Infection urinaire sur sonde : du Progress ! - Institut Central Frank Bally - HPCi
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous
21.05.2019
Frank Bally
Institut Central
Service des maladies infectieuses
Mai 2019
Infection urinaire sur sonde :
du Progress !
Infection sur sonde vésicale (SV)
13% des infections nosocomiales (soins intensifs (SI): 23%)
70% des infections urinaires nosocomiales (SI: 95%)
1 infection = 4 jours d’hospitalisation en plus
EMS:
Avec SV: 9 infections urinaires / 1000 jours
Sans SV: 3 infections urinaires / 1000 jours
50% des résidents EMS avec SV vont avoir une infection
Montoya A. et al. Aging health. 2011; 7(6): 889–899.
Shuman EK et al. Infect Dis Clin North Am. 2018 Dec;32(4): 885–97.
Kunin CM, et al. Am J Epidemiol. 1992 Feb 1;135(3):291–301.
1
21.05.2019
Cathéter et bactériurie
Cathéter urinaire > 1 mois
Culture d’urines 1x/semaine
20 patients
98% de cultures positives (≥10^5 germes/mL)
78% flore polymicrobienne
en moyenne entre 2 et 3 agents isolés
Warren JW, et al. J Infect Dis. 1982 Dec;146(6):719–23.
Durée de bactériurie
Cathéter urinaire: colonisation ≈ 100% après 30 jours
• Gram-pos (sauf enterococcus): 75% < 1 semaine
• E.coli, Proteus et Pseudomonas: en moyenne 4 à 6 semaines
• Providencia stuartii: max. 36 semaines
Warren JW, et al. J Infect Dis. 1982 Dec;146(6):719–23.
2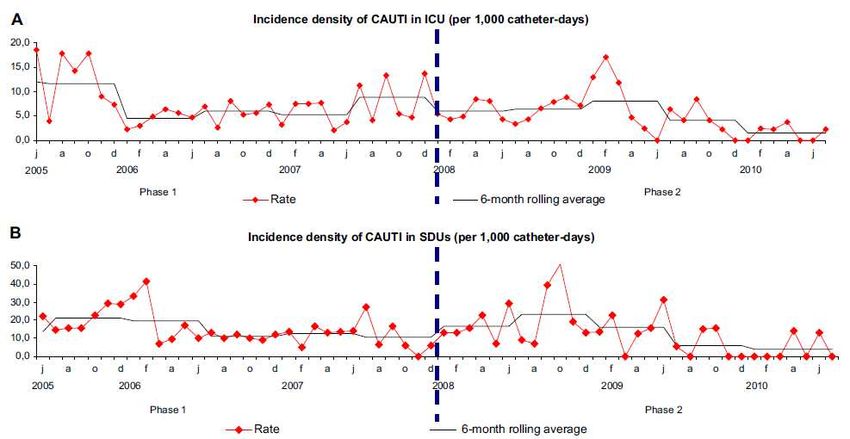
21.05.2019
Prévalence de point d’infections nosocomiales
tout type d’infection site chirurgical ou corps étranger
Point Prevalence Survey 2017 of healthcare-associated infections and
antimicrobial use in Swiss acute care hospitals. swissnoso; 2018.
