Cancer de vessie du Sujet Agé - DIU Oncogériatrie 2021 Pr Lotz - Yann-Alexandre Vano - Longue Vie et Autonomie
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous
DIU Oncogériatrie 2021 Pr Lotz
Cancer de vessie du Sujet Agé
Yann-Alexandre Vano
Oncologie Médicale
Hôpital Européen Georges Pompidou, AP-HP
INSERM 1138, Centre des Cordeliers, Paris
Liens d’intérêts Honoraires pour advisory board • Ipsen, BMS, Roche, Pfizer, Sanofi, Janssen, Novartis, MSD, Astellas
Plan • Epidémiologie (brève) • Prise en charge médicale des carcinomes urothéliaux • TVIM • Formes métastatiques • Données chez le sujet âgé • Messages clés
Epidémiologie (brève)
Cancer chez le sujet âgé en France (2017)
249 000 cas 115 000 décès
>65 ans
62% 75%
Essais Rando EORTC: Sur >6 000 pts, 9% ont 70 ans et plus è TRIAL PARADOX
Quinten C et al., Eur J Cancer 2015
https://www.e-cancer.fr/ressources/cancers_en_france/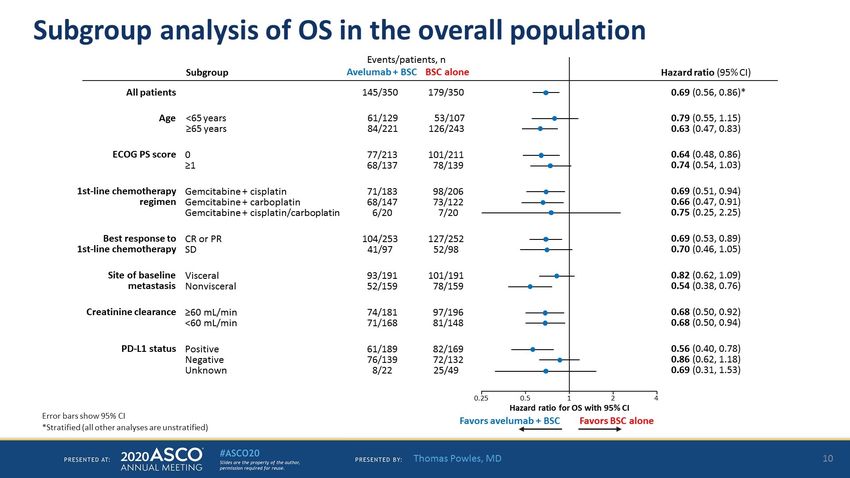
Le cancer 2de vessie est une maladie du sujet âgé
JO U R N A L OF GE RI A TRI C O N COL O G Y 6 (2 0 1 5) 1 –
75% What else do we n
management? There
45% and physical that m
making, most of whic
of any patient, but so
the elderly patient. H
What is the patient's
social support system
she prepare her own
she taking and who
organ function been
