Cardiopathies,acquises - Dr Daniela Laux Cardiopédiatre associée - UE3C -Paris Médecin hospitalier temps partiel - Arcothova
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous

Cardiopathies,acquises
Dr Daniela Laux
Cardiopédiatre associée – UE3C –Paris
Médecin hospitalier temps partiel
Centre Chirurgical Marie Lannelongue
Le Plessis Robinson
Plan,du,cours, • Maladie(de(Kawasaki( • Endocardite(infec4euse( • Myocardite(
Maladie(de(Kawasaki(
Kawasaki – Les points clés • Maladie(décrite(en(1967(–(seulement(50(ans(de(recul(!( • Vascularite, systémique, qui( touche( essen4ellement( les, artères, de, moyen, calibre, avec( un( tropisme( élec4f( pour( les, artères,coronaires,(gravité(de(la(maladie)(( • Les(complica4ons(coronaires(surviennent(dans(15,à,25,%,des( cas(chez(les(enfants(non(traités( • L'administra4on( précoce( d'immunoglobulines( humaines( par( voie( intraveineuse( a( transformé( le( pronos4c( en, diminuant, par,5,le(risque(d'anévrisme(coronaire( • Risque, de, mortalité, 0,015, %, (Japon),( surtout( entre( le( 15N45eme( jour( (thrombocytose( concomiQante( avec( la( vascularite)(
Epidémiologie( • Première,cause,de,cardiopathie,acquise,de,l'enfant,dans,les, pays,développés, ( • Tous,les,âges,pédiatriques,(80,%,des,cas,avant,5,ans)( • Les(pa4ents(de(moins,de,1,an,ou(de,plus,de,8,ans,sont(rares( mais(ont(un(risque(plus(élevé(d'anévrisme(coronaire( • Formes,de,l'adulte:,première(fois(décrite(en(1977( • symptômes(majeurs(décrits(iden4ques( ( • Kawasaki,aOeint,chaque,année:, – 265/100.00(enfants(
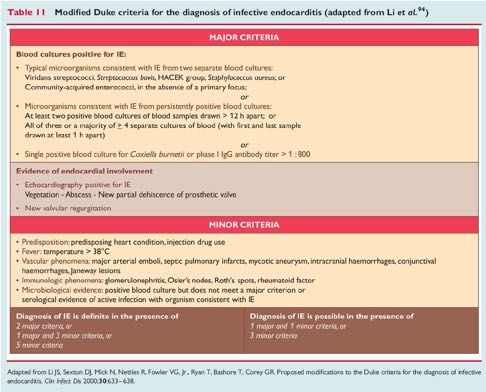
CaractérisTques,cliniques:,critères,majeurs,
La,fièvre,de,plus,de,5,jours,et,au,moins,4,critères,suivants,
(
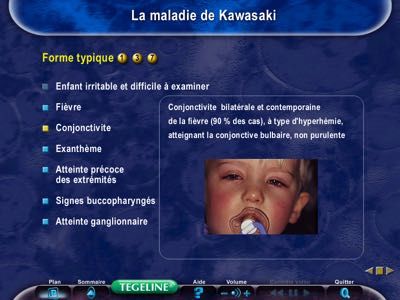
N(La(conjoncTvite(bulbaire(non(purulente(
N(L’aOeinte,muqueuse(:(la(pharyngite,(la(chéilite,(la(langue(framboisée,(la(stoma4te(
N(L'exanthème,polymorphe,du,tronc,
N(L'aOeinte,des,extrémités(:(un(érythème(des(paumes(des(mains(et/ou(des(plantes(
des(pieds,(l'œdème(palmoNplantaire,(la(desquama4on(palmoNplantaire(secondaire((
N(L'aOeinte,unilatérale,des,ganglions,cervicaux,(de(plus(de((
(1.5(cm(de(diamètre((
(
Critères majeurs définis par l'American Heart Association Committee On Rheumatic Fever, Endocarditis, and Kawasaki Disease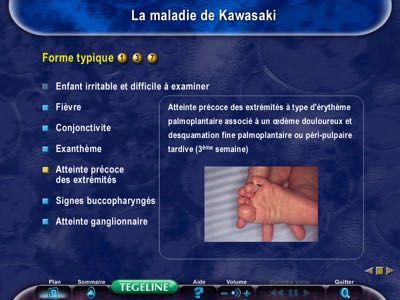
Faciès(typique(d’un(enfant(avec(( une(maladie(de(Kawasaki(
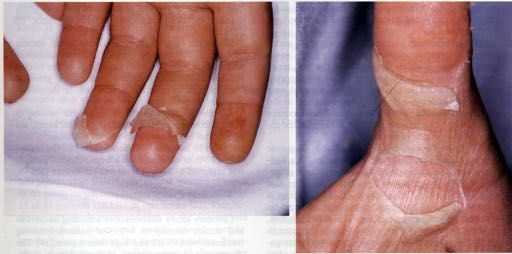
AQeinte(muqueuse(et(desquama4on(palmoNplantaire(
Formes(rares:(forme(psoriasiforme/(BCGite(
AQeinte(cardiovasculaire(
• Pas,d’aOeinte,coronaire,dans,75%,des,cas,!,
• Anomalie,ECG,ou,échocardiographique:,
– DilataTon,des,artères,coronaires,(20%),
– Anévrismes(coronaires(
– Infarctus(
– Myocardite(avec(possible(insuffisance(ventriculaire(gauche(
sévère(
– Péricardite,(épanchement(péricardique(
– Fuites(valvulaires(par(inflamma4on(des(valves(cardiaques(et(
par4culièrement(la(valve(mitrale((1(%)(
– Troubles(conduc4fs(et(troubles(du(rythme(par(inflamma4on(
du(4ssu(de(conduc4on(Les(anévrismes(coronaires(
• (
Entre,le,10 ,et,le,25 ,jour,d'évoluTon,
ème ème
• 5(%(lorsque(le(traitement(est(fait(précocement((
(=(,2,,2,5,,10,ou,>,8,mm,
(
Newburger JACC 2016Formes(atypiques(
Tableau,clinique,dominé,par,un,symptôme,inhabituel:(
(
«(convulsions,(œdème(pulmonaire,(diarrhée(sanglante,(ascite,(
obstruc4on(des(voies(aériennes(supérieures,(épiglonte,(
adénopathies(cervicales(compressives(ou(hémolyse(et(
défaillance(mul4Nviscérale,(syndrome(néphro4que,(
hyponatrémie….(»(
(
Formes,de,l'adulte,
• (Troubles(diges4fs,(aQeinte(hépa4que,(signes(
(ar4culaires(et(encéphalites(sont(plus(fréquent(Les(formes(incomplètes(
,
Pa4ents(ayant(eu(une(fièvre(depuis(au,moins,5,jours,et((
au(moins,deux,critères,cliniques,de,Kawasaki,(sans(cause(évidente,((
et(des(critères(biologiques(en(faveur(d'une(inflamma4on(systémique(
(
• Différent,de,la,«,forme,atypique,»,
,
• Manque(un(ou(plusieurs,des,cinq,critères,diagnos4ques(majeurs(
(,
• Plus,fréquentes,chez,les,enfants,les,plus,jeunes,,à,risque,,
,,,,,d'anomalies,coronaires(
((
Diagramme(décisionnel(proposé(par(l'American(Academy((
of(Paediatrics(pour(aider(à(la(prescrip4on(d’IgG(dans(les(formes(
incomplètes((
Newburger JW et al., Circulation. 2004Critères,cliniques,et,biologiques,supplémentaires, Cardiovasculaires,:(dilata4on(des(artères(coronaires,(anévrismes(coronaires,( infarctus,(myocardite(avec(possible(insuffisance(cardiaque(conges4ve,(péricardite,( épanchement(péricardique,(fuites(valvulaires,(troubles(conduc4fs(et(troubles(du( rythme,(anévrismes(des(vaisseaux(du(cou,(des(artères(rénales,(spléniques,( hépa4ques,(pancréa4ques,(génitales,(gangrènes(distales(et(pseudoNRaynaud( ( DigesTfs,:,diarrhées,(vomissements,(douleurs(abdominales,(hydrocholécyste,( dysfonc4on(hépa4que( ( Respiratoires(:(toux(et(rhinorrhée(( ( Neuroaméningés(:(troubles(de(la(conscience(avec(irritabilité,(apathie,(état(grognon,( hypoacousie( ( ArTculaires,:(arthrite,(arthralgies( Autres,:(uvéite,(érythème(au(niveau(de(la(cicatrice(de(BCG,(desquama4on(de(l’aine( ( Albumine(
secondaire en « doigt de gant »
Atteinte unilatérale des ganglions cervicaux, de plus de 1,5 cm de diamètre, ferme
Formes incomplètes
upplémentaires
Fièvre de plus de 5 jours et 2 ou 3 critères cliniques
e, péricardite, état de choc, ou
ronaire, anévrismes extra- Fièvre de plus de 7 jours sans cause retrouvée (enfants ≤ 6 mois+++)
(vaisseaux du cou, artères