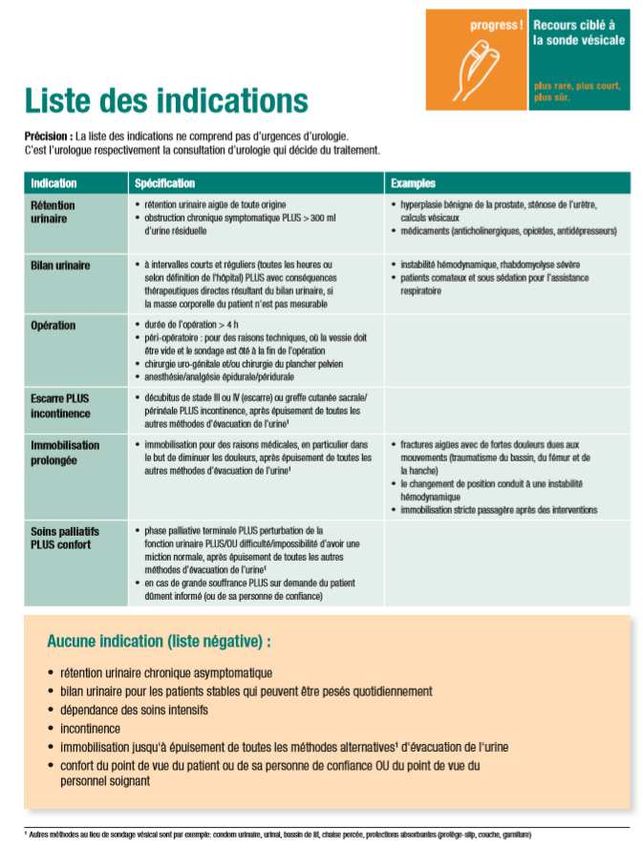
Mesures proposées pour réduire les infections sur cathéter
Réduction de l’utilisation
• Indication restrictive
• Ablation rapide
• Programme incontinence
Mesures spécifiques
• Pose stérile
• Système clos
• Eviter le reflux dans la vessie
• Cathéter fixé
• Manipulation aseptique
Précautions standard
• Hygiène des mains
3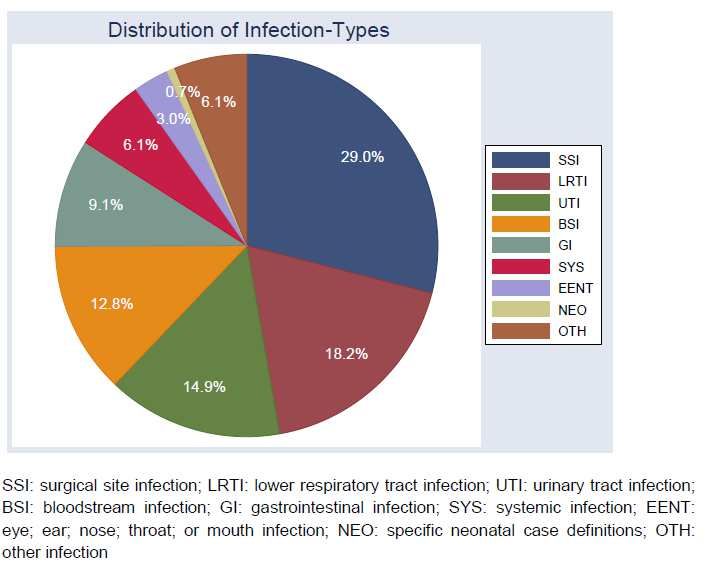
21.05.2019
Cathéter permanent vs. cathétérisme intermittent (gynécologie)
Moins d’infections avec cathétérisme intermittent
1 étude (2011)
N= 42
Li M, et al. Int Urogynecol J. 2019 Apr 9;30(4):523–35.
Intervention hospitalière
Sao Paolo (Brésil)
Soins intensifs : 34 lits
7.6 (IC95% 6.6- 8.6) 5.0 (IC95% 4.2-5.8)
Services (‘étage’): 40 lits
15.3 (IC95% 13.9-16.6) 12.9 (IC95% 11.6-14.2)
4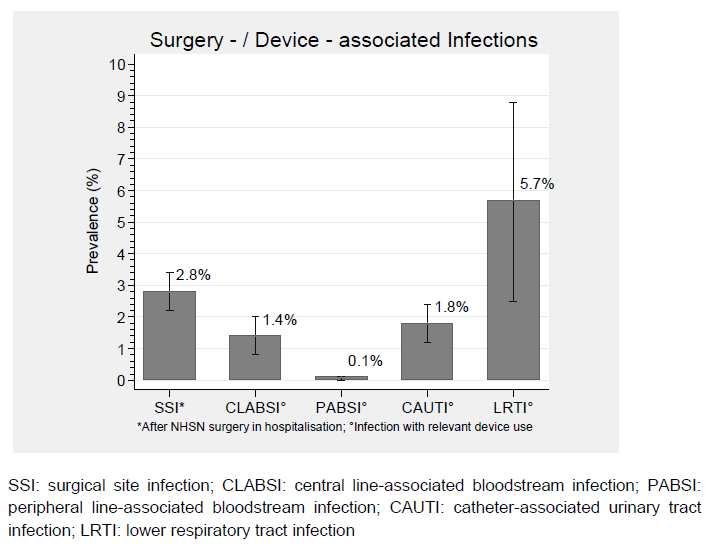
21.05.2019
Effets des mesures
Compter les événements adverses aux soins intensifs
Jain M, et al. Qual Saf Health Care. 2006 Aug;15(4):235–9.