Fig. 1 – Age distribution of new bladder cancer diagnoses in these domains are li
the United States (data derived from the Surveillance, Comprehensive Geria
Epidemiology, and End Results Program*). geriatrics consultation
*http://seer.cancer.gov/statfacts/html/urinb.html. ascertained through a
As we dig a bit dee
Matthew Galsky, J of Geria Oncol 2015
and even mortality. A radical cystectomy with pelvic lymph mild dementia. She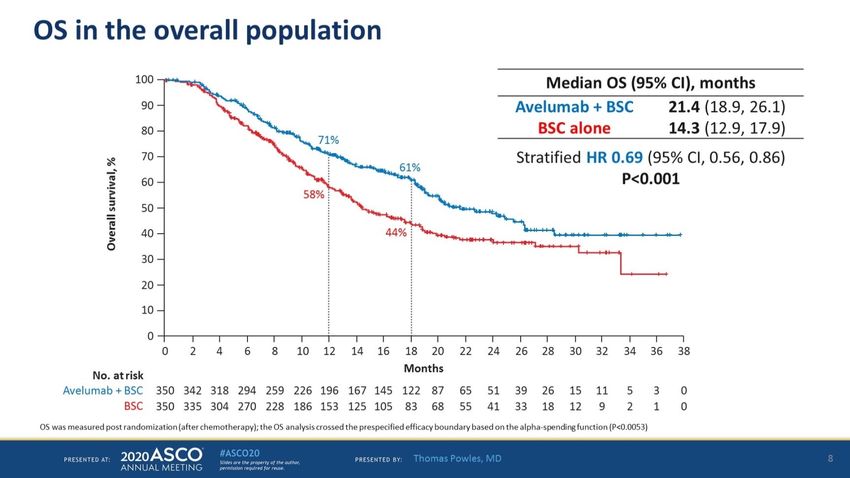
Evolution cancers de vessie 1990-2013
Age 1990 2013 Var
Incidence (%) 60-69 29 24 -5%
70+ 49 56 +7%
Mortalité (%) 60-69 26 20 -6%
70+ 56 64 +8%
Dy G. et al, Euro Urol 2017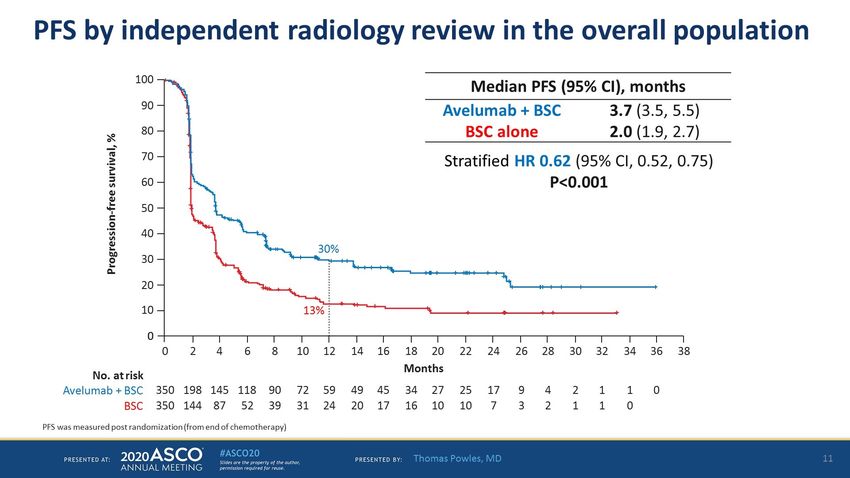
Prise en charge du cancer de vessie dans la pop. générale
Vue d’ensemble
T. LOCALISEES
TVNIM Tt local
Bon pronostic à court terme
70% à Récidives multiples à TVIM
TVIM CT néoadj puis cystectomie
Mauvais pronostic
30% à Progression métastatique
T. METASTATIQUES
= pronostic effroyable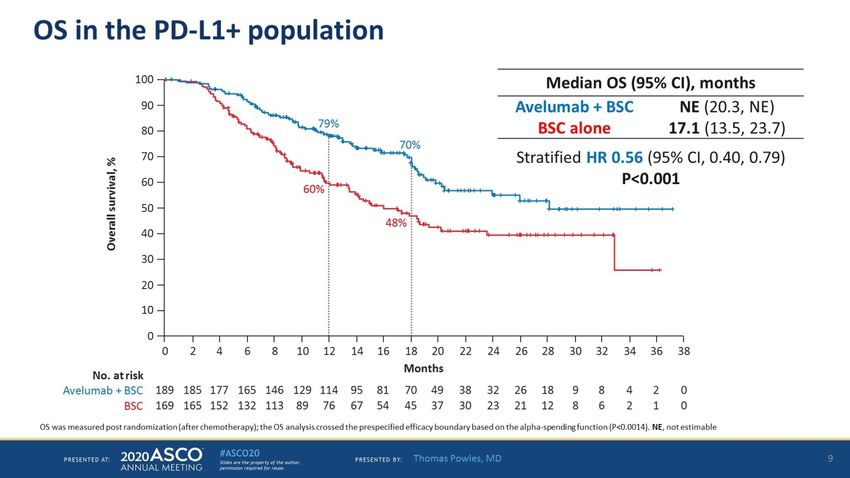
Tumeurs localisées infiltrant le muscle (TVIM)
TVIM
TVIM Chimiothérapie
Staging+++ CYSTECTOMIE
néoadjuvante (CNA)
RTUV pT2-4cN0M0
2-3 mois
RADICALE (60mL/min problématiques:
Chimiothérapie
Pas de perte auditive - Délais avant CT
Pas de neuropathies sensitives adjuvante (CA) - DFG dim.
