Screening for cervical cancer - Canadian programmatic guidelines
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous
I X
Screening for cervical cancer
Canadian programmatic guidelines
Jean Parboosingh, MB, CHB, MSC
Programmatic guidelines' have recently been published * Organized programs allow for evaluation and monitoring
by the Quality Management Working Group of the of screening and follow-up activities.
Cervical Cancer Prevention Network, an informal associa- Clinical practice guidelines are only one component of
tion of federal and provincial representatives with the rele- organized screening programs. Other components include
vant clinical professional bodies. Represented on the recruitment strategies at public, patient, and professional
Working Group are the Society of Obstetricians and levels; information systems; continuous management of the
Gynaecologists of Canada, the College of Family Physicians quality of care provided; and professional education. A key
of Canada, the Canadian Society of Cytology, the concept for programs to adopt is the ability to assess new
Gynaecologic Oncologists of Canada, the Society of research findings that provide information or evidence for
Canadian Colposcopists, and the Canadian Association of change in practice.
Pathologists.
The guidelines incorporate and reference existing Primary care practice
approaches and documentation on practice and education Information for women before a Pap smear. Primary
of relevant Canadian specialties where available. The follow- care providers should have patient education material avail-
ing extracts from the full document are those of primary able or should inform women that the purpose of the Pap
interest to family physicians and provide a rationale for smear is to identify precancerous lesions in order to prevent
developing organized programs, of which these guidelines cervical cancer. Many women find the procedure embar-
are one component. rassing, uncomfortable, and traumatic and might never
return after their first Pap smear. To encourage women to
Need for organized programs in Canada return, practitioners should explain the procedure, answer
Screening for cervical cancer has occurred opportunistical- questions, and communicate throughout the procedure. A
ly in Canada since the 1970s. Overall incidence and mortali- sensitive environment will help alleviate anxiety.
ty have declined considerably since then. Now, however, we Women should be informed at the time the appointment
must address cervical cancer screening systematically for is made that certain conditions are better than others for
the following reasons. screening and that the vagina should not be douched for 48
* Cancer of the cervix is a preventable disease, yet a sub- hours before examination.
stantial number of cases occur in Canada each year. Smears should not be taken during menstruation. The
* It is economically sound to prevent the disease. optimal time is midcycle or just before ovulation, and
* Since the 1970s, recommendations have been made for women should be informed that the date of their last men-
establishing provincially based, organized programs. strual period will be required. However, if these conditions
* More recently, the rate of decline of the disease in cannot be met and it is possible that a woman will not
women younger than 50 has decreased in Canada. return, a Pap smear should be done.
* Opportunistic screening does not achieve optimal screen- Primary care providers and their office staff should
ing coverage and appears to have reached the limit of its have an agreed-upon policy for advising patients of results
effectiveness. and should inform patients of how the information will be
* Women who are diagnosed with the disease are those communicated.
who have not been screened.
* Organized programs have been shown to be effective. Primary care practitioners. Most historical series cite
* The costs of organized programs are probably less than sampling problems as the cause of more than half the
the costs of opportunistic screening. false-negative smear results.23 Reasons for sampling
- FOR PRESCRIBING INFORMATION SEE PAGE 496 VOL45: FEBRUARY * 1FVRIER 1999Canadian Family Physician Le Medecin defamille canadien 383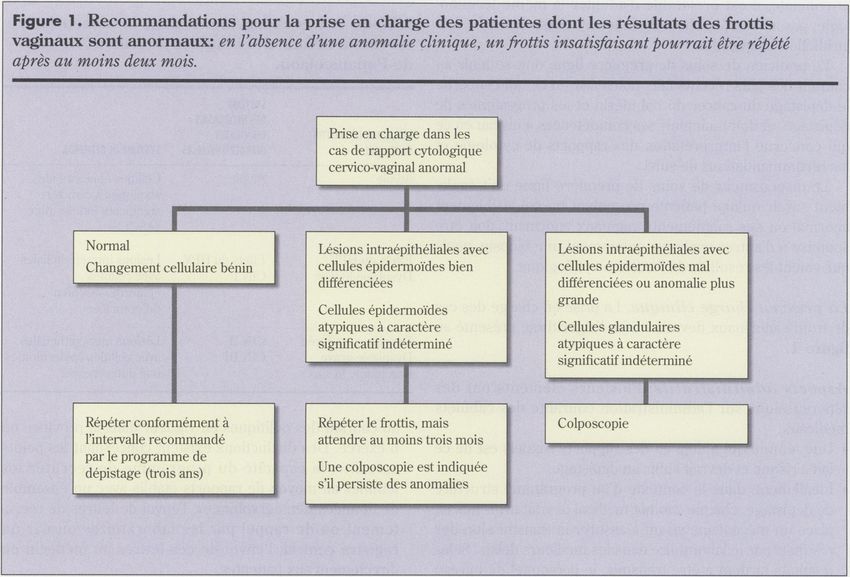
RESOURCES * RESSOURCES
errors could be the location of the lesion (eg, within the visible. They then should be able to describe the transfor-
endocervix), specific patient variables (eg, presence of mation zone; distinguish a normal cervix from a cervix with
blood or inflammatory material), or incomplete sampling obvious abnormalities; identify the appropriate tools with
(ie, poor technique). which to take a smear; take the smear, transfer material to
Training and maintenance of competence: In medical the slide, and fix the smear; and take the relevant history
school, students should be taught to take Pap smear sam- for completing the cytology requisition form.