Connaissance: indications et mesures préventives
6 EMS, Michigan USA, 2006
Assistantes
Question Infirmières
en soins
N (%) juste N(%) juste p
Indications:
Rétention avec échec de cath. intermittent 99 (88%) 164 (75%)
Grandes escarres 93 (83%) 159 (60%)
Maladie terminale (traitement de confort) 83 (74%) 152 (70%)
Mesures d’hygiène
Désinfection des mains, avant manipulation 99 (93%) 218 (98%) 0.008
Désinfection des mains, après manipulation 99 (93%) 216 (97%)
Mesures non recommandées de soin du cathéter
Le cathéter peut être débranché 59 (57%) 63 (29%) < 0.001
Le cathéter devrait être rincé 1x/semaine 50 (48%) 18 (8%) < 0.001
Mody L,et al Am J Am Geriatr Soc. 2010 Aug;58(8):1532–7.
5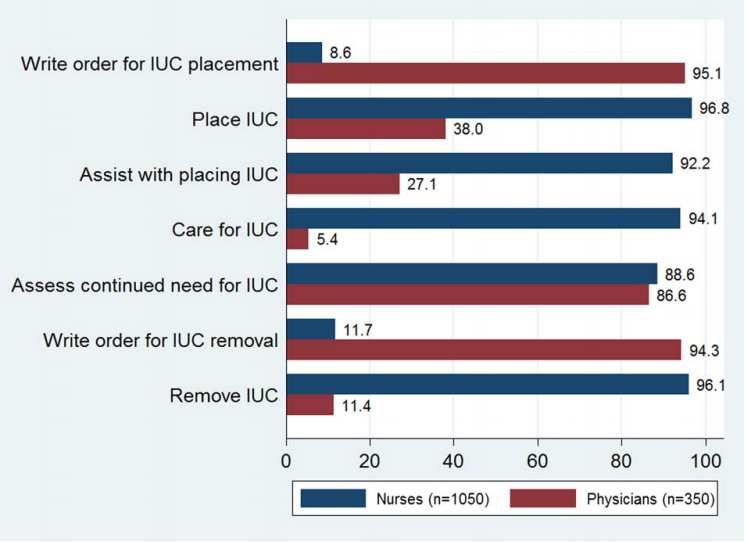
21.05.2019
Formation
Questionnaire: EMS Royaume Uni, 2005
Formation reçue (soins de sonde vésicale)
Infirmières 83%
Autres soignants 40%
McNulty C et al. J Hosp Infect. 2006 Jan;62(1):29–36.
Progress !
2016
1. une liste des indications
2. un contrôle quotidien de la nécessité de
la sonde vésicale (réévaluation)
3. la formation du personnel pour une
gestion sûre des sondes urinaires
6
21.05.2019
Collaboration: Qui fait quoi ?
Niederhauser A, et al. J Patient Saf. 2018 29;
7
21.05.2019
Résultats ‘progress’ 2016 - 2018
Selon le rapport final du projet pilote
• Moins de sondes (taux de portage de SV): 24% à 21%
• Moins de complications: 0.8 à 0.6 complications / 100 jours-patient
• Taux d’infection ‘bas et stable’: 1.0 à 1.3 infections / 1000 jours de SV
• Quels critères ?