Fonction cardiaque préservée
Objectif CNA: réponse complète pathologique (pT0)Chimiothérapie néoadjuvante Oui
§ Recommandation des sociétés savantes européennes
(ESMO, EAU) et américaine (NCCN)
§ cT2, T3, T4 et NÀ
§ A base de cisplatine :
§ cisplatine-gemcitabine: J1-J8, reprise à J21 (4 cycles)
§ MVAC intensifié: J1 = J15 (4 à 6 cycles)
§ Pas de place pour le carboplatine +++
2 phases II (n=44 et n=39), MVAC intensifié (4 cycles)
ORR 52% à 38% pT0
ORR 77% à 28% pT0
Pour le NA, c’est le %pT0 qui importe
12Chimiothérapie adjuvante
§ Recommandation des sociétés savantes européennes
(ESMO, EAU) et américaine (NCCN)
§ Indications:
§ Si traitement néoadjuvant: pas d’indication
§ En l’absence de traitement néoadjuvant: T3, T4, N+
§ A base de cisplatine :
§ cisplatine-gemcitabine: J1-J8, reprise à J21 (4 cycles)
§ (MVAC intensifié: J1 = J15)
§ Pas de place pour le carboplatine +++
Ruggeri et al, Cancer 2006 ; 15 :783 - 8
13Protocole VESPER (étude GETUG)
Objectif: Comparaison dd-MVAC vs GC en péri-
opératoire (A ou NA)
Cisplatine 70mg/m2 J1 Methotrexate 30mg/m2
Gemcitabine 1250mg/m2 J1J8 Vinblastine 3mg/m2
J1-J21 4 cycles Adriamycine 30mg/m2
Cisplatine 70mg/m2
J1-J15 6 cyclesProtocole VESPER (étude GETUG)
Adjuvant: Néo-adjuvant:
CT complète CT complète
GC 46% GC 66%
MVAC 37% MVAC 58%
Meilleure dose-intensité pour la CNA vs AProtocole VESPER (étude GETUG)
Taux de réponse pathologique Effets indésirables G3-4
GC dd-MVAC p value
GC dd-MVAC p value (n = 245) (n = 248)
(n = 198) (n = 199) Nausea/vomiting 7 (2.9%) 24 (9.7%) 0.003
Diarrhea 2 (0.81%) 3 (1.2%) –
Complete response
Asthenia 10 (4.1%) 35 (14%) 0.9
Non-muscle invasive Kidney 13 (5.3%) 15 (6.0%) 0.9Tumeurs métastatiques Objectifs: prolongement vie et amélioration/maintien QDV
Facteurs pronostic du cancer de la vessie avancé Classification la plus connu : Bajorin (1999) • Performance status : (0 ou 1 vs 2) • Nombre d’organes métastatiques : (1 vs 2 ou +) En fonction du nombre de facteur (0-1-2) : • 0 facteur pg = 33 mois, survie à 5 ans = 33 % • 1 facteur pg = 17 mois, survie à 5 ans = 15 % • 2 facteurs pg = 9 mois, survie à 5 ans = 0 %
Traitement des formes métastatiques
Peu d’avancées jusqu’en 2015… 1- SternberG CN et al. Cancer 1989;64:2448–2458
2- McCaffrey JA et al. J Clin Oncol 1997;15(5):1853-7
Docetaxel 2
3- Von der Maase et al. J Clin Oncol 2000;18(17):3068-77
4- SternberG CN et al. J Clin Oncol 2001;19(10):2638-46
5- VauGhn DJ et al. J Clin Oncol 2002;20(4):937-40
Gemcitabine + Cisplatine3 6- Bellmunt J et al. J Clin Oncol 2009;27(27):4454-61
MVAC
Dose-dense4
Paclitaxel 5 Vinflunine6
MVAC
standard1
1989 1997 2000 2001 2009 2015…
Rien d’excitant depuis 1989…
1- Sternberg CN et al. Cancer 1989;64:2448–2458 4- Sternberg CN et al. J Clin Oncol 2001;19(10):2638-46Traitement des formes métastatiques
les drogues actives en phase II
Monothérapie % RO
CDDP, MTX 35%
Vinblastine 25%
gemcitabine 30 %
paclitaxel, docetaxel 40%
Roth et al., J Clin Oncol 1994; 12: 2264–2270
de Wit et al., Br J Cancer 1998; 78: 1342–1345
Moore et al., J Clin Oncol 1997; 15: 3441–3Traitement des formes métastatiques
Les protocoles de références
MVAC intensifié (4-6 cycles) (J1=J15)
Methotrexate
Vinblastine
Adriamycine
Cisplatine
Neulasta ++
ORR 72 %
CR 25 %
PFS 9.5 mois
Sternberg et al., Eur J Cancer 2006; 42: 50-54Traitement des formes métastatiques
Les protocoles de références
Cisplatine-Gemcitabine (6 cycles)
ORR 50 %
CR 12 %
PFS 7.7 mois
Efficacité similaire au MVAC avec meilleure tolérance
Von der Maase et al., J Clin Oncol 2000; 17:3068-3077Traitement des formes métastatiques
Les protocoles de références
Patient unfit au cisplatine - DFG < 60 mL/min
- Insuffisance cardiaque NYHA III
- Neuropathie grade 2
- Baisse d’audition grade 2
Carboplatine – Gemcitabine (4-6 cycles)
(Gemcitabine – docetaxel)
(Carboplatine – Taxol)
Monothérapie: carboplatine, gemcitabine
Ardavanis A. 2005 Br J Cancer ;92
23 :645-50Traitement des formes métastatiques
Résumé 1ère ligne
ddMVAC MVAC Cis-Gem
ORR, % 64 50 50
PFS, m 9.5 8.1 7.7
OS, m 15.1 14.9 14
30-50% CIS-ineligible
Carbo instead of CIS :ORR=36%, OS=9.3 moisTraitement des formes métastatiques
2 ligne
ème
§ Vinflunine (Javlor®)
- Bénéfice en survie versus BSC (6.9 mois vs 4.6 mois)
- ORR = 9%
Bellmunt J, J Clin Oncol 2009; 27:4454-61.