s, pancréatiques, génitales),
du culot aortique Faire un bilan biologique
s, vomissements, douleurs
e, dysfonction hépatique,
te/méatite, hydrocèle
CRP < 30 mg/l et VS < 40 mm/h CRP ≥ 30 mg/l et/ou VS ≥ 40 mm/h
ribronchique et interstitiel,
monaires
conscience avec irritabilité
aralysie faciale, hypoacousie Réexaminer et contrôler le bilan Au moins 3 critères biologiques ou plus :
ies (hyperleucocytose du biologique si la fièvre persiste
novial) Anémie pour l’âge
eau de la cicatrice de BCG, Échocardiographie en cas de Plaquettes ≥ 450 000/mm3
Non
hlegmon rétropharyngé desquamation en doigt de gant Albumine ≤ 30 g/l
typique ALAT augmentées
Globules blancs ≥ 15 000/mm3
ECBU ≥ 10 globules blancs/champ
stics différentiels Oui ou
ntérovirus, EBV, rougeole Traiter Échocardiographie positive
ine
se staphylococcique
hoc toxique Échocardiographie positive
actérienne
x médicaments Z-score IVA ou CD ≥ 2,5
vens-Johnson Ou anévrisme coronaire (Z-score ≥ 2,5)
juvénile Ou plus de 3 critères :
rose - dysfonction ventriculaire gauche
- fuite mitrale
- épanchement péricardique
oronaire élevé si score ≥ 5) - Z-score IVA ou CD compris entre 2 et 2,5
Bajolle et al. 2018 EMC
(1 point) Description coronaire
s jours de fièvre (2 points)Evolu4on(naturelle( ( 1°)(La(phase(aiguë((J0NJ10)(:(aOeinte,cardiaque,rare, ( 2°)(La(phase(subaiguë((J10NJ20)(:(diagnosTc,de,complicaTon, coronaire, ( 3°)(La(phase(de(convalescence((J20NJ70)(:(constataTon,d’anévrysmes, et,de,sténoses,cicatricielles,en(cas(de(complica4on(coronaire(à(la( deuxième(phase(
Exemples(d’aQeinte(coronaires(
Dilata4on(anévrysmale(des(artères(coronaires(
Aorte IVA =6.9 mm
Thrombus
Aorte dans l’IVA
(A)(IVA=interventriculaire(antérieure(
(B)(thrombus(dans(l’IVA(Dysfonc4on(ventriculaire(gauche(sévère(en(
échographie(
Etat de choc dans 7% des cas de maladie de Kawasaki
VG
dilaté
VG
dilatéDilata4on(anévrysmale(des(artères(
coronaires(au(scanner(
CD =4.7 mm
Aorte
IVA =6.9 mmDilata4on(anévrysmale(de(l’IVA(en(
chapelet(au(scanner(
Aorte
Aorte
Chapelet anévrysmal
Chapelet anévrysmalAnévrysme(coronaire(avec(sténose(
coronaire(au(cathétérisme(cardiaque(
Sténose Anévrysmes et sténoses
coronaire multiples des coronairesAQeinte(diffuse(des(axes(vasculaires(
A B
Foie
Dilatation
fusiforme
Aorte
(A)(épaississement(pariétal(hyperéchogène(de(l’aorte,(de(l’artère(mésentérique(supérieure(et(du(tronc(
coeliaque(en(échographie((
(B)(dilata4on(fusiforme(de(l’artère(mésentérique(supérieure,(du(tronc(caeliaque(au(scanner(Le(traitement(de(1ère(inten4on(
Immunoglobulines,intraveineuses:(
• 2g/kg(en(8(à(12(heures,(à(posologie(progressive(
(
En,associaTon(à(de(l’acide,acétylsalicylique,(AAS),:,
• à( fortes( doses( pour( ses( effets( an4Ninflammatoires( et( an4N
thrombo4ques((30a50,mg/kg/j,en,4,fois),à(la(phase(aiguë((
• puis( à( dose, anTaaggrégante, plaqueOaire, rapidement( 48N72( h(
après(l’apyrexie((3N5(mg/kg/jour)(
De Graeff et al 2019, Newburger 2016CE NTRAL ILL USTRATIO N Management of Kawasaki Disease
Diagnosis of Kawasaki disease according to American Heart Association criteria*
Anti-inflammatory therapy with intravenous immunoglobulin (IVIG) and ASA (acetylsalicylic acid or aspirin).
Echocardiogram to assess coronary arteries and determine Z score.
Defervescence with no coronary dilation (Z scoreKawasaki Disease APRIL 12, 2016:1738–49
Recommanda4ons(américaines(
TABLE 1 Principles in Acute Management of KD
1. The goal of therapy is to reduce systemic and tissue-level inflammation as rapidly as possible. For this reason, patients should be treated as soon as
diagnosis can be confidently established.
2. All patients within the first 10 days of fever onset should be treated with IVIG. Patients diagnosed after 10 days should receive IVIG treatment if
they are still febrile, have markedly elevated inflammatory parameters, or have coronary artery dilation.
3. Recrudescent fever at least 36 h after the end of IVIG infusion without other explanation is a marker for persistent inflammation and should prompt
immediate and aggressive anti-inflammatory therapy
a. Antibody-mediated hemolysis has become common in KD patients who have received IVIG retreatment and have type A or B blood; rescue
therapies other than IVIG (e.g., infliximab, corticosteroids) should be considered.
4. Patients with coronary artery dilation (z-score >2.0) should be followed with a repeat echocardiogram at least twice a week until dimensions
stabilize; additional anti-inflammatory therapy should be considered.
5. Patients with giant aneurysms should have frequent echocardiograms in the first 3 months of illness for thrombus surveillance, even after
dimensions stabilize.
6. Infants under 6 months of age are at extremely high risk of aneurysm formation, even with timely therapy. They require echocardiograms every few
days until dimensions have stabilized.
7. Patients with giant CAA (z-score $10) are at highest risk for thrombosis during the first 3 months after fever onset
a. Systemic anticoagulation together with an antiplatelet agent should be administered until coronary dimensions improve.
b. Low-molecular-weight heparin is easier to regulate than warfarin in infants, as well as in patients of any age, during the acute phase of illness or
until hsCRP normalizes.
CAA ¼ coronary artery aneurysm; hsCRP ¼ high-sensitivity C-reactive protein; IVIG ¼ intravenous immunoglobulin; KD ¼ Kawasaki disease.