(les résultats ne sont pas publiés dans le détail)
Züllig S. La sécurité dans le sondage vésical. Recommandations de progress! La
sécurité dans le sondage vésical. 2018
Perspectives
La force du programme pilote Progress !
• 1ère intervention coordonnée en Suisse
• déjà démontré un impact
• bonne acceptation
• formation : possible
8
21.05.2019
Mesures proposées pour réduire les infections sur cathéter
Réduction de l’utilisation
• Indication restrictive
• Ablation rapide
• Programme incontinence
Mesures spécifiques
• Pose aseptique (presque-stérile)
• Système clos
• Eviter le reflux dans la vessie
• Cathéter fixé
• Manipulation aseptique
Précautions standard
• Hygiène des mains
Système clos
Système fermé Port de prélèvement
Pas de déconnexion
Robinet pour vider
9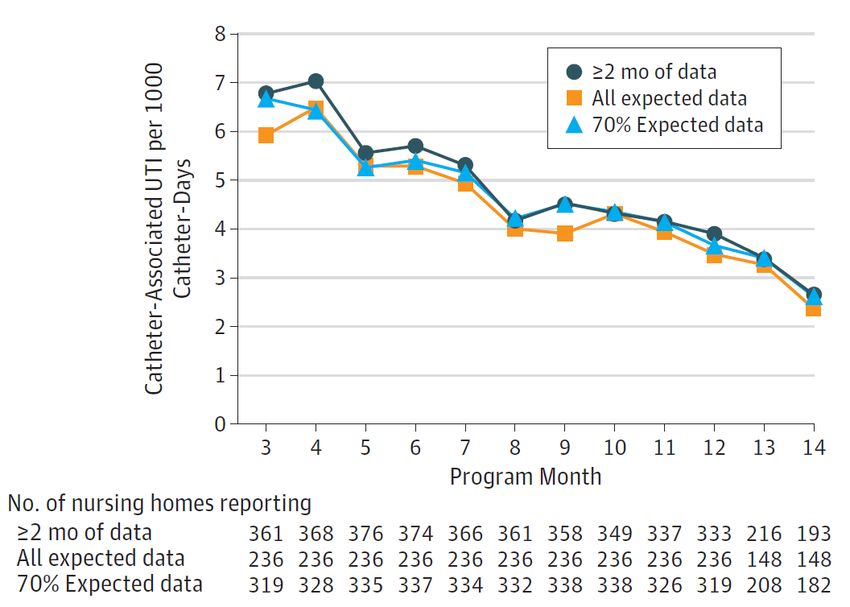
21.05.2019
Valve Anti-Reflux
Intervention pour réduire les UI sur cathéter long terme
2010 – 2013
418 résidents d’EMS avec SV à demeure (34’174 jours d’observation)
Etude pilote
Infections cliniquement documentées OR IC95%
• Réduction 1ère infection 0.54 0.3-0.97
• Réduction infections suivantes 0.7 0.5-0.99
Portage BMR
• MRSA 0.8 0.64–0.96
• VRE - ns.
• BLSE/CRE - ns.
Mody L, et al. JAMA Intern Med. 2015 May 1;175(5):714–23.
1021.05.2019
Paquet de mesures
Programme national (USA)
Enlever les cathéters non-nécessaires
Insertion aseptique par du personnel formé
Evaluation de l’indication au cathéter, à intervalle régulier
- incontinence: pas une indication en soi
Formation des soignants, résidents, famille
- Système fermé
- Maintient du flux sans obstruction
- Précautions standard (hygiène des mains)
- Proscrire des pratiques déconseillées:
- changement, analyse d’urine ou culture par routine
- désinfection de la zone péri-urétrale
- rinçage du cathéter
Indications acceptées
- Guérison d’escarre sacral chez résident avec incontinence
- Obstruction
- Soins de fin de vie (visée: confort)
Mody L, et al. JAMA Intern Med. 2017 1;177(8):1154–62.
Implicitement
Surveillance
- Définitions CDC: Surveillance Definitions of Infections in Long-Term Care Facilities
Antimicrobial stewardship
- Diagnostic et traitement de l’infection urinaire
Stone ND, et al. Infect Control Hosp Epidemiol. 2012 Oct;33(10):965–77.