ples, to interpret results, and to ensure appropriate follow There are three sampling areas of the cervix: the exo-
up or referral. They should learn: cervix (covered by squamous epithelium), the transforma-
* that cervical cancer is a preventable disease; tion zone (covered by metaplastic epithelium), and the
* that the Pap smear is an effective screening test; endocervix (covered by columnar epithelium). During high
* that all sexually active women are at risk; estrogen states, such as puberty and pregnancy, the visible
* that regular smears are recommended for women with squamocolumnar junction might become more exposed to
normal smears; and the outside portion of the cervix and be visible to the naked
* that there are nationally accepted recommendations eye. It is from this area of the visible squamocolumnar junc-
for follow up and treatment of women with abnormal tion that cervical cytology samples should be obtained.
smear results. After menopause, the squamocolumnar junction tends to
Practitioners should recognize that opportunities for recede into the endocervical canal and cannot be readily
screening or for reminding women about regular screening viewed. For this reason, it might be necessary to use an
include routine visits for chronic care, pregnancy, contra- endocervical sampling device in addition to a spatula to
ception, and visits related to hormone replacement therapy. obtain an adequate sample from older women.
How to take a smear: Medical students, residents, and Required equipment includes an examining table, good
other health care providers should be able to expose the illumination, various sizes of bivalve specula, a wooden spat-
cervix with a bivalve speculum in such a manner that it is ula (wood allows good adherence of the sample before
20,
(%)deseetoihLSCplus metronidazole and clarithromycin include taste disturbances (14%), diarrhea (13%), headache(6%)and increased ALAT (6%).
Como
Common (>5%) adnerse enents with LOSEC plus amoxicillin and clarithromycin include diarrhea (28%) andtnastedisturbances (15%).1
384 Canadian Family Physician Le Medecin defamille canadien * VOL45: FEBRUARY * FEVRIER 1999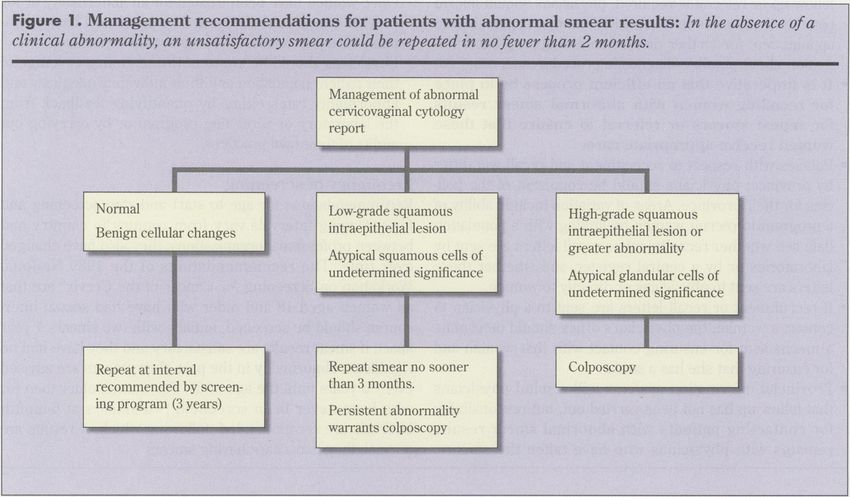
RESOURCES * RESSOURCES
transfer to the slide, eg, Ayre-type spatula), an endocervical recommended. The patient's name should be written in
sampling device, a glass microscope slide with frosted end, pencil on the frosted end of the slide.
a pencil for labeling the slide, a cytology spray fixative The requisition form should be completed by the per-
(unless otherwise informed by the laboratory to which the son taking the smear and should include the following rel-
slide is being sent), a container for transporting slides to evant clinical information: age; date of last menstrual
the laboratory, and requisition forms. Do not use lubricat- period; whether the patient is pregnant, or taking oral con-
ing jelly on the speculum. traceptives, or on hormone replacement therapy; presence
Several sampling techniques are acceptable. If the trans- of an intrauterine device; history of previous abnormal
formation zone is visible and easily sampled, the spatula smear results; history of hysterectomy (identified as total
alone can be used; if not, both the spatula and the endocer- or subtotal as appropriate); suspect appearance of cervix;
vical sampling device should be used. An endocervical history of previous treatment for an abnormality of the
sampling device alone should not be used. The spatula is cervix. Demographic information, such as name, health
used by applying it to the exocervix, incorporating the number, and physician name, is required by some provin-
squamocolumnar junction, and performing a 3600 scrape cial jurisdictions.
(keeping continuous contact with the cervix). An endocer- Medical students, residents, and primary care practition-
vical brush should be rotated 900 only. If an endocervical ers should understand the terminology used in reporting
sampling device is to be used, the woman should be cytology results and the reasons behind recommendations
informed that it might be uncomfortable and that spotting for follow up. Terminology has changed over the years. The
could occur. Canadian Society of Cytology4 recommends that The
The smear should be spread on one slide only and Bethesda System (TBS)5 be used in conjunction with dys-
fixed immediately unless air-drying is the choice of the plasia or cervical intraepithelial neoplasia systems
receiving laboratory. Spraying evenly across the slide with (Table 1). The obsolete numerical Papanicolaou class sys-
a cytologic spray fixative at a distance of 6 to 10 inches is tem of reporting should not be used. Within a provincial
myci~~~~~~~~~~~
Only LOSEC Trple Therapy* offers you the flexibility of two been shown equally effectivedTreatment lasts just seven days.
Three individually packaged medications provide the opportunity for clear direction from the pharmacist regarding the use of each medication.
