Acrosyndromes vasculaires phénomène de Raynaud prise en charge par le médecin vasculaire - Joël Constans Hôpital St André, CHU Bordeaux et ...
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous

Acrosyndromes vasculaires
phénomène de Raynaud
prise en charge par le médecin vasculaire
Joël Constans
Hôpital St André, CHU Bordeaux et
Université de Bordeaux
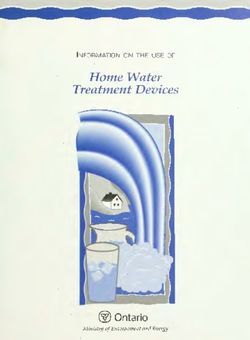
Défini:on
Microcircula:on cutanée
J Constans, EMC ermato_cosmeto, 2007
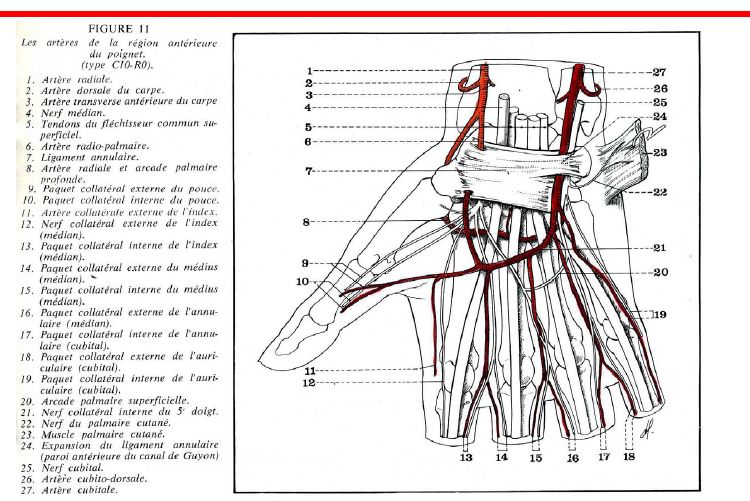
Arcades palmaires
Classifica:on des acrosyndromes
Diagnos:c différen:el du phénomène de
Raynaud
• Ischémie digitale
• Hématome digital spontané
• Engelures
• acrocyanose
engelures Hématome digital
spontané
Recommenda)on 1: Raynaud’s Phenomenon is the correct term for this disorder. It may take the form of Primary Raynaud’s Phenomenon or Secondary Raynaud’s Phenomenon. Recommenda)on 2 The terms Primary Raynaud’s Phenomenon and Secondary Raynaud’s Phenomenon should be used and the terms ‘syndrome’ and ‘disease’ discarded. Level C, Grade IIa
Diagnos:c de phénomène de Raynaud • Souvent aisé • Ischémie des extrémités • ParoxysCque • Phases blanc, (bleu), (rouge) • Peut être facilité par des photos • Le principal problème • PrimiCf? • Secondaire?
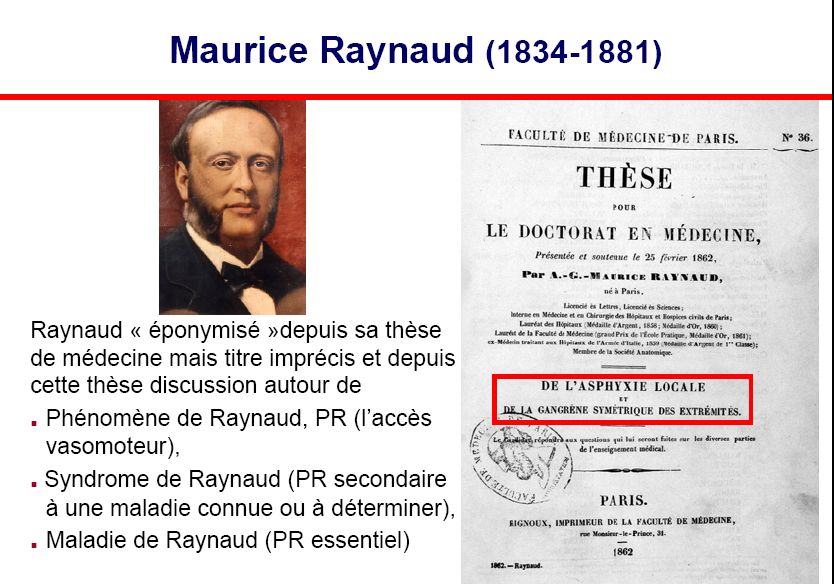
Table 1 The condiCons which may be associated with secondary RP. ConnecCve Tissue Disorders Endocrine • Systemic Sclerosis •Hypothyroidism • Systemic Lupus Erythematosus •Pheochromocytoma • Mixed CTD • Sjögren’s Syndrome • DermatomyosiCs/PolymyosiCs ParaneoplasCc (eg carcinoid) • Primary Biliary Cirrhosis (oYen with underlying SSc) Miscellaneous OccupaConal • Buerger’s disease (ThromboangiiCs obliterans) • Hand Arm VibraCon Syndrome and Hypothenar Hammer Syndrome •Low BMI • Vinyl Chloride Monomer exposure • Silica and solvents (causing systemic sclerosis) Drugs • AnC-migraine drugs eg ergot derivaCves • Non-selecCve β Blockers, including eye drops • Some Cytotoxic drugs • Cyclosporin (though may be obstrucCve especially in transplant paCents) • BromocripCne • Interferon α and β • Cocaine or amphetamine abuse, cannabis • Estrogen replacement therapy without progesterone • Ephedrine eg in Ear Nose and Throat preparaCons