1121.05.2019
Effet du programme
404 homes (USA)
-54%
Mody L, et al. JAMA Intern Med. 2017 1;177(8):1154–62.
Différences entre les homes
• Meilleur effet des mesures dans homes publics (vs. homes orientés profit)
• 75% des homes : ≥40% de réduction
• Estimation du travail d’intervention: 11 heures/semaine par home
• Pas de changement du taux de SV: 4.5% (stable sur l’étude)
Mody L, et al. JAMA Intern Med. 2017 1;177(8):1154–62.
1221.05.2019
Recettes pour le succès
Liste non exhaustive, adaptée
• Regarder le cycle de vie de la SV dans son ensemble
• indication, pose, maintien
• ablation ‘automatique’
• Assurer les standards PCI
• audit
• Multidisciplinaire,
• Inter-groupe professionnel (soignants – médecins)
• agents désignés sur place
• (Ressources)
Patel PK, et al. J Hosp Med. 2018 01;13(2):105–16.
Surveillance
Critères cliniques = ressources humaines
Critères non spécifiques
I. Without an indwelling catheter (both criteria 1 and 2 must be present)
…
II. With an indwelling catheter (both criteria 1 and 2 must be present)
1. At least 1 of the following sign or symptom subcriteria
A. Fever, rigors, or new-onset hypotension, with no alternate site of infection
B. Either acute change in mental status or acute functional decline, with no alternate diagnosis and leukocytosis
C. New-onset suprapubic pain or costovertebral angle pain or tenderness
D. Purulent discharge from around the catheter or acute pain, swelling, or tenderness of the testes, epididymis, or prostate
2. Urinary catheter specimen culture with at least 105 cfu/mL of any organism(s)
Stone ND, et al. Infect Control Hosp Epidemiol. 2012 Oct;33(10):965–77.
1321.05.2019
Critères d’infection urinaire (EMS)
I. Without an indwelling catheter (both criteria 1 and 2 must be present)
1. At least 1 of the following sign or symptom subcriteria
A. Acute dysuria or acute pain, swelling, or tenderness of the testes, epididymis, or prostate
B. Fever or leukocytosis (see Table ’Constitutional Criteria‘) and at least 1 of the following localizing urinary tract subcriteria
• Acute costovertebral angle pain or tenderness
• Suprapubic pain
• Gross hematuria
• New or marked increase in incontinence
• New or marked increase in urgency
• New or marked increase in frequency
C. In the absence of fever or leukocytosis, then 2 or more of the following localizing urinary tract subcriteria
• Suprapubic pain
• Gross hematuria
• New or marked increase in incontinence
• New or marked increase in urgence
• New or marked increase in frequency
2. One of the following microbiologic subcriteria
A. At least 105 cfu/mL of no more than 2 species of microorganisms in a voided urine sample
B. At least 102 cfu/mL of any number of organisms in a specimen collected by in-and-out catheter
II. With an indwelling catheter (both criteria 1 and 2 must be present)
1. At least 1 of the following sign or symptom subcriteria
A. Fever, rigors, or new-onset hypotension, with no alternate site of infection
B. Either acute change in mental status or acute functional decline, with no alternate diagnosis and leukocytosis
C. New-onset suprapubic pain or costovertebral angle pain or tenderness
D. Purulent discharge from around the catheter or acute pain, swelling, or tenderness of the testes, epididymis, or prostate
2. Urinary catheter specimen culture with at least 105 cfu/mL of any organism(s)
Stone ND, et al. Infect Control Hosp Epidemiol. 2012 Oct;33(10):965–77.
Perspectives
La force du programme pilote Progress !
• 1ère intervention coordonnée en Suisse
• il a déjà démontré un impact
• bonne acceptation
• la formation est possible
Les défis
• Collaboration entre médecins et soignants
• Extension à la prévention des infections sur SV
• Diagnostic et traitement des infections / stewardship
• Surveillance des infections
• Simplifier et automatiser les critères
• Pérennisation et extension du programme
• à plus d’hôpitaux, pas seulement les ‘motivés’
• aux EMS
• Ressources
1421.05.2019
Et en Suisse latine ?