§ Autres: paclitaxel, docetaxel
- ORR = 10%
Ardavanis A. 2005 Br J Cancer ;92 :645-50
25THE IMMUNE CHECKPOINT REVOLUTION…
Checkpoints
inhibitors
Figure 3. Emerging Hallmarks and Enabling
Characteristics
An increasing body of research suggests that two
additional hallmarks of cancer are involved in the
pathogenesis of some and perhaps all cancers.
One involves the capability to modify, or repro-
gram, cellular metabolism in order to most effec-
tively support neoplastic proliferation. The second
allows cancer cells to evade immunological
destruction, in particular by T and B lymphocytes,
macrophages, and natural killer cells. Because
neither capability is yet generalized and fully vali-
dated, they are labeled as emerging hallmarks.
Additionally, two consequential characteristics of
neoplasia facilitate acquisition of both core and
emerging hallmarks. Genomic instability and thus
mutability endow cancer cells with genetic alter-
ations that drive tumor progression. Inflammation
by innate immune cells designed to fight infections
and heal wounds can instead result in their inad-
vertent support of multiple hallmark capabilities,
thereby manifesting the now widely appreciated
tumor-promoting consequences of inflammatory
responses.
Hanahan and Weiberg, Cell 2011 The extraordinary ability of genome maintenance systems to
Yet other distinct attributes of cancer cells have been
proposed to be functionally important for the development of detect and resolve defects in the DNA ensures that rates ofInhibiteurs de checkpoints immunologiques
Antigen
PD-L1/
MHC TCR
PD-1 PD-L2
Tumour
T cell T cell
APC cell
B7-1/ CTLA-4
B7-2 TCR MHC
Antigen
CTLA-4 pathway PD-1 pathway
Anti–CTLA-4
Positionnement
Anti–PD-L1:
initial ICP: Anti–PD-1
•Ipilimumab 1ère ligne CIS-UNFIT
•Atezolizumab •Nivolumab
•Tremelimumab
2ème ligne post-platine
•Durvalumab
• Avelumab
•Pembrolizumab
Adapted from BMS.ICP chez les CIS-UNFIT
Rappel: 50% des patients
Trial n inegibility ORR, % OS, m 1y OS, % Tox G3-4, %
Chemotherapy*1 28-56 9.8 37 >40
DFGICP en 2 ème ligne post-doublet avec platine
ORR, PFS, OS, 1y OS,
Trial n
% m m %
Chemotherapy* 12 2.2-3 7 26
Pembrolizumab KEYNOTE-0451 270 21 2.1 10.3 44
Atezolizumab IMvigor 2112 467 23 2.1 11.1 46
Durvalumab Etude 11083,4 191 31 1.5 18.2 -
Nivolumab CHECKMATE 2755 270 19,6 2 8.74 NA
Avelumab JAVELIN6,7 44 18 2.7 13.7 -
* vinflunine or taxanes
1-Bellmunt et al, N EnG J Med 2017; 2. Powles et al, Lancet 2018; 3. Massard C et al, J Clin Oncol 2016; 4-Powles et al, JAMA Oncol 2017;
5- Sharma P et al, Lancet Oncol 2017; 2-; 6-Apolo AB et al, J Clin Oncol 2017; 7-Patel MR et al, Lancet Oncol 2018lizumab : la déception de la phase 3
PhIIIR: grosse déception pour l’ATEZO en 2ème ligne !
=primary endpoint
Powles et al. EAS 2017PhIIIR:Pembrolizumab
Plus de succès pour le pembrolizumab!
: essai transformé!