Table 3: Condi)ons where microvascular occlusion may mimic Raynaud’s and
should be excluded
Occlusive vascular disease
• Embolism (eg from thoracic outlet syndrome)
Haematological
• Malignancies
• Cryo diseases (cryoglobulinaemia, cryofibrinogenaemia and cold aggluCnin disease)
• Hyperviscosity Syndromes
InfecCon
• HepaCCs associated vasculiCs
AggluCnines froidesRecommenda)on 3 Condi)ons associated with RP should be divided into true associated disorders with e)ological links; those which worsen RP or precipitate its appearance; and those which do not cause vasospasm but digital necrosis. Level C, Grade III Recommenda)on 4 A thorough history and examina)on should be taken from all pa)ents presen)ng in Primary Care to ensure correct diagnosis of any underlying condi)on, as early diagnosis and organ screening in CTD improves outcome. Level C, Grade IIa
Critères évoquant un PR secondaire • Absence de rémission esCvale complète • Pouces touchés • Survenue après 35 ans • Phase bleue prolongée • Caractère unilatéral persistant • Absence de trouble trophique • Sexe masculin
Recommenda)on 5 All pa)ents presen)ng with RP should undergo blood tests including full blood count, ESR or CRP, and ANA tes)ng, and capillaroscopy when available. Level C, Grade IIa Recommenda)on 6 Capillaroscopy should only be carried out using equipment of good op)cal quality and by an experienced operator, usually in Secondary or Ter)ary Care. Level C, Grade IIa Recommenda)on 7 Capillary microscopy is a useful diagnos)c tool. Abnormal capillary paTerns are strong predictors of CTD, and should be employed by Secondary Care. Level A, Grade IIa
Capillaroscopie: quel matériel?
• Pour faire une capillaroscopie, il faut un capillaroscope
• Videocapillaroscope= opCmal
• Capillaroscope « tradiConnel »
• Pas de mesure de densité ou de diamètre
• Pas de possibilité de stockage d’images
• Autres techniques?
Mais problème de grossissement, pas de mesures, pas de valida:on
• Capteurs opCques reliés à un système numérique
• dermatoscopeQuel grossissement u:liser?
• Etre habitué à son grossissement
• X100 le plus répandu
• X50: meilleure vue d’ensemble du lit capillaire mais repères
différents
• X200-350:
• réalisa)on plus difficile
• Quelle zone d’intérêt?