Merci pour votre attention !
Critères d’infection urinaire (EMS)
I. Without an indwelling catheter (both criteria 1 and 2 must be present)
1. At least 1 of the following sign or symptom subcriteria
A. Acute dysuria or acute pain, swelling, or tenderness of the testes, epididymis, or prostate
B. Fever or leukocytosis (see Table ’Constitutional Criteria‘) and at least 1 of the following localizing urinary tract subcriteria
• Acute costovertebral angle pain or tenderness
• Suprapubic pain
• Gross hematuria
• New or marked increase in incontinence
• New or marked increase in urgency
• New or marked increase in frequency
C. In the absence of fever or leukocytosis, then 2 or more of the following localizing urinary tract subcriteria
• Suprapubic pain
• Gross hematuria
• New or marked increase in incontinence
• New or marked increase in urgence
• New or marked increase in frequency
2. One of the following microbiologic subcriteria
A. At least 105 cfu/mL of no more than 2 species of microorganisms in a voided urine sample
B. At least 102 cfu/mL of any number of organisms in a specimen collected by in-and-out catheter
II. With an indwelling catheter (both criteria 1 and 2 must be present)
1. At least 1 of the following sign or symptom subcriteria
A. Fever, rigors, or new-onset hypotension, with no alternate site of infection
B. Either acute change in mental status or acute functional decline, with no alternate diagnosis and leukocytosis
C. New-onset suprapubic pain or costovertebral angle pain or tenderness
D. Purulent discharge from around the catheter or acute pain, swelling, or tenderness of the testes, epididymis, or prostate
2. Urinary catheter specimen culture with at least 105 cfu/mL of any organism(s)
Stone ND, et al. Infect Control Hosp Epidemiol. 2012 Oct;33(10):965–77.
1521.05.2019
Critères constitutionnels (EMS)
Definitions for Constitutional Criteria in Residents of Long-Term Care Facilities (LTCFs)
1. Fever
1. Single oral temperature >37.8°C (>100°F)
2. OR
3. Repeated oral temperatures >37.2°C (99°F) or rectal temperatures
>37.5°C (99.5°F)
4. OR
5. Single temperature >1.1°C (2°F) over baseline from any site (oral,
tympanic, axillary)
2. Leukocytosis
3
1. Neutrophilia (>14,000 leukocytes/mm )
2. OR
3
3. Left shift (>6% bands or ≥1,500 bands/mm )
3. Acute change in mental status from baseline (all criteria must be present;
see Table ‘Confusion’)
1. Acute onset
2. Fluctuating course
3. Inattention
4. AND
5. Either disorganized thinking or altered level of consciousness
4. Acute functional decline
1. A new 3-point increase in total activities of daily living (ADL) score
(range, 0–28) from baseline, based on the following 7 ADL items, each
14
scored from 0 (independent) to 4 (total dependence)
1. Bed mobility
2. Transfer
3. Locomotion within LTCF
4. Dressing
5. Toilet use
6. Personal hygiene
7. Eating
Stone ND, et al. Infect Control Hosp Epidemiol. 2012 Oct;33(10):965–77.
Confusion
Confusion Assessment Method Criteria
Evidence of acute change in resident’s mental
Acute onset
status from baseline
Behavior fluctuating
Fluctuating (eg, coming and going or changing in severity during the
assessment)
Inattention Resident has difficulty focusing attention
(eg, unable to keep track of discussion or easily distracted)
Resident’s thinking is incoherent
Disorganized thinking (eg, rambling conversation, unclear flow of ideas, unpredictable
switches in subject)
Resident’s level of consciousness is described as
Altered level of consciousness different from baseline
(eg, hyperalert, sleepy, drowsy, difficult to arouse, nonresponsive)
Stone ND, et al. Infect Control Hosp Epidemiol. 2012 Oct;33(10):965–77.
16Vous pouvez aussi lire