Newburger JACC 2016
The progression of aneurysm formation in some Children With Kawasaki Disease and Coronary ArterySurveillance(à(court(terme((
Pour,les,paTents,sans,complicaTon,coronaire:,
• 1(echo(entre(1N2(semaines(et(1(echo(entre(4N6(semaines((Classe(1)(
Pour,les,paTents,avec,Z,score,coronaire,>,2,0,à,la,phase,aigue:,
• 2(echos(par(semaines(jusqu’à(l’arret(de(la(progression(
(
Pour,les,paTents,avec,anévrismes,géants:,
• 2(échos(par(semaine(tant(que(les(lésions(progressent(
• 1(écho/sem(pdt(45(jours(puis(
• 1(écho/mois(pendant(3(mois((Casse(IIA)(
Newburger JACC 2016An4agréga4on(et(an4coagula4on( PaTents,sans,aOeinte,coronaire:, • Aspirine(pendant(6(semaines((Cl(1)( ( PaTents,avec,aOeinte,coronaire,d’aggravaTon,rapide:, • Hospitalisa4on(pour(mise(sous(heparine((An4Xa(0,5N1)( • Arret(si(stabilisa4on;(Z(score(
Que(faire(en(cas(de(persistance(de(la(fièvre(
après(une(première(cure(d’IgIV?(
• Résistants:,15(à(20(%(des(cas(
• Associée(à(un(risque(plus(élevé(d'aQeinte(coronaire(
• Deuxième(dose(d’IVG((
• associée(à(un(bolus(de(cor4coides((20N30(mg/kg/jour(IV(
methylprednisolone)(
• Discuter:,prednisolone(p.o.(plus(prolongé(2N3(semaines(
• Alterna4ve:(infliximab(
• En(cas(d’échec:(ciclosporine(
Newburger(JW(et(al.,(Circula4on.(2004(
Egami&K&et&al.,&J&Pediatr&2006&Qui sont les patients à haut risque?
Comment identifier les résistants ?
• Score issu de la littérature de patients japonais!!
Score d’Egami (2006) Score de Kobayashi (2006) Score de Sano (2007)
Age ≤ 6 mois (2 points) Age ≤ 12 mois (1 point) Bilirubine totale ≥ 0.9mg/dL (1
point)
≤ 4 jours de fièvre (1 point) Traitement dans les 4 premiers CRP ≥ 7mg/dL (1 point)
jours de fièvre (2 points)
Plaquettes ≤ 300.109/L (1 Plaquettes ≤ 300.109/L (1 ASAT ≥ 200 U/L (1 point)
point) point)
CRP ≥ 8mg/dL(1 point) CRP ≥ 10mg/dL (1 point)
ALAT > 100 U/L (1 point) ASAT ≥ 100 U/L (1 point)
≥ 80% neutrophiles (2 points)
Na+ ≤ 133 mmol/L (2 points)
Haut risque si ≥ 3 points Haut risque si ≥ 5 points Haut risque si ≥ 2 points
Scores issus de la population japonaise, spécifique mais non sensible
Shohai O et al., Pediatrics 2011; Egami K et al., J Pediatr 2006 ; Chen S, et al. JAMA 2016; Mc Crindle Circ 20172. Treatment of KD should include IVIG at a dose of 2 g/kg as a single infusion. 1A A
3. In non-Japanese patients, the Kobayashi criteria may indicate risk of IVIG resistance if ‘positive’ (score 2A C
Original article
54) but may not reliably exclude IVIG resistance if ‘negative’ (scoreQuelle,est,l’histoire,naturelle,des,complicaTons,
coronaires,de,la,MK?,
• Dispari4on(complète(dans(plus(de(50%(des(cas(même(
en(cas(d’anévrysme((sauf(géant)(dans(les(2(ans(
• Occlusion(coronaire;(sténoses(localisées(ou(mul4ples(
parfois(très(tardives…(
• Gravité(des(lésions(tardives(car(mul4ples(et(chirurgie(
difficile(Anévrysme(géants((1%)( • Mortalité(et(morbidité(+++( • Survie(à(30(ans:(88N90%( • Cardiac(event(free(à(30(ans(:(30%( • 26%(infarctus(myocardique( Adapted with permission from Newburger et al. (99). • Risque(accru(dans(les(2(ans(après(le(diagnos4c(( • 50%(de(bypass(coronaire(à(30(ans(
Surveillance à long terme
19-1800 ! Maladie de Kawasaki
Immunoglobulines IV à 2 g/kg sur 12 h
Aspirine à dose anti-inflammatoire 60 mg/kg/j jusqu’à disparition de la fièvre
Puis relais par AAP 3–5 mg/kg/j
75 % 20 % 4% 1%
Anévrisme géant
Coronaires Petit anévrisme Anévrisme moyen
Dilatation Z-score ≥ 10 ou ≥ 8 mm
normales 2,5 ≤ Z-score < 5 5 ≤ Z-score < 10
2 ≤ Z-score < 2,5 AAP à vie
Z-score < 2 AAP 1 an AAP à vie
AAP 6 semaines AVK pour INR 2-3
AAP 6 semaines Cs à M3, M6, M12 Cs à M3, M6, M12
Cs à 6 semaines Cs à M1, M2, M3, M6, M9, M12
Cs à 6 semaines Coroscanner à 1 an Coroscanner à 1 an
Coronarographie à 1 an
Même Si Normali- Si
Normali- Si
Arrêt Normali- Si si persistance sation persistance
sation persistance
aspirine sation persistance normalisation Aspirine Aspirine Aspirine à vie
Arrêt Maintien
Clôture Arrêt Maintien Aspirine à vie à vie à vie Maintien AVK
aspirine aspirine
du aspirine aspirine ± double ± double ± double ± double AAP
Clôture du Cs/2–5
dossier Cs/1–3 ans Cs/an AAP AAP AAP ± BB
dossier ans
Cs/an Cs/an Cs/an Cs/6 mois
Prévention des FDRCV pour tous !
Figure 2. Arbre décisionnel. Prise en charge proposée par le centre de référence Malformations Cardiaques Congénitales Complexes (M3C) Necker. IV : par
voie intraveineuse ; AAP : aspirine à dose antiagrégante plaquettaire ; Cs : consultation ; AVK : antivitamine K ; INR : international normalized ratio ; FDRCV :
facteurs de risques cardiovasculaires.
! Formes incomplètes lines est le plus souvent excellente. La recommandation est une
perfusion lente de 12 heures pour éviter tout effet secondaire
Lorsqu’on a une forme incomplète de maladie de Kawasaki (flush, hypertension, malaise,Bajolle et al.etc.).
hypotension, 2018 Les EMC
immuno-
(fièvre d’au moins cinq jours associée à deux ou trois critères cli- globulines humaines sont des médicaments dérivés du sang. Àiffness testing should minimize risks of anesthesia and
North ionizing radiation. Children too young to exercise
in pe-
, reas- Devenir(à(long(terme(
of late T A B L E 2 Principles in the Long-Term Management of Patients With KD
nifesta-
1. On the basis of available data, patients with no demonstrated coronary artery
always- dilation by echocardiogram with excellent visualization of all arterial segments
ears of during the first weeks of illness appear to have normal cardiovascular status in
early adulthood.
2. Remodeling (so-called regression) of aneurysms, especially if moderate or large,
to normal internal lumen diameter is often accompanied by luminal
myofibroblastic proliferation and abnormal vascular reactivity.
3. Patients with persistent CAA are at lifelong risk of progressive coronary artery
stenosis or occlusion and worsening ischemia.
ifelong 4. Patients with CAA documented at any stage require lifelong cardiovascular
are to surveillance tailored to disease severity and age.
5. Testing should minimize exposure to ionizing radiation whenever possible.
cardial
6. Sedentary life-style should be avoided.
ble 2).