A ~~Week of
~~~~~~~~~~
ASTRA treatment
A,,,._M.- 1- MJ,14-9 O na rua LOSEC* 12-3M and LOSEC* 1-2-3 A"
F1 areetrademarks of Astra PharmalInc. TRUSTED ACID CONTROL
Times a day
LOSEC in combination Wth clarithromyun and eu[her amouiclltn t To ensure healing and/or symptom control, further treatment auth Coonsderaton should be given to drug allergien and pasterns ol
or mesrontazole is indtcased lot the treatment of pasienos weh 20 mg LOSEConcedcaifyfor up to three wek srecommendedfor ancibsotic rensistance. Drug substoutenos mnay lead to unacceptable
peptic ulcerdseaea associated seth H pylor tnfecoon. The opomn-al patients witnactiv dluodenal ulcer and tih 20-f0mg LOShConce etadication rates~Consensus guidelines should tbe consulted '
slmung forteradcanon to pattents woeulcer istemt clinicallyactnve dailyfor uprto twlewesfor sateers sthactsv ganstric ulcer rh .eseT
r anttbaooc Product M uonogah smolc ste consulted Medications
(i.e.asympsomastc) rematns to bedetetmsned andhtollowe.
FOR PRESCRIBING INFORMATION SEE PAGE 537
VOL 45: FEBRUARY * FtVRIER 1999 + Canadian Family Physician Le Medecin defamille canadien 385
RESOURCES *. RESSOURCES
Primary care practitioners should also be aware that a
Table 1. Changing nomenclature for classifying patient with a visibly abnormal cervix or abnormal vaginal
abnormal Pap smear results bleeding should be subjected to further investigation,
including biopsy, regardless of the cytologic findings.
CERVICAL
INTRAEPITHELIAL Clinical management: Management of an abnormal
PAP SMEAR RESULTS NEOPLASIA SYSTEM THE BETHESDA SYSTEM smear should follow the algorithm in Figure 1.
Atypia Atypia Atypical squamous cells of
Office management: Several issues affect routine office
undetermined significance management.
(ASCUS) * A woman is at risk if she has ever been sexually active
....................................I............................I.........................................................
and should be screened.
HPV effects HPV effects Low-grade squamous
Mild dysplasia CIN 1 intraepithelial lesion * Ideally, within the context of an organized screening pro-
.......................................................................................................................... gram, each office should have a mechanism to ensure
Moderate dysplasia CIN 2 High-grade that results are obtained from the laboratory in a timely
Severe dysplasia CIN 3 squamous manner. If results are not received, office staff should ask
Carcinoma in situ intraepithelial lesion
laboratory staff to check that the laboratory received the
sample and that a report is forthcoming.
jurisdiction, it is preferred that one terminology be used; * Results need to be communicated to patients. If results are
however, the terminology is chosen by each jurisdiction. normal and require no immediate follow up or if the smear
Primary care practitioners should be aware of new infor- needs to be repeated for technical reasons, an office staff
mation regarding cervical cancer screening, screening pro- member could call the patient with this information, remind
grams, and recommendations for follow up and should her to return at the appropriate time if a normal result has
maintain their competence in taking samples and interpret- been obtained, or give her an appointment for a repeat
ing the reports of cytology results. smear when this is indicated. If results are abnormal and
S *_ *
*tPeaeso i/S
Final resuI
Hypertension
Treatment
Intenamtionol Study
386 Canadian Family Physician Le Midecin defamille canadien *V0L45: FEBRUARY *Fb,TRIER
1999RESOURCES * RESSOURCES
follow up or referral is required, physicians should inform Once women have been treated for an abnormality or for
patients themselves in a sensitive manner, suggesting an cervical cancer and discharged by specialists back to pri-
appointment for further discussion and appropriate infor- mary care physicians, follow up should be ensured.
mation about possible diagnostic procedures as required. * Physicians should be aware of the screening coverage of
* It is imperative that an efficient process be in place their patient population and their individual adequacy and
for recalling women with abnormal smear results abnormality rates either by quantifying feedback from
for repeat smears or referral to ensure that these the laboratory or screening program or by carrying out
women receive appropriate care. audits of their own practices.
* Policies with respect to recruitment and recall will differ
by province; physicians should be cognizant of the poli- Frequency of screening
cies for their province. Areas of variation include ability of Recommendations for age to start and stop screening and
a program to recruit women by linking with a population for screening intervals vary from country to country and
data set, whether recruitment or recall letters are sent by between professional organizations; they also have changed
laboratories or by a central register, and whether these over time. The recommendations of the 1989 National
letters are sent to physicians or directly to women. Workshop on Screening for Cancer of the Cervix6 are that
* If recruitment or recall letters are sent to a physician to all women aged 18 and older who have had sexual inter-
contact a woman, the physician's office should determine course should be screened, initially with two smears 1 year
a mechanism for ensuring contact with that woman and' apart; if smear results are satisfactory and they have had no
for ensuring that she has a smear. significant abnormality in the past, then smears are advised
* Provincial information systems will remind physicians every 3 years until the age of 69. For women older than 67,
that follow up has not been carried out, but responsibility who have never been screened, two smears at 6-month
for contacting patients with abnormal smear results intervals are recommended, following which, if results are
remains with physicians who have taken the smears. normal, they may cease having smears.
IdlX
I
With over 18,000 randomized hypertensive patients, the HOT Study, an independent international trial, demonstrates the
following: if a therapy is highly effective and well-tolerated, a high level of patients will continue with their therapy.2
PLENDIL. Start on it, stay on it.
To receive a copy of the HOT Study final results, please call Medical Information at 1-800-668-6000.
Average follow-up time was 3.8 years (range 3.3 - 4.9 years). t Additional ACE Inhibitor or 8-blocker used in some patients and possibly diuretics. PLENDIL is indicated in the treatment of mild to moderate essential
hypertension. PLENDIL should normally be used when a diuretic or beta blocker is found to be ineffective, or has been associated with unacceptable adverse effects or is contraindicated.3 PLENDIL should be used with caution to
treat hypertension in patients with heart failure until safety in these patients can be confirmed with additional clinical experience. Most common adverse effects were peripheral edema, headache and feeling of warmth and flushing.
