Bactériémie à Staphylocoque doré: du diagnostic à la prise en charge - MERCREDI 27 JUIN 2018 MAGALI VIDAL-ROUX MALADIES INFECTIEUSES ET TROPICALES ...
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous
Bactériémie à Staphylocoque doré:
du diagnostic à la prise en charge
MERCREDI 27 JUIN 2018 MAGALI VIDAL-ROUX MALADIES INFECTIEUSES ET TROPICALES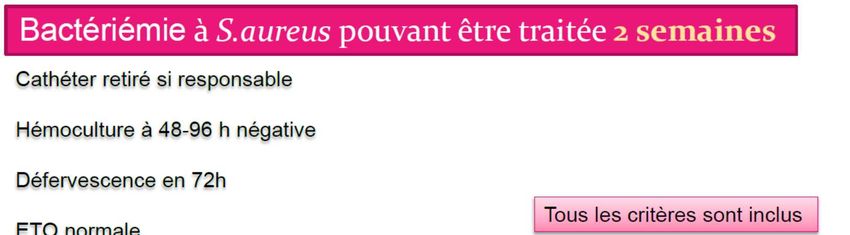
Bactériémie à Staphylococcus
aureus
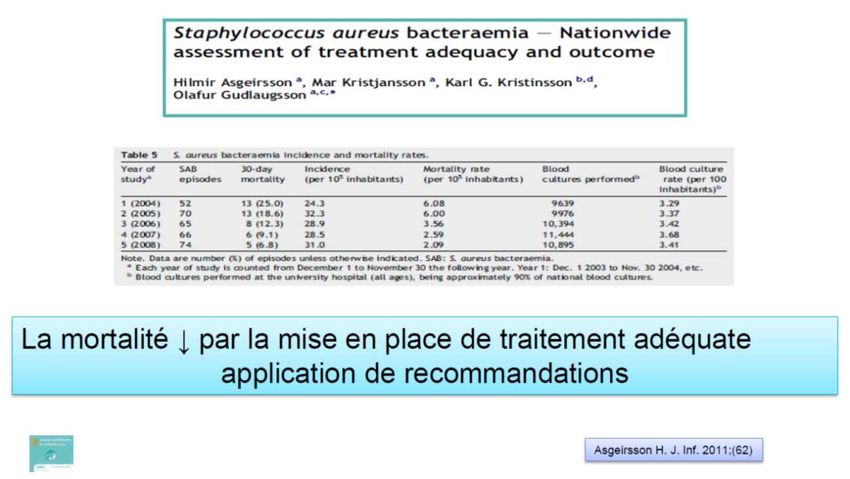
Mortalité si pas d’antibiotique: 80%
Avec antibiotiques: mortalité 15 à 40%
Staphylocoque aureus (SA) sensible à la
méticilline vs Résistant à la méticilline
Mortalité SARM > SASM (sauf pneumonies)
Comparison of mortality risk associated with bacteremia due to methicillin-resistant and methicillin-susceptible Staphylococcus aureus.
Shurland S, et al, Infect Control Hosp Epidemiol. 2007;28(3):273.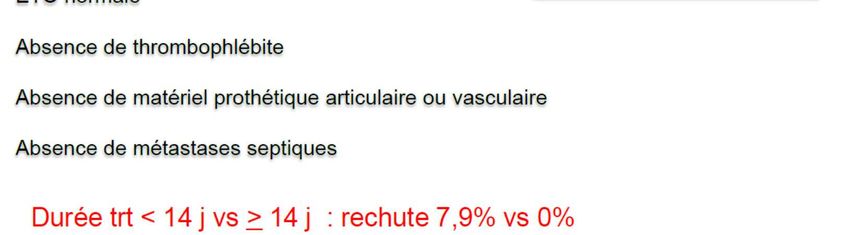
Complications des bactériémies à Staphylocoque doré o Endocardites ≈ 25-30% o Spondylodiscite/ostéomyélite/arthrites o Rein o Abcès psoas o Méninges/cerveau SASM ou SARM o Peau et tissus mous o Poumons o…. oRécidive: traitement IV 14 jours

Risque d’endocardite ETO recommandée 5 à 7 jours après le début de la bactériémie, À répéter si patient à risque d’EI (valvulopathie, bactériémie continue) ETT insuffisante mais nécessaire pour chaque bactériémie: Valvulopathie sous-jacente?