7. Women with coronary aneurysms can carry pregnancy successfully, but should
de the have reproductive counseling.
testing 8. Monitoring and counseling regarding traditional CV risk factors is appropriate to
reduce the likelihood of later atherosclerosis.
d upon Newburger JACC 2016
athero-Endocardite(
Endocardite(infec4euse(
(
Def:(Infec4on/inflamma4on(de(l’endocarde(=(valves(cardiaques(
Dg:,Echographie(transNthoracique(voire(ETO(
(N(EI(des(VAV:(sur(le(versant(auriculaire(
(N(EI(des(valves(sigmoïdes:(sur(le(versant(ventriculaire(
• Hémocultures:(au(moins(3!!!!!!!!!!!((au(mieux(6)(
• Pas(d’ATB(à(l’aveugle(
• Scanner(total(body((cérébral,(thoracique(et(abdominal)(
• Examen(ophtalmologique,(bandeleQe(urinaire(
• Recherche(porte(d’entrée:(examen(dentaire,(ORL,(cutané,(diges4f,(
urinaire,(KTC…(
(Endocardite:(germes(
Endocardite:(Traitement(médical(
Endocardite:(Traitement(chirurgical(
Endocardite:(préven4on(
Endocardite:(préven4on(
Endocardite:(préven4on(
- Bonne hygiène dentaire quotidienne
- Consultation dentaire tous les 6 mois
Indispensable pour diminuer le risque d’endocarditePOPULATION CONGENITALE(N(ENFANTS(
34 279 enfants avec CC suivis de 0 à 18 ans
Incidence annualisée = 4.1 / 10 000 pt-année
Rushani et al. Circulation
2013POPULATION CONGENITALE(N(ADULTES(
Registre CONCOR (14 224 patients>18 ans)
Incidence EI : 1.33/1000 pt-years
Prothèse valvulaire: HR=3.57(2.58–5.36)
Kuijpers et al. Eur Heart Jour
2017INCIDENCES(COMPARATIVES(
Valve Melody : 0.8 – 3% pt-année
Valves/conduits pulmonaire chir : 0.5 - 3% pt-année
TAVI: 0.67 – 2.1% pt-année
Valves Ao/mitrale chir : 0.3 – 1.2% pt-année
Dispositifs electroniques implantables : 1.9/1000,deviceaannée,,
Patients avec CC: 0.4 – 1.33 / 1000 pt-année
Miranda et al. Eur Heart Jour 2016
Wang et al. JAMA 2007
Rushani et al. Circulation 2013
Population générale : 30 -100/ million pt-année Habib et al. Eur Heart Jour 2015
Dayer et al. Lancet 2015COMPARER(CE(QUI(EST(COMPARABLE(
50VALVES(PERCUTANÉES(VS(CHIRURGICALES(
p=0.1
3
134 chir et 208 percut (33 Sapien) 195 chir et 93 percut (0 Sapien) 631 chir et 107 percut (0 Sapien)
Incidence IE: 0.5 vs 1.5 %pt/années Incidence IE: 1.2 vs 3.9 %pt/années Incidence IE: 0.8 vs 2.7 vs 3% %pt/années
Lluri et al. CCI 2017 Malekzadeh-Milani et al. JTCS 2014 Van(Dijck(et(al.(Heart(2014(SUBSTRAT(VALVULAIRE(
Author Year n Substrate EI EI Annualized Median
Cumulative Incidence Follow-up
incidence (% pt-year) (years)
Albanesi, 2014 12/106 Contegra 11.3 7.6
Malekzadeh 2014 5/190 Homografts 2.6 1.2 2
Contegra
Ramanan 2015 6/115 Freestyle 5.4 - 4.3
Mery 2016 23/586 Homograft 4 - 7
Contegra
Porcine valve
Ugaki 2016 21/298 Contegra 7 - 3.4
Homograft
Tous les dispositifs valvulaires sont susceptibles d’être le
siège d’une EI
Avec une incidence variable mais significative Albanesi(et(al.(EJCTS(2014(
Ramanan et al. Ann Thorac Surg
2015
Ugaki et al. Ann Thorac Surg 2016(
Mery(et(al.(JTCS(2016(SUBSTRAT(VALVULAIRE( • EI plus fréquente chez les patients avec VJB • Quelle que soit la techniqued’implantation (i.e. Contegra et Melody) • Comparés aux homogreffes RR=8.7 and 9.7 pour Melody et Contegra MalekzadehNMilani(et(al.(JTCS(2014( (Mery et(al.(JTCS(2016( Van(Dijck(et(al.(Heart(2014( Ugaki(et(al.(Ann Thorac Surg 2015
SUBSTRAT(VALVULAIRE(
Méta-analyse sur IE chez les patients avec RVP chirurgical ou
percutané
7063 patients
Incidence cumulative globale = 2.5%
VJB vs autres substituts : 5.4% vs 1.2%; p < 0.0001
Sharma et al. JACC Int. 2017VALVE(SAPIEN(
JACC: CARDIOVASCULAR INTERVENTIONS VOL. 10, NO. 5, 2017
ª 2017 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/$36.00
PUBLISHED BY ELSEVIER http://dx.doi.org/10.1016/j.jcin.2016.12.012
512 Hascoet et al. JACC: CARDIOVASCULAR INTERVENTIONS VOL. 10, NO. 5, 2017
Endocarditis After PPVI: Melody Versus Sapien Infective Endocarditis Risk After MARCH 13, 2017:510–7
JACC: CARDIOVASCULAR INTERVENTIONS VOL. 10, NO. 5, 2017
Percutaneous Pulmonary Hascoet et al.Valve513
MARCH 13, 2017:510–7 Endocarditis After PPVI: Melody Versus Sapien
Implantation With the Melody
and from phone calls to the patients and to their
TABLE 1 Patient Demographics, Procedural Data, and Post-Procedural Outcomes and Sapien Valves
cardiologists and general practitioners. For cases of
PPVI With PPVI With IE, every effort was made to obtain
Sebastieninformation
Hascoet, MD,a Luciaon
Mauri, MD,a Caroline Claude, MD,a Emmanuelle Fournier, MD,a Julie Lourtet, MD,b
Melody Valve Sapien Valve Standardized c c
the Duke criteria, clinical and microbiological
Jean-Yves Riou, MD, details,
Philippe Brenot, MD, Jérôme Petit, MDa
(n ¼ 32) (n ¼ 47) Difference
Age (yrs)
(73 of19.979;(15.8–28.9)
92.4%). A single stent was sufficient
26.3 (18.9–39.9) 0.58*
in all
medical and surgical strategies, and outcome.
TABLE 1 Continued
Weight (kg) Melody56.5
group
! 13.5patients, 65.8
whereas
! 17.6 in the Sapien
0.59* group 4
ABSTRACT
STATISTICAL ANALYSIS. Statistical analyses were
Male (%) 53.1 66.0 0.26 PPVI With PPVI With
patients required 2 to 4 stents. Pre-stenting was not
performed using Stata 11.2 software (StataCorp,
OBJECTIVES Col- the risk of infective endocarditis (IE) after percutaneous pulmonary valve
This study compared
Genetic syndrome (%) 18.8 10.6 -0.23 Melody Valve Sapien Valve Standardized
implantation (PPVI) with the Sapien and Melody valves.
History of severe infectiousperformed
9.4in 6 patients with
8.5 valve-in-valve
-0.03 implan-
lege Station, Texas). Continuous data(n ¼were
32) described (n ¼ 47) Difference
disease (%)
History of endocarditis (%)
tation. Balloon
6.3
post-dilation
2.1
was performed
-0.20
in 19 as
of meanInfective
! SD if normally distributed
endocarditis during
and asThemedian
BACKGROUND
25.0
incidence of IE after PPVI is estimated at 3% per year with the Melody valve. The Sapien valve is a
0.0 -0.80*
(interquartile range [IQR]) more recently Categorical
otherwise. marketed valve used for PPVI.
Pacemaker/defibrillator (%)79 patients
6.3 (24.1%) and was
10.6 more common
0.16 in the follow-up (%)
variables were described as number (%).