mOS : 10,3m
7,4m
lN=542
lRéponse objective: 21.1% vs 11.4%
AMM Européenne
ASMR IV en France
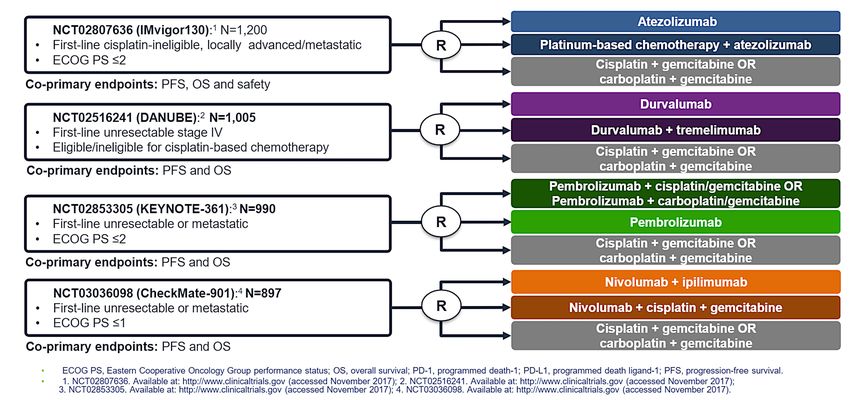
Avec prise en charge! Bellmunt et al. NEJM 2017Perspectives en 1ère ligne métastatique: COMBO
NEGATIF
NEGATIF
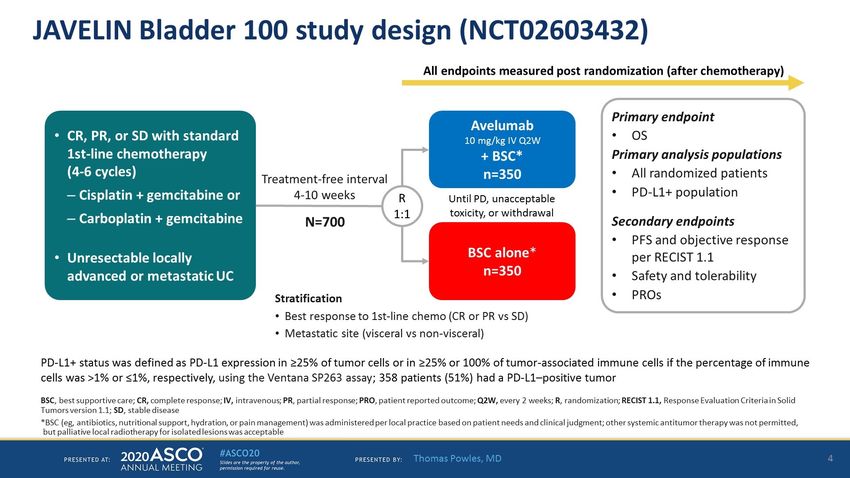
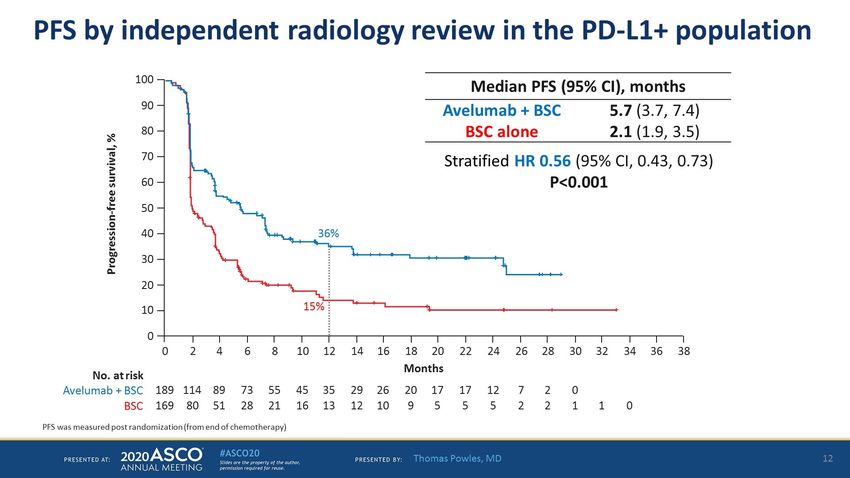
NEGATIFJAVELIN Bladder 100 study design (NCT02603432)
Presented By Thomas Powles at TBDOS
Overall
population
Primary endpoint
PD-L1+
population
Presented By Thomas Powles at TBDSubgroup analysis of OS in the overall population
Presented By Thomas Powles at TBDPFS (IRR)
Overall
population
PFS by independent radiology review in the overall population
PD-L1+
population
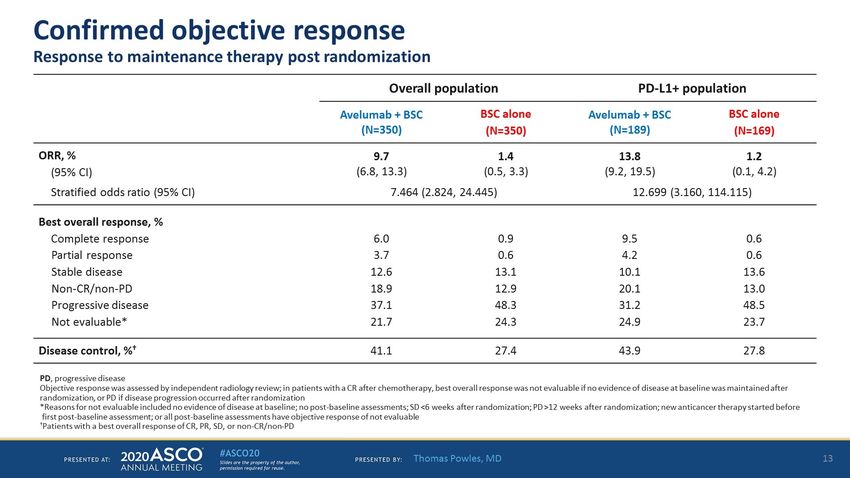
Presented By Thomas Powles at TBDConfirmed objective response
Presented By Thomas Powles at TBDImmune-related AEs
Presented By Thomas Powles at TBDThérapies ciblées dans le cancer de vessie
Non-invasive bladder cancer
Mutations ~ 70% tumors
Invasive bladder cancer Proliferation/migration/
Altérations de FGFR3 Mutations/translocation ~15% anti-apoptosis/angiogenesis
Upper tract urothelial
Mutations/translocation ~35%
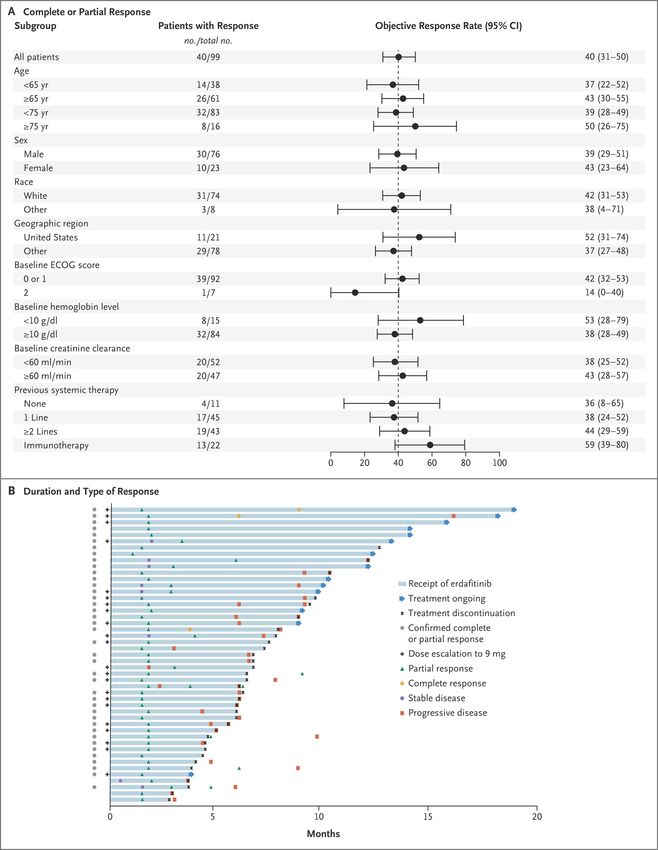
Erdafitinib (Janssen): 40% ROBahleda R, ASCO 2015
Thérapies ciblées dans le cancer de vessie Tabernero J JC0 2015
Inhibiteur de FGFR
2 months
40Overall Survival in the Intention-to-Treat Population and
Nouvelle classe:
Analysesles
in Ac
Keyconjugués