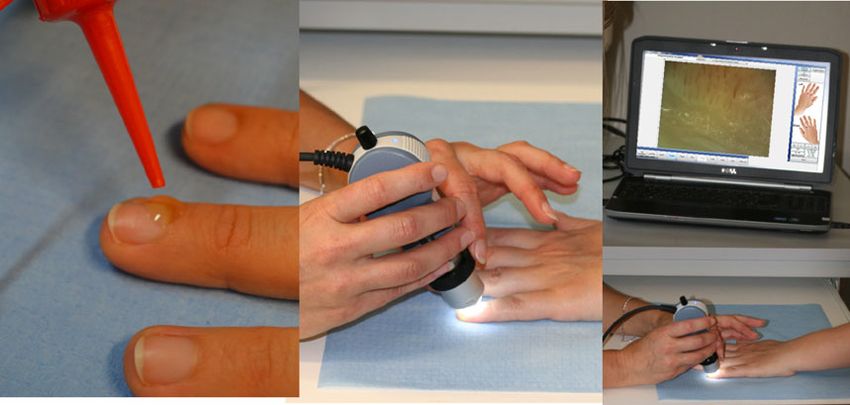
• Plus de variabilité? Perte d’informa)onsConduite de l’examen capillaroscopique • Pièce tempérée • Malade au calme, pas de soins de manucurie récent, difficultés chez les travailleurs manuels • Posi)on assise • GouTe d’huile sur le rebord péri-unguéal • Examiner tous les doigts sauf le pouce, les 2 mains • Garder des images
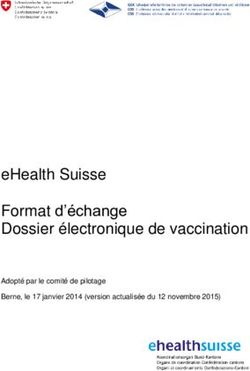
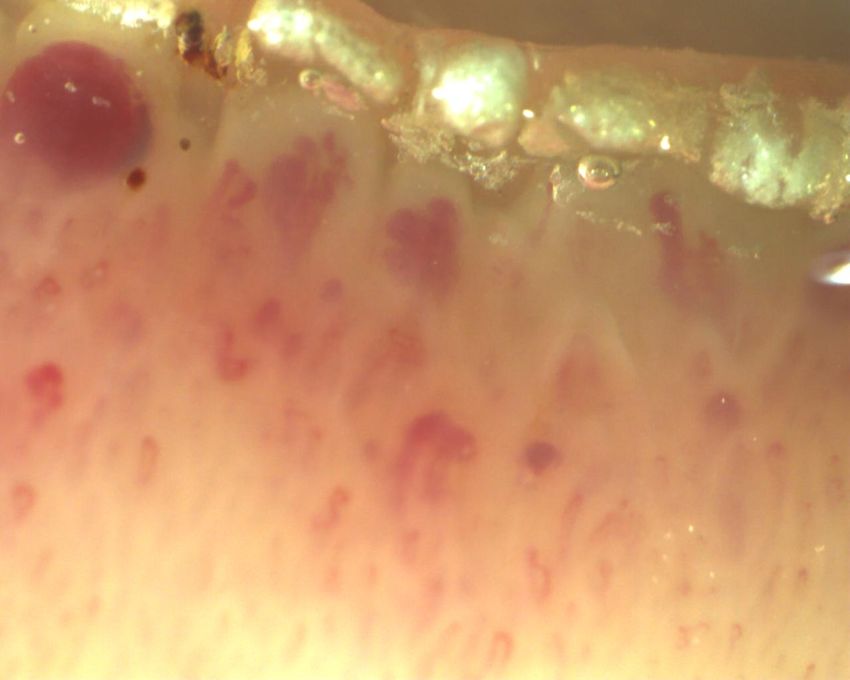
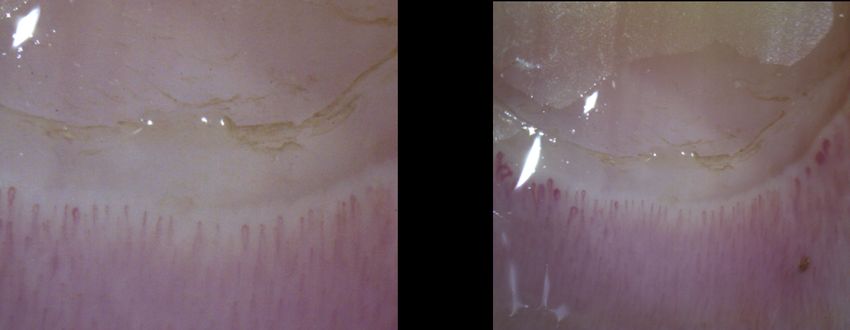
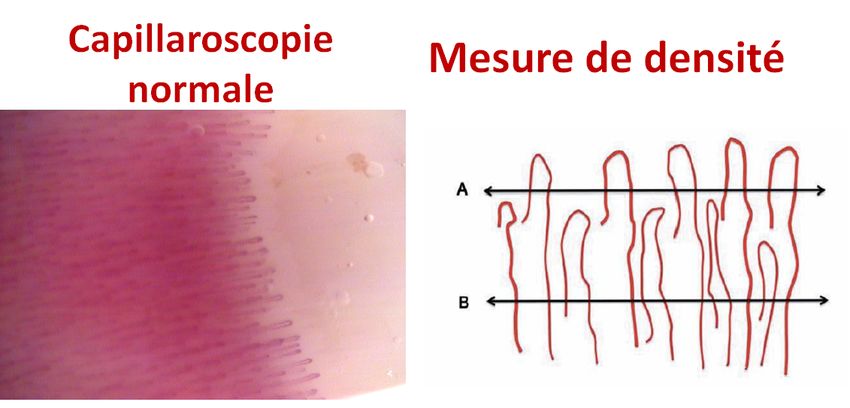
Différentes étapes de la capillaroscopie • Regarder l’ensemble du paysage • Œdème • Hémorragies • DésorganisaCon architecturale • Mesurer la densité capillaire • N≥8/mm; détecter les plages avasculaires? (
Paysage Paysage normal sclérodermique
Sensibility of scleroderma paIern in SSc
Prevalence of SSc landscape in
confirmed SSC
Maricq 1980 82%
(N=173)
Vayssairat 1981 94%
(N= 74)
Granier 1986 93%
(N=30)
Blockmans 1996 73-100%
(N=42)
Ohtsuka 1994 90%
(N=55)
Cutolo 2004 99%
(N=241)
86% (N=2754): cohorte EUSTAR (Ingegnoli 2013)
Adapted from Atlas de Capillaroscopie, Collège des Enseignants de
Médecine VasculaireFollow-up of Raynaud’s phenomenon
Series RP Suspect RP Follow-up Confirmed CTD
years during follow-up
Priollet 1987 240 26 (clinics or ANA) 6 50%
Lugen 1995 64 64 (clinics or ANA) 8 50%
Spencer 1998 639 262 (clinics or ANA) 4 30%
Meli 2006 1024 168 (capillaroscopy) 6.5 82%