AS T tA
Astr, Pharmo In,c., MMisssouo Ontario LAY IM4
|1 _ ONCE *A *DAY * * _
pd oft
CMA IMCANIAN
PMBC ] M Of
WA6 C_!- MEDICALE MEDK-AL _
CCPP 0 ICO Of d dl p VJ-- a Infobase CANADIENNE ASSOCIAMN
www.cma.ca/cpgs EMPdi
FEO I E aadenT 8
FOR PRESCRIBING INFORMATION SEE PAGE A52 VOL45: FEBRUARY*FtVR1ER 1999 0Canadian Family Physician .Le Medecin de famille canadienRESOURCES *: RESSOURCES
Management of abnormal
.~~ .~~ .~~.. .. ~~cervicovaginal cytology 4.
: |~;
'.~g *. , 1 ., Ireport
Normal Low-grade squamous High-grade squamous
| Benign cellular changes intraepithelial lesion _ intraepithelial lesion or
-- Atypical squamous cells of greater abnormality
,
_| undetermined signcance Atypical glandular cells of
undetermined significance
Repeat at interval Repeat smear no sooner Colposcopy
] recommended by screen- thano3 months.
Persistent abnormality
~~ u4~~~44r~~~4 ~ ~ ~ warrants colposcopy
The recommended interval of every 3 years is Dr Parboosingh is a Senior Medical Consultant in the Adult
predicated on the presence of a system for recall and Health Division of the Health Promotion and Programs Branch
quality assurance within an organized screening pro- of Health Canada in Ottawa, Ont.
gram. Opportunistic screening, based on annual
screening, depends on individual women's and their References
physicians' memories. 1. Cervical Cancer Prevention Network, Quality Management Working
After an initial smear result within normal limits, a Group. Programmatic guidelines for screeningfor cervical cancer in
woman infected with the human immunodeficiency virus Canada. Ottawa, Ont: Health Canada and the Society of Gynecologic
should have at least one additional smear within 6 months Oncologists of Canada; 1998.
to rule out the possibility of false-negative results on the ini- 2. Department of Health and Human Services. Improving the quality of
tial smear. If results of the repeat smear are normal, annual clinician Pap smear techniques and management, client Pap smear
smears are advised.7'8 For other women with immunosup- education, and the evaluation of Pap smear laboratory testing: a
pression, annual smears are also recommended. resource guidefor title Xfamily planning projects. Washington, DC:
If a woman has not had a smear in the past 5 years, it US Dept of Health and Human Services; 1989.
is suggested that she have two 1 year apart before start- 3. Gay JD, Donaldson LD, Goellner JR False negative rates in cervical
ing the 3-yearly routine (if results are normal). cytological studies. Acta Cytol 1985;29:1043-6.
The remainder of the document contains information 4. Canadian Society of Cytology. Guidelines for practice and quality assur-
on trends in incidence, mortality, and screening rates in ance in cytopathology. Montreal, Que: Canadian Society of Cytology; 1996.
Canada as well as on the effectiveness of organized 5. National Cancer Institute Workshop. The 1988 Bethesda system for
screening programs. Areas of practice relating to cytology reporting cervical/vaginal cytological diagnoses.JAMA 1989;262:931-4.
and cytology laboratories, colposcopy, gynecology, and 6. Miller AB, Anderson G, Brisson J, Laidlaw J, Le Pitre N,
gynecologic oncology are also included. To obtain a copy Macolmson P, et al. Report of a National Workshop on Screening for
of Programmatic Guidelines for Screening for Cervical Cancer of the Cervix. Can Med Assoc J 1991;145:1301-25.
Cancer in Canada, contact the Adult Health Division, 7. Hankins CA, Lamont JA, Handley MA. Cervicovaginal screening in
Health Promotion and Programs Branch, Health Canada, women with HIV infection: a need for increased vigilance? Can Med
by fax at (613) 941-2633; by mail at Postal Locator 1910C1, Assoc i 1994;150:681-6.
Tunney's Pasture, Ottawa, ON KlA 1B4; or by e-mail at 8. Maiman M, Fruchter RG, Clark C, Arrastia CD, Matthews R, Gates EJ.
Jean_Parboosingh@hc-sc.gc.ca. 4 Cervical cancer as an AIDS-defining illness. Obstet Gynecol 1997;89:76-80.
388 Canadian Family Physician Le Medecin defamille canadien * VOL 45: FEBRUARY * FEVRIER 1999RESOURCES + RESSOURCES
Le depistage du cancer du col uterin
Des lignes directrices pour les programmes au Canada
Jean Parboosingh, MB,CHB,MSC
Le groupe de travail sur la gestion de la qualite du . Les programmes structures prevoient des modalites
Reseau de prevention du cancer du col uterin, un d'evaluation et de surveillance du depistage et des acti-
regroupement informel de representants f6deraux et pro- vites de suivi.
vinciaux ainsi que des organismes professionnels cliniques Les guides de pratique clinique ne representent que
concernes, a recemment publie des lignes directrices pour l'une des composantes des programmes de depistage
les programmes 'a cet egard. Au nombre des associations structures. Au nombre des autres elements figurent les
representees au sein du groupe de travail figurent la strategies de recrutement au niveau du public, des
Societe des obstetriciens et gynecologues du Canada, le patients et des professionnels; les systemes d'information;
College des medecins de famille du Canada, la Societe cana- l'assurance continuelle de la qualite des soins prodigues;
dienne de cytologie, la Societe des gynecologues onco- et l'education professionnelle. Les programmes devraient
logues du Canada, la Societe des colposcopistes du Canada adherer au principe qu'ils doivent etre en mesure d'eva-
et l'Association canadienne des pathologistes. luer les nouveaux resultats de recherche qui procurent les
Les lignes directrices englobent les approches et la renseignements ou les donnees probantes justifiant des
documentation existantes entourant la pratique et l'educa- modifications aux pratiques.
tion dans les specialites canadiennes pertinentes, la oiu elles
sont disponibles, et le texte y fait ref6rence. Les extraits sui- La prestation des soins de premiere ligne
vants, tires du document original, concernent principale- Information des patientes avant la realisation d'un
ment les m6decins de famille. Ils expliquent les motifs qui frottis. Le dispensateur de soins de premiere ligne doit
justifient l'elaboration de programmes structures, dont les pouvoir offrir des documents d'information 'a sa patiente ou
presentes lignes directrices font partie. lui expliquer que l'objet du frottis est de depister les lesions
precancereuses afin de prevenir le cancer du col uterin.