METHODS Bivariate
We retrospectively included consecutive patients who underwent PPVI at a single center between 2008 and
Congenital heart diseases (%) Pulmonary valve replacement 25.0 4.3 -0.59*
Melody group (46.9% vs. 6.5%, respectively). Pro-
analyses with calculation of standardized differences
2016. IE was diagnosed using the modified DUKE criteria.
Conotruncal malformation 81.3 68.1 during follow-up (%)
Ross procedure cedure duration,
9.4 21.3 time, and irradiation
fluoroscopy were performed to compare variables
Percutaneous
between the
3.1 PPVI was performed in 79 patients
RESULTS 2.1 (Melody valve, 40.5%;-0.06
Sapien valve, 59.5%). Median age was 24.9 years
two valve types and between patients (range 18.1 towith
34.6). IEversus
occurred in 8 patients (10.1%) at a median of 1.8 years (minimum: 1.0; maximum: 5.6) after
TGA
were higher
3.1
in the Sapien 0.0
valve group. Surgical 21.9
surgery. 2.1
Causative organisms were methicillin-sensitive Staphylococcus-0.63*
aureus (n ¼ 3), Staphylococcus epidermidis (n ¼ 1),
PA-IVS/PVS 3.1 4.3 without IE during follow-up.
DORV Severe 3.1
procedural complications
6.4 occurred in 2 pa- Kaplan-Meier
Death during curves
follow-up of
(%) the cumulative
3.1
Streptococcus mitis (n ¼ 1),
IE inci-
Aerococcus 2.1
viridans (n ¼ 1), -0.06
Corynebacterium striatum (n ¼ 1), and Haemophilus influenzae
(n ¼ 1). All 8 cases occurred after Melody PPVI (25.0% vs. 0.0%). The incidence of IE was 5.7% (95% confidence interval:
RVOT (%) tients (2.5%). One patient died of massive hemo-
dence were plotted using the date of PPVI
2.9% asperthe
to 11.4%) entry
person-year after Melody PPVI. The Kaplan-Meier cumulative incidence of IE with Melody PPVI was
Native RVOT 3.1 25.5 Values are time
median since
[interquartile range]
thorax due to perforation date
of a distal pulmonary and the PPVI as orthe
%. Standardized
24.0%time difference
scale.
(95% confidence computed
The12.2%
interval: as the
to 43.9%) afterdifference
4 years and in means
30.1% (95%orconfidence interval: 15.8% to 52.5%)
Bioprosthesis 9.4 23.4 proportions divided by the SE. *Significant after
imbalance.
6 years, compared with 0.0% with the Sapien PPVI after 4 years (p < 0.04 by log-rank test). There was a trend
right censor was the date of IE, valve replacement,
Homograft branch during
25.0 Sapien valve
31.9PPVI over a Lunderquist toward a higher incidence of IE in the first 20 patients with Melody PPVI (who received prophylactic antibiotics during the
DORV ¼ double-outlet right ventricle; PA-IVS ¼ pulmonary atresia with intact ventricular septum; PPVI ¼
Conduits 62.5 19.2
heart transplantation, death, or follow-up
percutaneous pulmonary valve implantation; procedure only) andcomple-
PVS ¼ pulmonary in patients who had percutaneous interventions, dental care, or noncardiac surgery after PPVI.
valve stenosis; RVOT ¼ right ventricle outflow
RVOT lesion (%)
guidewire. In the other patient, who had a mechanical
tion. Differences in incidence were evaluated
tract; TGA ¼ transposition of the great arteries. using
CONCLUSIONS IE after PPVI may be less common with the Sapien compared with the Melody valve.
Stenosis aortic valve,
84.4 a large femoral
50.0 hematoma developed
the log-rank test. The Kaplan-Meier method
(J Am was
Coll Cardiol Intv also © 2017 by the American College of Cardiology Foundation.
2017;10:510–7)
Regurgitation 0.0 35.7 used to assess the cumulative incidences of pulmo-
Mixed 15.6 14.3 nary valve replacement and of death, with the date of
Pre-stenting (%)
1-stage
Hascoet PPVIJACC
et al. (%) Int. 2017
No. of stents (%)
0
90.6
87.5
93.6
87.2
0.11
0.01
FIGURE 1 Kaplan-Meier Cumulative Incidences of Death and Pulmonary
9.4 6.4
Valve
PPVI as the entry date and the time since
time scale and with the right censor set
Replacement and Kaplan-Meier
outflow
geryasforthe
Cumulative
tract
valve replacement, heart transplantation, death, (RVOT).
PPVI as the
P ercutaneous pulmonary valve implantation
(PPVI) has emerged as an alternative to sur-
certification in 2006 and Food and Drug Administra-
tion approval in 2010 for PPVI. The Sapien valve
date ofthe right ventricular (Edwards SAPIEN pulmonic transcatheter heart valve,
reconstructing
Incidences
PPVI was firstofdescribed
or Infective
in Endocarditis
Edwards Lifesciences, Irvine, California) was used
2000 (1) and since then many studies have supported initially for transcatheter aortic valve replacement
1 90.6 85.1 end of follow-up. Differences itsinefficacy
incidence were
(2–13) The Melody valve (Medtronic Inc., and subsequently licensed for PPVI (Europe, 2010;VALVE(SAPIEN( Hascoet et al. JACC Int. 2017
VALVE(SAPIEN( Edwards SAPIEN XT Transcatheter Heart Valve with the NovaFlex1Deliv- ery System. Vol. 2016. https://www.accessdata.fda. gov/cdrh_docs/pdf13/ p130009s037d.pdf.
(PREVENTION(N(EDUCATION((
PROCEDURE
PRE-IMPLANTATION
Salle hybride
Patient et famille
Optimisation gradient
Depistage foyer infectieux résiduel
Bilan dentaire et ORL Antibioprophylaxie per +/-
post procédure
POST-IMPLANTATION
Education patient, parents, médecin traitant, dentiste
Anti-aggrégants au long cours
Antibioprophylaxie à vieFACTEURS(AGGRAVANTS(
Portes d’entrée évitables
Manque observance
Déficiences mentales
Education - Prophylaxie EI
Bauer et al. Int Jour Cardio
2017
Buber et al. Circ Intrv 2013Myocardites,aiguës,
,Généralités(
• Série(autopsique:(iden4fica4on(d’une(myocardite(dans(8,6%(à(
12%(en(cas(de(mort(subite(
• Evolu4on(vers(la(CMD(possible(et(non(excep4onnelle(
• Physiopathologie(
Kindermann, JACC 2012Kociol et al
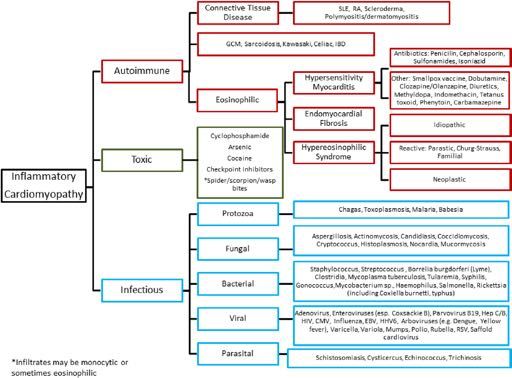
E4ologies(des(myocardites( Recognition and Management of Fulminant Myocarditis
CLINICAL STATEMENTS
AND GUIDELINES
Downloaded from http
Kociol et al Figure 5. Causes of lymphocytic myocarditis. Recognition and Management of Fulminant Myocarditis
Diagram demonstrating the primary causes and associated subcategories of lymphocytic myocarditis. GCM indicates giant cell myocarditis; IBD, inflammatory
bowel disease; RA, rheumatoid arthritis; and SLE, systemic lupus erythematosus. Reprinted from Trachtenberg and Hare.99 Copyright © 2017, American Heart
Association, Inc.Diagnos4c(posi4f(
(
• Clinique,évocatrice:,,
– douleur(thoracique,(fièvre((30%),(tachycardie((58%),(
dyspnée((68%)(
– Choc(cardiogénique((Forme(fulminante,(5N10/1(mill(
d’habitants/an)(
– Mort(subite((TDR(ou(TDC)(
• Biologie:, , , ,Troponine,(BNP(ou(NNproBNP(
• ECG:, , , ,infarctus(du(myocarde(
• Echocardiographie:, ,dysfonc4on(modérée(à(sévère(
• IRM(et/ou(biopsie,endomyocardique,(BEM)(
• Sérologies,virales( ( (peu(u4les(en(pra4que(clinique(
(Critères(de(Dallas(historiques((1986)(
Infiltration lymphocytaire
Signe de nécrose non ischémique
Magnani JW et al. Circulation 2006 Cooper LT et al. Circulation 2007Problèmes(des(critères(de(Dallas(