Subgroups. Exemple de l’enfortumab vedotinExemplePopulation
Overall Survival in the Intention-to-Treat de l’enfortumab
and vedotin
Nouvelle classe:
Analysesles
in Ac
Keyconjugués
Subgroups.
PFS
OS
T Powles et al. N Engl J Med 2021. DOI: 10.1056/NEJMoa2035807
Powles T. et al. NEJM 2021Perspectives carcinome urothelial • Combinaisons: • Anti-PD-1 avec anti-FGFR ou Ac conjugués • Stades plus précoces • TVIM voire TVNIM + instillations BCG
Prise en charge du cancer de vessie dans la pop. AGEE
Algorithme de traitement proposé pour le
cancer de vessie du sujet âgé
4 JO U R N A L OF GE RI A TRI C O N COL O G Y 6 (2 0 1 5) 1 –7
Table 1 – Potential management algorithm for elderly patients with muscle-invasive bladder cancer.
Patient characteristics a Treatment options
Medically operable cisplatin-eligible • Neoadjuvant cisplatin-based chemotherapy followed by radical cystectomy
• Radiation therapy with concurrent cisplatin if opts for bladder sparing
Medically operable cisplatin-ineligible • Radical cystectomy
• Radiation therapy with concurrent chemotherapy?
Medically inoperable cisplatin-eligible • Radiation therapy with concurrent cisplatin
Medically inoperable cisplatin-ineligible • Radiation therapy with concurrent chemotherapy (5-fluorouracil + mitomycin; gemcitabine, etc.)
• Radiation therapy alone
a
Components of the Comprehensive Geriatric Assessment (function, mobility, nutrition, comorbidity, cognition, mood, social support) may
further refine risk/benefit assessment.