Koenig 2008 784 133 (capillaroscopy or ANA) 15 50%
Adapted from Atlas de Capillaroscopie, Collège des Enseignants de Médecine VasculaireRheumatology (Oxford). 2017 Oct 1;56(10):1780-1783.
Recommenda)on 8
Children under the age of 12 should be referred to Secondary Care as PRP is less
common in these age groups
Level C, Grade IIa
Recommenda)on 9
Pa)ents with RP should be referred to Secondary Care when
• There is evidence of an associated disorder or of occlusive vascular disease
• Symptoms are severe or progressing despite first line lifestyle and drug
treatment
Level C, Grade IIaRecommenda)on 10 Lifestyle change is an effec)ve means of controlling RP aTacks and should include avoiding triggers such as cold, dressing warmly, ceasing smoking, and an Occupa)onal Therapy assessment for aids if difficul)es are reported. Level C, Grade IIa Recommenda)on 11 Calcium channel blockers are the recommended first line drug treatment for RP, if life-style modifica)on alone has failed. Level A, Grade 1 Recommenda)on 12 Nifedipine in slow release form should be used to minimise debilita)ng vasodilatory side effects and short dura)on of ac)on. Care should be taken to increase dosage by increments to avoid side effects. If side effects are not severe pa)ents should be encouraged to tolerate them for 2 – 3 weeks as they may subside. Level C, Grade IIa
Vous pouvez aussi lire