• Myocardite(avec(aQeinte(hétérogène(du(myocarde(N
>(Biopsies(mul4ples(>(5(
• Geste,invasif:,mortalité(0,5%,(complica4ons(5%:(
perfora4on(cardiaque,(hémopéricarde,(tamponnade(
• Geste(plus(risqué(chez(le(nourrisson(
• Variabilité(d’interpréta4on(même(entre(experts(
1916 Cooper et al.
Endomyocardial Biopsy in Cardiovascular Disease
Table 1. Risks Associated With Endomyocardial Biopsy in failure, includi
• «(Goldstandard(»(mais(discutée(++(
546 Procedures potentially hear
Overall 33 complications (6%)
Sheath insertion 15 (2.7%) Analysis o
12 (2.0%) arterial puncture during local anesthesia
2 (0.4%) vasovagal reaction EMB Proces
1 (0.2%) prolonged venous oozing after sheath removal
Samples should
ventricular sept
Biopsy procedure 18 (3.3%)
range from 5 to
6 (1.1%) arrhythmia
and each samp
5 (1.0%) conduction abnormalities must be handle
4 (0.7%) possible perforation (pain) ferred from the
3 (0.5%) definite perforation (pericardial fluid) formalin) by u
2 of 3 patients with definite perforation died (21,22). The f
Data derived from Deckers et al (20). prevent contrac
The clinical
(0.03%). Deckers et al (20) prospectively recorded compli- samples are rem
cations from 546 consecutive right heart biopsy procedures in least 4 to 5 sIndication d’une BEM
Kociol et al Recognition and Management of Fulminant Myocarditis
CLINICAL STATEMENTS
AND GUIDELINES
Figure 3. Indications for endomyocardial
biopsy (EMB).
Guideline-based algorithm for whether EMB
is indicated. COR indicates Class of Recom-
mendation; LOE, Level of Evidence; and MRI,
magnetic resonance imaging. *Usually a dilated
cardiomyopathy. Fulminant myocarditis may
have normal end-diastolic diameter with mildly
thickened walls. Exclude ischemic, hemodynam-
ic (valvular, hypertensive), metabolic, and toxic
causes of cardiomyopathy as indicated clinically.
Reprinted from Bozkurt et al.3 Copyright ©
2016, American Heart Association, Inc.
despite normalization of cardiac enzymes and biomark-
EMB, CORONARY ANGIOGRAPHY, ers.78 EMB can be considered the primary diagnostic
AND INVASIVE
Circ 2020
HEMODYNAMICS strategy76,79 when magnetic resonance imaging is not
Kociol et al Recognition and Management of Fulminant Myocarditis
In the setting of cardiogenic shock, right-sided heart possible (eg, shock, presence of metal devices) if expe-
catheterization and coronary angiography are essential to rienced operators and cardiac pathologists are readily
guide management strategies. The decision to perform available. According to guidelines, however, indications
SLake(Louise(Criteria:((IRM((
Trois(séquences(IRM(contribu4ves:(
• 1.(Œdème(en(T2(
• 2.(rehaussement(précoce(du(myocarde(
• 3.(rehaussement(tardif(du(myocarde(
• Diagnos4c(posi4f(si(>(2(critères(:(
– Hypersignal(T2(
– Ra4o(Signal(myocarde(/(muscle(périph(augmenté(après(injec4on(de(
Gadolinium(
– Hypersignal(en(rehaussement(tardif(
• Refaire(IRM(à(1N2(semaines(si:(
– 0(critère(mais(symptômes(trop(récents,(forte(suspicion(clinique(
– 1(seul(critère(présent(
Friedrich MG et al. JACC 2009Traitement(en(fonc4on(de(la(forme(clinique(
,
• Myocardite,segmentaire,focale:,Repos(
• Myocardite,aiguë,diffuse,chez,l’enfant(
– Surveillance(+/N(assistance(circulatoire((HNF)(
– Traitement(d’aQaque:((
• Immunomodulateurs,(immunosuppresseurs,(An4N
inflammatoire,(immunoadsorp4on(
• Myocardite,fulminante,
– PEC(du(choc(cardiogénique(
– (Traitement(spécifique(en(fonc4on(du(type(histologique)(
• Myocardite,chronique,acTve(
– Discuter(immunosupresseurs(Traitement( ce(qui(est(admis(…(
Traitement(de(l’insuffisance(cardiaque(
• Selon,les,guidelines,
• Selon,la,classe,foncTonnelle,NYHA,
– IEC(
– Diuré4ques(
– BNbloquant(
– ARA(II(
(
• Formes,sévères:,Prise,en,charge,en,réanimaTon,
– Traitement,«,agressif,»,
– Assistance,circulatoire,(>(60(à(80(%(survivants(et(
récupéra4on(ad(integrum(possible)(
– Drogues,Inotropes,posiTves,et,héparine!,
Kindermann, et al., JACC 2012
Amabile et al. Heart 2006Traitement(de(la(myocardite(fulminante(
Kociol et al Recognition and Management of Fulminant Myocarditis
CLINICAL STATEMENTS
AND GUIDELINES
Downloaded from h
Circ 2020
Figure 4. General approach to initial stabilization of patients in cardiogenic shock.
ACS indicates acute coronary syndrome; CABG, coronary artery bypass grafting procedure; ECMO, extracorporeal membrane oxygenation; IABP, intra-aortic bal-
loon pump; MCS, mechanical circulatory support; PCI, percutaneous coronary intervention; and VAD, ventricular assist device. Reprinted from van Diepen et al.86Traitement(
ce(qui(est(discuté(…(
(
Immunoglobulines(
An4(inflammatoires(
An4viraux(
Immunosuppresseurs(
(Immunosuppressive Treatment for
Myocarditis in the Pediatric
He et al. Immunosuppressive Treatment for Myocarditis in the Pediatric
Population: A Meta-Analysis
TABLE 1 | Characteristics of studies included in the meta-analysis.
Study N Age Study IMSA IMSA dosage, time of Follow-up Observed Inclusion criteria
methodology IMSA start variables
Bing He* , Xiaoou Li and Dan Li
Camargo et al. 50 5 months−15 PNCT P, CyA P & A: 2.5 mg/kg/d, 1 8.4±1.2 months LVEDD, LVEF, Active myocarditis based
Department (9)of Pediatrics, Renmin
years Hospital of Wuhan University, Wuhan,
week; 2.0 mg/kg/d, 3 China PWP, CI, HR on EMB findings
weeks; 1.5 mg/kg/d, 4
weeks
Cy: 1.5 mg/kg/d, 1 week;
The use of immunosuppressants in the treatment of myocarditis in children remains 1.0 mg/kg/d, 7 weeks;
0.5 mg/kg/d, 1 week
controversial.