La necessite d'avoir des programmes structures Bon nombre de femmes trouvent l'intervention genante et
au Canada inconfortable. Pour encourager ses patientes 'a revenir, le
Depuis les annees 1970, on procede au depistage du cancer praticien doit leur expliquer en quoi consiste l'intervention,
du col uterin au Canada. Meme si l'initiative a et ciblee un repondre 'a leurs questions et communiquer avec elles tout
peu au hasard, c'est 'a partir de ce moment que l'incidence au long de l'intervention; une atmosphere receptive contri-
globale et la mortalite ont baisse considerablement. buera 'a soulager l'anxiete.
Toutefois, il nous faut maintenant aborder systematique- Lors de la prise du rendez-vous, il faut expliquer 'a la
ment le depistage du cancer du col uterin pour les raisons patiente que certaines conditions sont plus propices que
suivantes: d'autres au depistage et qu'elle doit eviter toute douche
. Le cancer du col uterin est une maladie qu'il est possible vaginale durant les 48 heures pr&cedant l'examen.
de prevenir et pourtant, un nombre considerable de cas Les frottis ne doivent pas etre effectues durant les mens-
sont diagnostiques chaque annee au Canada. truations. Le moment optimal est le milieu du cycle ou
. Il est rentable de proceder 'a la prevention de cette immediatement avant l'ovulation, et il faut prevenir la
maladie. patiente qu'on lui demandera la date de ses dernieres
. Depuis les annees 1970, il a ete recommande d'etablir des regles. Cependant, si ces conditions ne peuvent etre rem-
programmes structures sur le plan provincial. plies, et s'il est possible qu'elle ne revienne pas, il faut
Recemment, la tendance 'a la baisse dans l'incidence de la quand meme effectuer un frottis.
maladie chez les femmes de moins de 50 ans a plafonne Le dispensateur de soins de premiere ligne et le per-
au Canada. sonnel de son cabinet doivent avoir une politique relative 'a
. Le depistage occasionnel ne permet pas de rejoindre le la communication des resultats 'a la patiente, et la patiente
public cible de maniere optimale et semble avoir atteint doit etre informee de la maniere dont l'information lui sera
les limites de son efficacite. donnee.
. Les femmes chez qui la maladie est diagnostiquee sont
celles qui n'ont pas subi d'epreuves de depistage. Le dispensateur de soins de premiere ligne. Dans la
. L'efficacite des programmes structures a ete demontree. majorite des etudes sur des series chronologiques, les pro-
. Le cou't des programmes systematiques est probable- blemes de prelevement sont la cause de plus de la moitie des
ment moins eleve que celui des depistages occasionnels. frottis faux negatifs2'3. Les erreurs de prelevement peuvent
VOL 45: FEBRUARY * FtVRIER 1999* Canadian Family Physician . Le Medecin defamille canadien 389RESOURCES * RESSOURCES
s'expliquer par l'emplacement de la lesion (par exemple a Le materiel requis est le suivant: une table d'examen, un
l'interieur de l'endocol), par certaines caracteristiques parti- bon eclairage, des speculums 'a double valve de differentes
culieres 'a la patiente (par exemple la presence de sang ou de tailles, une spatule en bois (e bois permet une bonne adhe-
materiel inflammatoire), ou par un prelevement incomplet rence de l'echantillon avant son transfert sur la lame; p. ex.
(c'est.-a-dire une technique deficiente). spatule d'Ayre), un outil de prelevement endocervical, une
La formation et le maintien des competences. Durant les lame de microscope en verre a extremite en verre depoli,
etudes 'a la faculte de medecine, on doit enseigner aux etu- un crayon pour identifier la lame, un fixatif cytologique en
diants la fa,on de realiser un frottis, l'interpretation des vaporisateur (sauf indication contraire du laboratoire
resultats, ainsi que les mesures appropriees de suivi ou auquel la lame sera envoyee), un contenant pour envoyer
d'aiguillage de la patiente. Is devraient savoir les points sui- les lames au laboratoire, et des formulaires de demande
vants: d'analyse cytologique. I1 ne faut pas appliquer de gelee
* le cancer du col uterin est une maladie potentiellement lubrifiante sur le speculum.
evitable; Plusieurs techniques de prelevement sont acceptables.