Identique à l’algorithme chezhaslebeensujet
adoptedplus
the absence of randomized trials, due to a favorable tolerability jeune
as a commonly utilized first-line treatment
profile [22]. standard. Age alone should generally not be used to exclude
Little data is available regarding the use of chemoradiation patients with metastatic bladder cancer from cisplatin-based
with curative intent specifically for elderly patients with chemotherapy. In an analysis of the impact of age on outcomes
bladder cancer. A recent review of this topic by Turgeon et al. of patients with metastatic bladder cancer receiving cisplatin-
Matthew Galsky, J of Geria Oncol 2015
identified only one prospective study though additional retro- based chemotherapy in a series of phase II and III clinical trials,Given the large proportion of cisplatin-ineligible patients
La question cruciale en néoadjuvant et en 1ère
with metastatic bladder cancer, particularly elderly patients,
several phase II trials and a single phase III trial have explored
ligne métastatique
der Cancer in
chemotherapy regimens specifically for this patient popula-
tion. The EORTC conducted a randomized phase II/III trial of
gemcitabine plus carboplatin (GCa) versus methotrexate,
Eligibilité au cisplatine ?
vinblastine, plus carboplatin (M-CAVI) in cisplatin-ineligible
e 1980s, represented a
tastatic bladder cancer Table 2 – Consensus definition for cisplatin-ineligibility in
ved in up to 50% of patients with metastatic bladder cancer.
20% of patients, and At least one of the following
–10% of patients [24].
• ECOG PS of 2 (KPS of 60–70)
herapy regimens have
• Creatinine clearance >> âge
Status; chronologique
CTCAE, Common Terminology
ever, gemcitabine plus Criteria for Adverse Events;
MaisNYHA, New York Heart Association.
lien évident
vere side effects and
Matthew Galsky, J of Geria Oncol 2015to acknowledge that the value proposition of current treat-
However, whether the safety an
ments is in direct relation to their associated balance of
particularly immune checkpoin
Algorithme de traitement de 1 ligne ère
potential benefits and harms. As more efficacious and less
toxic treatments emerge, artificial classifications such as
aging on the immune system, a
métastatique du cancer de vessie du sujet âgé patients requires further invest
In the meantime, developing
risk assessment of the benefits a
Table 3 – Potential management algorithm for elderly integrating these tools into stan
patients with metastatic bladder cancer. cating this information in a ma
Patient characteristics a Treatment options medical decisions, is critical to
medicine in the elderly.
PS 0–1 and creatinine clearance ≥60 • Gemcitabine plus cisplatin
Prudence+++
• Dose-dense MVAC b
En néoadjuvant surtout
• Clinical trial
PS 2 or creatinine clearanceQuid des ICP chez le sujet âgé
452 O. Alkharabsheh et al. / Journal of Geriatric Oncology 9 (2018) 451–458
Pas d’essais dédiés ICP chez
les sujets âgés
Age médian essais phases III
ICP vs CHIMIO en L2
= entre 66 et 73 ans
Fig. 1.
surveillance,” the innate immune system “checks” tumorigenesis. The and prevalence of cancer among older adults, adu
balance between activated and inhibited T cells is critical in maintaining years of age account for b10% of patients enrolled i
an active immune response against foreign antigens and immune toler- Institute (NCI) cooperative group trials. This lack
Daste A. et al. EJC 2017 Alkharabsheh O. et al. Journal
ance for host antigens. Immunotherapy seeks to activate the host immune Ofattributed
been Geriatric Oncology
to different factors,2018
including adv
system against tumor cells that escape normal immunosurveillance. adequate social support, poor performance statusLa sénescence impacterait négativement la
réponse immunitaire anti-tumorale
158 A. Daste et al. / European Journal of Cancer 82 (2017) 155e166
Théorique!!!
Daste A. et al. EJC 2017Efficacité ICP chez le SA: données de sous- e
Données d'efficacité et de toxicité des immunothérapies anti cancéreuses chez le sujet âgé – 5 journée de
groupes toutes tumeurs
pharmacologie des anti-tumoraux
Compte-rendu de congrès
TABLEAU I
Principales études de validation des inhibiteurs de points de contrôle immunitaire et recueil des résultats des analyses de sous-groupe
concernant les populations âgées
Cancer primitif Molécule étudiée Population Nombre de patients Efficacité (versus
population générale)
Cancer de la tête et du cou [5] Nivolumab phase 3 Sous-groupe 65–75 ans 95 HR 0,93 (0,64)
IC95 [0,56–1,64] Bénéfice
Cancer rénal à cellules claires [4] Nivolumab phase 3 Sous-groupe 65–75 ans 119 HR 0,64 (0,78) supérieur à
IC95 [0,45–0,91] la pop.