Aziz et al. (6)
The
68
aim of RCTthis meta-analysis
3.7 ± 2.9 P 2 mg/kg/d, 1 month
is to 15.1±9.2
summarize LVEDD, LVESD,
the current empirical
Duration of symptoms
evidence for immunosuppressive years treatment for myocarditis months LVEF in the forstudies of
Department arePediatrics,
included inRenmin
the present study,ofofWuhan
Hospital which University,
only one Wuhan,
treatmentChina
in the short term may significantly improve LVEF,
is an RCT study; this might result in a lack of statistical reduce LVEDD, and reduce the risk of death and heart transplant
power to detect a significant difference in the treatment effect. in pediatric population with myocarditis. Although this meta-
Moreover, we were able to ascertain publication bias in only analysis reported beneficial outcomes with immunosuppressive
The four
use ofstudies,
immunosuppressants
which means only four of sixin thedata treatment
therapy, theof myocarditis in children remains
Immunosuppressive Treatment for
of six
controversial. The aimDueofto this
findings of this meta-analysis.
studies’
could be merged, which may have impacted the analysis of the
meta-analysis
the included studies’ lack
results have to be interpreted cautiously because
one RCT was included in this meta-analysis; more large-scale
is to summarize the current empirical
RCTs are required in the future.
only
Myocarditis in the Pediatric
evidence for follow-up
of long-term immunosuppressive treatment
(only two studies had median follow- for myocarditis in the pediatric population.
up > 1 year), their inferences can only be applied to short- AUTHOR CONTRIBUTIONS
We term
searched PubMed, MEDLINE, and Embase for articles to identify studies analyzing
Population: A Meta-Analysis
outcomes. In this meta-analysis,
didn’t report
we couldn’t provide
data of viral genome and histologic type, because the included
the studies
efficiency of these
immunosuppressive
data even if this information
exact
treatment
was
BH is responsible for the provision of the overall idea and writing
articles. in the data
XL collects pediatric
and modifiespopulation. Pooled
the paper. DL is responsible
important to the therapy and prognosis. RCTs in the future for statistical analysis.
Bing estimates wereLigenerated
and Dan using fixed- or random-effect models. Heterogeneity within
• Groupe d’enfants avec immunosuppresseurs
He* , Xiaoou Li
studies
Department was assessed
of Pediatrics, Renmin using Hospital Cochran’s
of Wuhan University,Q and I2Wuhan, statistics. ChinaFunnel plots and Begg’s rank
The were
amélioration significative:
REFERENCES
correlation method were constructed to evaluate
use also
of immunosuppressants in potential
1. Sagar S, Liu PP, Cooper LT Jr. Myocarditis. Lancet. (2012) 379:738–7.
the treatment
publication
detection bias.
of viruses in myocardial
ofheterogeneity.
myocarditis After
Sensitivity
11. Camargo PR, Okay TS, Yamamoto L, et al. Myocarditis in children and
tissue: implications analyses
for immunosuppressive
in children
therapy. Int J Cardiol. (2011) 14:148:204–8. doi: 10.1016/j.ijcard.2009.
conducted to evaluate the
doi: 10.1016/s0140-6736(11)60648-x sources
11.002 of a detailedremains
– 2. Fraction
controversial.Dancea AB.
screening ofThe aim
Myocarditis
159Paediatrics
the paediatrician. d’éjection
studies, of
in infants this
and children:
six
and Child separate
Health. (2001) VG
meta-analysis
A review for
studies were
6:543–5.
is to
12. Richardson summarize
P, McKenna
identified,
J, et al. Report
W, Bristow M, Maisch
of the 1995 worldwithhealth 181
the current
B, Mautner
patients
B, O’Connell empirical
organization/international in the
society
evidence for immunosuppressive treatment for
doi: 10.1093/pch/6.8.543 myocarditis
and federation in on
of cardiology task force the pediatric
the definition population.
and classification of
immunosuppressive treatment group, and 199 incardiomyopathies.
the conventional Circulation. (1996) treatment group. The
– Diamètre télédiastolique VG
3. Burch M. Immunosuppressive treatment in pediatric myocarditis Scanty 93:841–2. doi: 10.1161/01.CIR.93.5.841
We searched Evidence. PubMed,
Heart. (2000) 90:1103–4.MEDLINE, and
doi: 10.1136/hrt.2004.034082 Embase 13. Higgins for JPT, articles to
Green S (eds). Cochrane identify studies
Handbook for Systematic Reviewsanalyzing
immunosuppressive
4. Liu PP, Mason JW. Advances intreatment
the efficiency of immunosuppressive
(2001) 104:1076–82.
the understanding ofgroup
doi: 10.1161/hc3401.095198
myocarditis.showed
Circulation. a
treatment significant
of Interventions Version
Collaborationin (2011).
theimprovement
5.1.0 [updated March
pediatric
Available
in left
2011]. ventricular
The Cochrane
population. Pooled
online at: http://www.cochrane-handbook.
Edited by:
Giuseppe Limongelli, estimates– Diminution
ejectionetwere
fraction of knowledge on décès
(LVEF)
generated
al. Current state
[mean
using
aetiology, et
difference
5. Caforio AL, Pankuweit S, Arbustini E, Basso C, Gimeno-Blanes J, Felix SB,
fixed-
diagnosis, transplantation
management,
therapy of myocarditis: a position statement of the European Society of
or 1.10; org
95%
and random-effect
CI:
14. Wells GA, Shea B, O’Connell
0.41, models. 1.79] and significantly within
D, Peterson Heterogeneity
J, Welch V, Losos M,
et2al. The Newcastle–Ottawa Scale (NOS) for Assessing the Quality of
iversity of Naples, Italy decreased
studies wasCardiology left
assessed ventricular
Working Group on using end-diastolic
Myocardial Cochran’s dimension
and Pericardial Diseases. I (LVEDD)
QEurand Nonrandomised
statistics. [mean
Studies Funnel difference
in Meta-Analyses. plots
Ottawa, andHospital
ON:−0.77
Ottawa mm, rank
Begg’s
Heart J. (2013) 34:2636–48. doi: 10.1093/eurheartj/eht210 Research Institute (2019). Available online at: http://www.ohri.ca/programs/
Reviewed by: correlation
95%6. CI: method
Aziz KU,−1.35 towere
Patel N, Sadullah T,−0.20
constructed
Tasneem H, mm]Thawerani when
toviralevaluate
compared
H, Talpur S. Acute to the publication
conventional
clinical_epidemiology/oxford.asp
bias. Sensitivity
treatment group. analyses
Marco Merlo, wereFurthermore,
also myocarditis:
conducted the20:509–15.
Cardiol Young. (2010) riskto doi:evaluate the potential
role of immunosuppression: a prospective randomised study.
of10.1017/S1047951110000594
death and sources of heterogeneity. Afterwas
15. Okada R, Kawai S, Kasyuya H. Non-specific myocarditis: a statistical and
heart transplant clinicopathologicalin study
conventional
of autopsy cases. Jpn treatment
Circ J. (1989) 53:40–8.
a detailed
niversity of Trieste, Italy
Meena Nathan, • MAIS: 1 seule étude RCT, effectifs faibles,
screening of 159 studies, six separate studies were identified, with 181 patients in the
7. Drucker
significantly
NA,
Gamma-globulin
immunosuppressive
Colan
higher
SD, Lewis
treatmentthan
AB, Beiser AS, Wessel
in thein the
of acute myocarditis
treatment
Circulation. (1994) 89:252–7.