. le frottis cervical est un test de depistage efficace; Si la zone de transformation n'est pas visible et s'il est diffi-
. toutes les femmes qui ont deja eu une activite sexuelle cile d'y acceder, il faut utiliser l'outil de prelevement endo-
sont 'a risque; cervical en plus de la spatule. On ne doit pas utiliser seul un
. on recommande des frottis reguliers pour les femmes outil de prelevement endocervical. Pour utiliser la spatule,
presentant des resultats normaux aux tests; l'appliquer sur l'exocol, incluant la jonction squamo-cylin-
. il existe des recommandations adoptees 'a l'echelle natio- drique, et gratter la surface en effectuant une rotation de
nale relativement au suivi et au traitement des femmes 3600 tout en maintenant un contact constant avec le col.
presentant des frottis anormaux. Avec une brosse endocervicale, la rotation ne doit etre que
Les praticiens doivent tirer profit de toutes les occasions de 900. Si l'on doit utiliser un outil de prelevement endocer-
pour effectuer un depistage ou pour rappeler 'a leurs vical, il faut avertir la patiente que l'intervention peut etre
patientes de subir des examens reguliers, notamment lors desagreable et qu'elle comporte des risques de petites
de leurs visites de routine pour recevoir des soins chroni- pertes sanglantes.
ques, ou encore pour un suivi de grossesse, de contracep- Le frottis doit etre etale sur une lame seulement et etre
tion ou d'hormonotherapie substitutive. fixe immediatement, sauf si le laboratoire de destination
Comment re'aliser un frottis. L'etudiant en medecine, le prefere un sechage a l'air. On recommande de vaporiser
resident ou tout autre praticien doit etre en mesure uniformement un fixatif cytologique a une distance de 6 a
d'exposer le col 'a l'aide d'un speculum 'a deux valves de 10 pouces de la lame. Les renseignements sur la patiente
maniere 'a ce qu'il soit visible, de decrire la zone de transfor- demandes par le laboratoire sont inscrits au crayon sur
mation, de distinguer un col normal d'un col presentant des l'extremite en verre givre de la lame.
anomalies evidentes, de connaitre les outils appropries uti- Le formulaire de demande d'examen cytologique est
lises pour realiser un frottis, de realiser le frottis, de le rempli par la personne qui a realise le frottis et doit inclure
transferer sur la lame et de le fixer, de prendre en note les les renseignements cliniques pertinents suivants: l'age; la
ant&cedents pertinents pour remplir le formulaire de date des dernieres regles; si la patiente est enceinte, si elle
demande d'examen cytologique. prend des contraceptifs oraux ou si elle suit une hormono-
Le col uterin comporte trois zones de prelevement: therapie substitutive; la presence d'un sterilet; les antece-
l'exocol (recouvert par l'epithelium malpighien), la zone de dents de frottis anormaux; les antecedents d'hysterectomie
transformation (recouverte par l'epithelium metaplasique) totale ou partielle selon le cas; l'aspect suspect du col; les
et l'endocol (recouvert par l'epithelium cylindrique). antecedents de traitement d'une anomalie du col. Les ren-
Lorsque la secretion d'oestrogenes est importante, par seignements d'ordre demographique comme le nom, le
exemple lors de la puberte et de la grossesse, la jonction numero d'assurance-maladie et le nom du me'decin varient
squamo-cylindrique visible peut devenir encore plus selon les lois provinciales en vigueur.
exposee dans la partie exterieure du col et etre visible 'a L'etudiant en medecine, le resident et le dispensateur de
l'oeil nu. C'est dans la region de la jonction squamo- soins de premiere ligne doivent comprendre la termino-
cylindrique visible qu'il faut prelever les echantillons cytolo- logie utilisee dans les rapports d'examen cytologique ainsi
giques cervicaux. que les motifs sous-tendant une recommandation de suivi.
Apres la menopause, la jonction squamo-cylindrique La Societe canadienne de cytologie4 recommande le recours
tend 'a reculer dans le canal endocervical et devient moins au systeme de Bethesda5 combine aux systemes de la dys-
facilement visible. Pour cette raison, il peut etre necessaire plasie et des neoplasies intraepitheliales du col uterin
d'utiliser un outil de prelevement endocervical en plus de la (Tableau 1). Il faudrait abandonner l'usage du systeme
spatule pour obtenir un prelevement adequat chez les desuet de classification numerique de Papanicolaou aux
femmes plus agees. fins des rapports. Dans le contexte d'une competence
390 Canadian Family Physician . Le Medecin defamille canadien o VOL45: FEBRUARY * FtVRIER 1999RESOURCES + RESSOURCES
provinciale, il est preferable d'adopter la meme termino-
logie; par ailleurs, le choix de la terminologie incombe 'a la Tableau 1. Les changements dans la nomenclature
juridiction en question. servant a definir des r6sultats anormaux de test
Le praticien de soins de premiere ligne doit se tenir au de Papanicolaou.
courant des plus recents faits nouveaux en ce qui concerne
le depistage du cancer du col uterin et les programmes de SYSTEME
depistage, et doit maintenir ses competences a niveau en ce DES NEOPLASIES
RESULTATS DE FROTTIS CERVICALES
qui concerne l'interpretation des rapports de cytologie et VAGINAUX INTRAEPITHELIALES SYSTEME DE BETHESDA
les recommandations de suivi.
Le dispensateur de soins de premiere ligne doit egale- Atypie Atypie Cellules epidermoides
atypiques 'a caractere
ment savoir qu'une patiente presentant un col visiblement significatif indetermine
anormal ou des saignements vaginaux anormaux doit etre (ASCUS)
soumise 'a d'autres analyses, notamment une biopsie, quels ..........................................................................................................................
que soient les resultats de l'examen cytologique. Effets du HPV Effets du HPV Lesions intraepitheliales
Dysplasie legere CIN I avec cellules
epidermoides bien
La prise en charge clinique. La prise en charge des cas differenciees
de frottis anormaux devrait suivre l'algorithme present6 au ..........................................................................................................................