Cancer rénal à cellules claires [4] Nivolumab phase 3 Sous-groupe > 75 ans 34 HR 1,23 (0,78)
IC95 [0,66–2,31]
générale
Carcinome urothélial [14] Pembrolizumab phase 3 Sous-groupe > 65 ans 312 HR 0,76 (0,75)
IC95 [0,56–1,02]
Carcinome urothélial [15] Atézolizumab phase 2 Sous-groupe > 80 ans 25 Objective response
28 % (23 %)
[12–49]
Cancer bronchique non à petites Nivolumab phase 3 Sous-groupe 65–75 ans 200 HR 0,63 (0,81)
cellules, non épidermoïde [16] IC95 [0,45–0,89]
Cancer bronchique non à petites Nivolumab phase 3 Sous-groupe > 75 ans 43 HR 0,90 (0,81)
cellules, non épidermoïde [16] IC95 [0,43–1,87]
Cancer bronchique non à petites Pembrolizumab phase 3 Sous-groupe > 65 ans 164 HR 0,45 (0,61)
cellules PDL1 positifs [17] IC95 [0,29–0,70]
Gaultier de Saint Basile. et al. Bull. Can. 2018Toxicités compilées nivolumab chez le SA
H. Gaultier De Saint Basile, C. Poisson, J. Arrondeau, P. Boudou-Rouquette, F. Goldwasser, E. Tartour, et al.
Compte-rendu de congrès
TABLEAU II
Tolérance du nivolumab chez les personnes âgées [23]
Effet secondaire Patients < 65 ans Patients ! 65 ans Patients ! 70 ans
(n = 616) (n = 414) (n = 212)
n (%) n (%) n (%)
Grade 1–2 584 (94,8) 394 (95,2) 202 (95,3)
Grade 3 –5 360 (58,4) 259 (62,6) 152 (71,1)
Conduisant à l'interruption du traitement 89 (14,4) 71 (17,1) 42 (19,8)
Nécessitant la mise en place d'un traitement immuno modulateur
Total 256 (41,5) 196 (47,3) 110 (51,9)
Diarrhée/Colite 15 (2,4) 17 (4,1) 11 (5,2)
Pneumopathie 23 (3,7) 8 (1,9) 5 (2,4)
Hépatite 8 (1,3) 3 (0,7) 1 (0,5)
Néphrite/Dysfonction rénale 6 (1,0) 8 (1,9) 7 (3,3)
Rash 47 (7,6) 34 (8,2) 22 (10,4)
>70 ans: plus de grade 3-5, plus d’arrêt de tt, plus de tox nécessitant un traitement immunomodulateur
Gaultier de Saint Basile. et al. Bull. Can. 2018.091), in RCC patients in 52.9% vs. 41.5% (p = .424) and in UC patients
in 67.0% vs. 40.0% (p = .118) (Fig. 1B). After exclusion of patients under-
going combination ICI therapy, there was still no difference regarding
DCR between patients ≥75 years vs.0.55–1.33, P = 0.49) when directly compared w
3.4. Multivariable Analysis ≥G3 toxicity. In the sensitivity analysis using b
and cancer type were eliminated from the mod
AgeDonnées Enfortumab vedotin SA
EV-201: Non-Comparative, Pivotal Phase 2 Trial
Presented By Arjun Balar at 2021 Genitourinary Cancers SymposiumDonnées Enfortumab vedotin SA
EV-201 Cohort 2: Key Demographics and Disease Characteristics
Presented By Arjun Balar at 2021 Genitourinary Cancers SymposiumDonnées Enfortumab vedotin SA
EV-201 Cohort 2: Responses by Subgroup per BICR
PFS 5,8 mois
OS 14,7 mois Presented By Arjun Balar at 2021 Genitourinary Cancers SymposiumDonnées Enfortumab vedotin SA
EV-201 Cohort 2: Treatment-Related Adverse Events
Presented By Arjun Balar at 2021 Genitourinary Cancers SymposiumA retenir
Messages
• Majorité des cancers de vessie >65 ans
• Souvent population poly-vasculaire poly-morbide
• Ne pas sous-traiter les patients FIT sur la base de l’âge chrono
• Précaution >75 ans et poly-chimio
• sous-groupes des études prospectives: Cut-off à 65 ans inadapté, patients ultra-fits
• CISPLAT > CARBO à contrebalancer avec nécessité hyperhydrat vs tox hémato
• Dogmes (- efficace – toxique) sur inhibiteurs de checkpoints chez SA sont
faux
• aussi efficaces que chez le jeune
• toxicités identiques voire plus fréquentesNous avons besoin de vous, gériatres pour identifier les fragilités des SA
Merci
QUESTIONS?
yann.vano@aphp.frVous pouvez aussi lire

















