DL, Takahashi
immunosuppressive
M, et
pediatric population.
group, and 199in in
doi: 10.1161/01.CIR.89.1.252
al. doi: 10.1253/jcj.53.40
16. Waller BF,
2007the
treatment
Catellier MJ, Clark group
conventional
consecutive
MA, Hawley DA, [relative
forensic autopsies. Clin treatment
risk
Pless JE. Cardiac (RR):
pathology
Cardiol. (1992) 15:760–5. group. The
follow-up court
4.74; 95% CI: 2.69, 8.35]. No significant heterogeneity across the studies was observed.
rvard Medical School, 8. Bhatt GC, Sankar J, Kushwaha KP. Use of intravenous immunoglobulin doi: 10.1002/clc.4960151014
immunosuppressive
compared with standard treatment group
therapy is associated with showed
improved 17. a significant
Klugman D, Berger JT, Sableimprovement
CA, He J, Khandelwal SG, Slonim inAD.left ventricular
Pediatric
EditedUnited
by: States
Therefraction
ejection was no evidence
complicated by (LVEF) myocarditis. [mean
of publication
clinical outcomes in children with acute encephalitis syndrome
Pediatr Cardiol. difference bias whenCardiol.
(2012) 33:1370–6. 1.10;
assessed
95% bydoi:Begg’s
CI:
(2010) 31:222–8. 0.41, test.
patients hospitalized with myocarditis: a multi-institutional analysis. Pediatr
1.79] and significantly
10.1007/s00246-009-9589-9
e Limongelli,
*Correspondence: doi: 10.1007/s00246-012-0350-4 18. Arola A, Pikkarainen E, Sipilä JO, Pykäri J, Rautava P, Kytö V. Occurrence and
Naples, Italy decreased
Bing He
leftPR,ventricular
Conclusions:
9. Camargo Snitcowsky R, da Luz end-diastolic
There may be a possible Assoc. dimension
PL, Mazzieri R, Higuchi ML, Rati M, features of(LVEDD)
benefit, [mean
a nationwidedifference
in the short term, to the
childhood myocarditis: −0.77
study in Finland. J Am Heart mm,
viewed by:
hb0701@sina.com
Marco Merlo,
et al. Favorable effects of immunosuppressive therapy in children with dilated
95% CI: −1.35
addition
to −0.20 mm]
of immunosuppressive therapy in the
when compared
cardiomyopathy and active myocarditis. Pediatr Cardiol. (1995) 16:61–8.
doi: 10.1007/BF00796819
to the conventional
management of myocarditis in the
19. Aretz HT, Billingham ME, Immunosuppressive Treatm
(2017) 6:e005306. doi: 10.1161/JAHA.116.005306
treatment
Edwards WD, Factor SM, Fallon JT, Fenoglio
JJ, et al. Myocarditis: a histopathologic definition and classification. Am J
group.
Furthermore, the risk of death and heart transplant in conventional treatment was
Trieste, Italy
enaSpecialty
Nathan,section:
10. Gagliardi MG, Bevilacqua M, Bassano C, Leonardi B, Boldrini R, Camassei
pediatric
significantly
population.
FD, ethigher
al. Long term than However,
follow up ofinchildren
further prospective
thewithimmunosuppressive
myocarditis treated by
Cardiovasc Pathol. (1986) 1:3–14.
investigation
treatment
20. Cooper LT, Baughman is AM,
KL, Feldman warranted
group
Myocarditis in the Pediatric
to
[relative
Frustaci A, Jessup validate
M, Kuhl U, et al.risk (RR):
ticle
ical was
nited
4.74;this
submitted to
School,
States
95%
immunosuppression and of children with dilated cardiomyopathy. Heart.
finding.
CI:
(2004) 2.69,
90:1167–71. 8.35]. No significant heterogeneity
doi: 10.1136/hrt.2003.026641 disease: a scientificacross
statement fromthe Population: A Meta-Analysi
The role of endomyocardial biopsy in the management of cardiovascular
studies
the American wastheobserved.
Heart Association,
Pediatric Cardiology,
There was no evidence of publication bias when assessed by Begg’s test.
apondence:
section of the journal Keywords: immunosuppressive treatment, myocarditis, pediatric, cardiac function, meta-analysis Bing He*, Xiaoou Li and Dan Li
Bing in
Frontiers He Conclusions:
Pediatrics There may
be a possible benefit, in the
Frontiers in Pediatrics | www.frontiersin.org
8 short
November 2019 | Volume 7 |term,
Article 430 to the
Department of Pediatrics, Renmin Hospital of Wuhan University, Wuhan, China
1@sina.com
addition of immunosuppressive therapy in the management of myocarditis in the
ceived: 22 May 2019Traitement(de(la(myocardite(fulminante(
Kociol et al Recognition and Management of Fulminant Myocarditis
Table 7. Major Myocarditis Subtypes Resulting in a Fulminant Presentation
CLINICAL STATEMENTS
Subtype H&E Findings Clinical Manifestations Treatment
AND GUIDELINES
Fulminant lymphocytic Extensive dense lymphocytic infiltrate Acute heart failure rapidly leading Treatment is primarily supportive; circulatory
myocarditis with associated myonecrosis. May have to cardiogenic shock, conduction support as needed to prevent MOSF. Some
occasional isolated multinucleated giant abnormalities, or ventricular evidence that in the absence of cardiotropic
cells or eosinophils. arrhythmias/SCD. Chest pain. viral genome by PCR, steroids may be helpful
GCM Extensive mixed inflammatory infiltrate Acute heart failure caused by systolic Treatments consists of multimodality therapy
characterized by the presence of several dysfunction, myocardial restriction, and should be implemented after a tissue
multinucleated giant cells (usually or both. Conduction abnormalities, diagnosis has been confirmed. Usual therapy
present after 1–2 wk), eosinophils, including CHB and EMD; ventricular includes a combination of a high-dose
monocytes, and macrophages in the arrhythmias, including sustained VT/VF steroids, a calcineurin inhibitor (such as
absence of noncaseating granulomas. and SCD. Tends to comigrate with other cyclosporine), and an antimetabolite such
Edema and extensive myonecrosis often autoimmune diseases. as azathioprine. Cytolytic therapy (purified
present. rabbit-derived polyclonal IgG directed at
human thymocytes) used for suppression of
life-threatening GCM has been reported.
Acute NEM Extensive inflammatory infiltration of Acute heart failure/cardiogenic Identify potential precipitant, especially if a
the myocardium with mononuclear cells shock. May present with a restrictive drug hypersensitivity (Table 5). High-dose
and eosinophils. Associated myonecrosis cardiomyopathy. Prothrombotic steroids. Anticoagulation. Often presents
or fibrosis. On EM, may see eosinophil intracardiac state. Peripheral with ST-segment elevations and chest
degranulation and deposition of major eosinophilia may or may not be pain mimicking an ST-segment–elevation
basic protein. present. Recent viral infection or new myocardial infarction. Rapid angiography,
medication. EMB with subsequent circulatory support,
and initiation of high-dose intravenous
corticosteroids can be lifesaving.
ICI myocarditis Newly identified lymphocytic myocarditis Acute heart failure, cardiogenic shock, Treatment includes immediate cessation
resulting from the introduction of and atrial fibrillation developing of therapy, high-dose corticosteroids (1 g
novel chemotherapeutic agents that soon after ICI therapy is started and solumedrol intravenously daily for 3 d and
unleash inhibited antitumor T cells, generally more severe with combination then 2 mg/kg prednisone daily to start,
which also may infiltrate and attack ICI therapy. Typically occurs early in followed by a slow wean) and initiation of
the myocardium. Histopathology treatment and has a fulminant course. an angiotensin receptor blocker or sacubitril/
consistent with lymphocytic infiltrate valsartan. May initially need MCS.
and myocardial necrosis.
CHB indicates complete heart block; EM, electron microscopy; EMB, endomyocardial biopsy; EMD, electromechanical dissociation; GCM, giant cell myocarditis;
Circ 2020
Downloaded
H&E, hematoxylin and eosin; ICI, immune checkpoint inhibitor; IgG, immunoglobulin G; MCS, mechanical circulatory support; MOSF, multiorgan system failure;
NEM, necrotizing eosinophilic myocarditis; PCR, polymerase chain reaction; SCD, sudden cardiac death; and VT/VF, ventricular tachyarrhythmia/ventricular fibrillation.Vous pouvez aussi lire