figure 1. Dysplasie moderee CIN II Lesions intraepith6liales
Dysplasie grave CIN III avec cellules epidermoides
Carcinome in situ mal differenciees
Aspects administratifs: Plusieurs elements ont des
repercussions sur l'administration courante des cabinets
medicaux. au courant des politiques en vigueur dans la province otu
* Une femme qui a dej"a eu des rapports sexuels est de ce il exerce. Des distinctions existent concernant les points
fait 'a risque et devrait subir un depistage. suivants: la capacite du programme de recruter les
* Idealement, dans le contexte d'un programme structure femmes au moyen de rapports etablis avec un ensemble
de depistage, chaque cabinet medical devrait avoir mis en de donnees demographiques; l'envoi de lettres de recru-
place un mecanisme visant 'a assurer la transmission des tement ou de rappel par les laboratoires ou par un
resultats par le laboratoire dans les meilleurs delais. Si les registre central; l'envoi de ces lettres au medecin ou
resultats tardent a etre transmis, le personnel de bureau directement aux patientes.
doit communiquer avec le laboratoire afin de verifier que * Si les lettres de recrutement ou de rappel sont envoyees
le specimen a bien ete re,u et que le rapport sera au medecin, un mecanisme doit 'tre en place dans son
transmis sous peu. cabinet pour s'assurer que la patiente soit bien rejointe et
* Les resultats doivent etre communiques 'a la patiente. Si qu'elle subisse un frottis.
le resultat est normal, et qu'aucun suivi immediat n'est * Si les systemes d'information provinciaux rappelleront au
necessaire, ou encore si le frottis doit etre repete pour medecin qu'il n'y a pas eu de suivi, la responsabilite de
des raisons techniques, un membre du personnel admi- contacter les patientes ayant obtenu des resultats anor-
nistratif peut appeler la patiente pour lui donner cette maux demeure celle du medecin qui a realise le frottis.
information, lui rappeler de revenir au moment approprie Une fois que la patiente a ete traitee pour une anomalie
si le resultat etait normal, ou lui donner un rendez-vous ou un cancer du col et que le specialiste a renvoye son
pour un nouveau frottis au besoin. Si les resultats sont dossier au medecin de soins de premiere ligne, ce der-
anormaux et s'il faut suivre ou referer la patiente, le nier doit assurer le suivi
medecin doit l'informer lui-meme de cette situation en fai- * Les medecins doivent se tenir au courant de la proportion
sant preuve de sensibilite, et doit prendre rendez-vous de leurs patientes qui sont couvertes par le depistage et
avec elle pour lui donner des renseignements plus de leurs taux de resultats positifs et negatifs, soit par des
detailles sur les procedures diagnostiques envisageables, calculs effectues sur la base des renseignements fournis
le cas echeant. par le laboratoire ou par le programme de depistage, soit
* Il est imperatif d'avoir mis en place un processus par des verifications de leurs propres dossiers.
efficient pour le rappel des patientes dont le frottis
est anormal afin d'effectuer un nouveau frottis ou La fr6quence du depistage
de les aiguiller vers d'autres ressources, de D'un pays et d'une organisation professionnelle 'a l'autre,
maniere A s'assurer qu'elles recevront les soins les recommandations varient quant 'a l'age ou il est
appropries. indique de commencer et d'arreter le depistage; elles ont
* Les politiques en matiere de recrutement et de rappel dif- aussi evolue avec le temps. Les recommandations de
ferent d'une province 'a l'autre; chaque medecin doit etre l'Atelier national de 1989 sur le depistage du cancer du
VOL45: FEBRUARY * FtVRER 1999 +Canadian Family Physician . Le Medecin defamille canadien 391RESOURCES *: RESSOURCES col uterin6 preconisaient le depistage chez toutes les Si une femme n'a pas subi d'epreuve de depistage au femmes de 18 ans et plus qui avaient eu des rapports cours des cinq dernieres annees, il est suggere qu'elle sexuels, initialement au moyen de deux frottis 'a une subisse deux tests a une annee d'intervalle avant annee d'intervalle; si les resultats du frottis etaient satis- d'adopter la routine du frottis aux trois ans (si les resul- faisants et qu'ils n'avaient pas presente d'anomalies signi- tats sont normaux). ficatives par le passe, on recommandait de proceder 'a un Le reste du document comporte des renseignements frottis a tous les trois ans jusqu'a l'age de 69 ans. Chez les sur les tendances dans l'incidence, sur la mortalite et les femmes de plus de 67 ans qui n'avaient jamais et assujet- taux de depistage au Canada, ainsi que sur l'efficacite ties au depistage, on recommande deux frottis a six mois des programmes structures de depistage. II porte egale- d'intervalle et si les resultats sont normaux, elles peuvent ment sur d'autres domaines de la pratique concernant la cesser de subir les tests. cytologie et les laboratoires de cytologie, la colposcopie, La recommandation d'un intervalle de trois ans la gynecologie et l'oncologie gynecologique. Pour presume l'existence d'un systeme de rappel et de obtenir une copie des Lignes directrices pour les pro- modalites d'assurance de la qualite dans le contexte grammes de depistage du cancer du col uterin au Canada, d'un programme de depistage structure. Le depis- veuillez communiquer avec la Division de la sante des tage occasionnel, c'est-A-dire annuel, se fie a la adultes, Direction generale de la promotion et des pro- memoire de chaque femme et a celle de leur grammes de sante, Sante Canada, par telecopieur au medecin. (613) 941-2633; par courrier au Repere postal 1910C1, A la suite d'un resultat de test initial qui se situe dans Parc Tunney, Ottawa, Ontario KlA 1B4; ou par courriel une marge acceptable, une femme atteinte du virus de a Jean_Parboosingh@hc-sc.gc.ca + l'immunodeficience humaine devrait subir au moins un autre test dans les six mois qui suivent, pour eliminer la DT Parboosingh est consultante medicale principale a la possibilite de resultats faux negatifs lors du test anterieur. Division de la sante des adultes de la Direction generale de la Si les resultats du deuxieme frottis sont normaux, un depis- promotion et des programmes de sante de Sante Canada, a tage annuel est alors recommande. Ottawa, Ontario. 392 Canadian Family Physician . Le Medecin defamille canadien * VOL45: FEBRUARY * FVR1ER 1999
RESOURCES *. RESSOURCES
References assurance in cytopathology. Montreal, Que: Societe canadienne de
1. Reseau de prevention du cancer du col uterin, Groupe de travail sur cytologie; 1996.
la gestion de la qualite. Lignes directrices pour les programmes de 5. National Cancer Institute Workshop. The 1988 Bethesda system for
depistage du cancer du col uterin au Canada. Ottawa, Ontario: Sante reporting cervical/vaginal cytological diagnoses.JAMA 1989;262:9314.
