone previous palliative procedures. Anatomical
repair (group I) by rates
Overall survival (2A) and freedom of reoperatio
means of of mortality
intraventricular and
baffle need
construction for reoperation,
was performed according to surgical strategy
underwentin 24 (associated right ventricular outflow tract reconstruction in 12 and arterial
should be considered with caution.
switch in 5) at a median age of 10.5 months. Ventricular septal defect was Central Message
surgically enlarged in 12 (50%) patients. The remaining 12 patients underwent
sis wasuniventricular
the repair (group II). There were 4 hospital deaths (11%), all in group
I (P ¼ 0.30 vs group II). A total of 8 of 20 patients in group I survivors underwent
Anatomical repair, associated with subs
rates of mortality and need for reope
should be considered with caution.
h in group I for reoperation
13 reoperations after a median delay of 24 months: subaortic stenosis was the
main cause
Perspective Statement
in 6 of 8 patients. There was 1 late death in group I Perspective Statement
and 2 late deaths in group II. The median follow-up was 5.6 years (95% CI:
s (95%0.2-9.8).
CI:The 10- year actuarialFigure survival rate and freedom from reoperation The surgical management of DORV
2. Overall survival (A) and freedom of reoperation (B) according to surgical strategy.
were 74.7 ! 5% and 58 ! 5% in group I and 71 ! 7% and 70 ! 7% in group
NCVSD constitutes a challenge. Be
The surgical
visit, all management
figure is available online.) of York
DORV Heart with
1993 and 2011, 36 consecutive patient
eoperationN=36; 1993-2011
II, respectively. At the last survivors were in New
Association class I-II. Univariate analysis showed that atrioventricular septal
senting with DORV or NCVSD and 2
quately sized ventricles underwent su
defect and isolated NCVSD constitutes
associated withadeath
DISCUSSION
mitral cleft were challenge. Between
(P ¼ 0.04) and need
STCS 2016 Villemain
the selection et al.
criteria according to
repair at 2 centers. Anatomical repair in D
% in group
for reoperation (P ¼ 0.038). In conclusion, anatomical
The classification repair,
of the associated
conotruncal with
anomalies with NCVSD should be considered wit
omy of the VSD and its relation to
tion. Associated AVSD or isolated mitraConclusion Les VDDI imposent – Une bonne vision dans l’espace – Une analyse génétique – Une analyse anatomo-échographique – Une analyse anatomo-physiologique – Une discussion médico-chirurgicale – Un bon suivi
Vous pouvez aussi lire