Canada et la Societe des gynecologues oncologues du Canada; 1998. 6. Miller AB, Anderson G, Brisson J, LaidlawJ, Le Pitre N,
2. Department of Health and Human Services. Improving the quality of Macolmson P, et collegues. Report of a National Workshop on
clinician Pap smear techniques and management, client Pap smear Screening for Cancer of the Cervix. Can Med AssocJ 1991;145:1301-25.
education, and the evaluation of Pap smear laboratory testing: a 7. Hankins CA, Lamont JA, Handley MA. Cervicovaginal screening in
resource guide for title Xfamily planning projects. Washington, DC: women with HIV infection: a need for increased vigilance? Can Med
US Dept of Health and Human Services; 1989. AssocJ 1994;150:681-6.
3. Gay JD, Donaldson LD, Goellner JR. False negative rates in cervical 8. Maiman M, Fruchter RG, Clark C, Arrastia CD, Matthews R,
cytological studies. Acta Cytol 1985;29:1043-6. Gates EJ. Cervical cancer as an AIDS-defining illness. Obstet Gynecol
4. Societe canadienne de cytologie. Guidelines for practice and quality 1997;89:76-80.
. . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . ,.tC . . t.i
Availale i:
Af
.* ...d .il ...l.. . .e .. .......o
...£.. .. ........ ..
Canadians with arthritis is
growing a t a icrate of onem
lionarhrtsamn aaartii's 9. millio baybomrlae
perdecad.Mdclofcaslrmdb th rapidprad
eee
*.call z fo
a Cz
oas-tocoat-sratgy o;0 cpeith the dies's eii' a . .|#~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~i~ . o:...
~.....
physicianand member the~In
of Deatmn ofFnl eiie atgd
on iCanaians byatrts,iem .':2.~ ~ ~ ~9. . . ma
impraivethtw sm
e by theUnvri of
me..Toronto,Calgary
tof obese patients.Itwas nd ... ....
4. . |.~ ~:~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~
Z~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.
and Mdnreal.-Fr, coiso bst:O Cu 1-rita
Division. oc
s stud etas that th..........
numberS.trateg.7es for Primary.Care Ph$ciaus., contact.D~~~~~~eboa.Eltn?St .~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~
...
or LeslieWood at Lexicomm Communications (41368-0:
6) ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
and the numbe of 55 to 64yarods will mor.e thani doub3le. Fobr Cwsad*'4*a~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.
.s..et. for..a...ages ...
...
...
. ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~. . .
New guideinesfor treatingCtioP
N*~~~~~~~~~~.*.t...:..?. .:...g:.,'.
Canada, a societ/ralae,atmuit i o.AJtmtoa
.~~~~~~~~~~~~~~~~~~~~~~~~~.. ........ '........ . . . '.' :' . .'
N.e.w guidelin.e.s for: treatmentt;:of chrom.ic..obs.tuctive.pulmonary seniors'.
isus. I lo it.Itre.rsuce.T oti acwo
X Kt +| . . .~ ~ ~ ~ ~ ~locator.,
.~~~~~~..
*r.Panel,sktWr
werereleased in Iovembe. :Development ofthegi...e....s
*.s.w Conunittee, i,'lj {rt!+ 8th3+floor a~~~ddress
*..|+
Jeanne-Mance Building, ~ ~ ~ ~ ~.~ .............
....
manfsts as cough,..sptm .production, shortness o breath, and
wndthe P e O are el re l National
Nutrition
Month~~~~ati :. -th=2. . ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ...~.
:. and.livm . . ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~
(4"
adas: toadopt =t,.
:w
termsmokeprs. Onset ofdisease usu.a llyoccursftr.ag. 50.
f.o r .r...
...
....... .....
To motiate Ca health aighbt
Sp guiretinccreenio.nof
s h-risk patin hbestu t earl .i:~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~...........
..............................
dentification;. eal detectio smokn ct ino
(416)t outcomes.
*best
59-6867 Fr fa 46 9-54 re-almm@s.am
more
.
inati
.
. o. n c
r ..eV lop.is
ofthe guidelines
Staegie.s frw kigith .o bese pepl
AreportMedic
contact nse Man
entitled~~~~~~~~~~~
Obesity Curn tServcs by te
aemStraegis.fo.PrmaryCar populationto
aging remain self-sufficient and maintain optimum~~~~~~~~~~~~~~~~~~~~~~~~-f d...
Phyicins asbee pulihebyPgssHatcr
Intrnaionl t hep pysiiasbetter ndrtnthefcto
obesityontchealh:nto hl hmdvlpstaeist rvn haei on-erm ipcatin o urhat,exlisLs
websiteath aV/wdsitus
paiet.iD tewati aris afail
Obesit inOhei
And mt:ana ed
VOL45: FEBRUARY * FRIER 1999* Canadian Family Physician . Le Medecin defamille canadien 393Vous pouvez aussi lire

















