Place de l’échographie cardiaque
ETO indispensable
o Bactériémie persistante malgré antibiothérapie adequate
o “Ancienneté” de la bactériémie non connue (BSA communautaire)
o Présence de materiel intracardiaque: valves, PM..
o Valvulopathie sous-jacente
o Pas de point d’appel évident de la bactériémie (qui pourrait être
traité: abces, catheter, arthrite…..)
o Hémodialyse
o Infection du dos: Spondylodiscite, épidurite
o Présence d’emboles périphériques
o Usage de drogue intraveineuse
Use of Transthoracic Echocardiography in the Management of Low-Risk Staphylococcus aureus
Use of a simple criteria set for guiding echocardiography in nosocomial Staphylococcus aureus Bacteremia: Results From a Retrospective Multicenter Cohort Study.Showler A, Burry L, Bai AD, Steinberg
bacteremia. Kaasch AJ, Fowler VG Jr, Rieg S, Peyerl-Hoffmann G, Birkholz H, Hellmich M, Kern WV,
M, Ricciuto DR, Fernandes T, Chiu A, Raybardhan S, Science M, Fernando E, Bell CM, Morris AM JACC
Seifert H Clin Infect Dis. 2011
Cardiovasc Imaging. 2015
Place de l’échographie cardiaque
On peut se passer d’ETO si:
si:
o Bactériémie nosocomiale
o Contrôle des hémocultures stériles dans les 4 jours qui suivent le
début de l’antibiothérapie adaptée
o Pas de materiel intracardiaque: valves, PM/DAI
o Pas d’hémodialyse
o Pas de signe Clinique d’endocardite ni de localisations eptiques
secondaires
o Source de l’infection traitée dans les 72 heures ‘abcès drainé, KT
retire)
o Défervescence dans les 72 heures qui suivent la 1ère hémoculture
positive
Predicting Risk of Endocarditis Using a Clinical Tool (PREDICT): Scoring System to Guide
Low rates of endocarditis in healthcare-associated Staphylococcus aureus bacteremia suggest that
Use of Echocardiography in the Management of Staphylococcus aureus Bacteremia.
echocardiography might not always be required.Barton T, Moir S, Rehmani H, Woolley I, Korman TM,
Palraj BR, Baddour LM, Hess EP, Steckelberg JM, Wilson WR, Lahr BD, Sohail MR Clin
Stuart RL Eur J Clin Microbiol Infect Dis. 2016
Infect Dis. 2015
Clinical management of Staphylococcus aureus bacteremia: a review. Holland TL, Arnold C, Echocardiography is dispensable in uncomplicated Staphylococcus aureus bacteremia.Khatib
Fowler VG Jr JAMA. 2014 R, Sharma M Medicine (Baltimore). 2013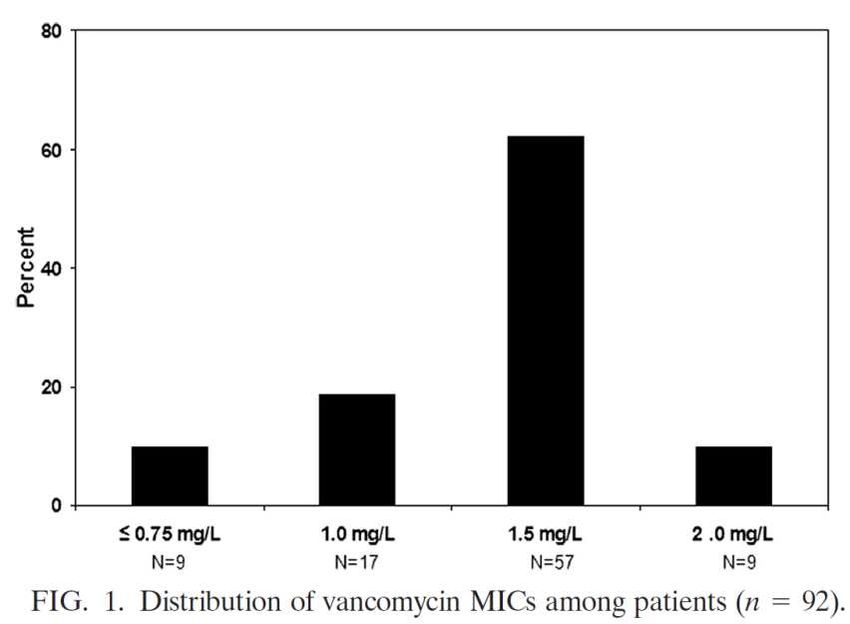
ETO et BSA nosocomiale Use of a simple criteria set for guiding echocardiography in nosocomial Staphylococcus aureus bacteremia. Kaasch AJ et al. Clin Infect Dis. 2011;53(1):1. oBactériémie prolongée >4 jours oDispositif cardiaque implantable oHémodialyse oSpondylodiscite ou infection ostéoarticulaire oSi aucun de ces critères: VPN EI 99%, pas d’ETO
Antibiothérapie SAMS ou SAMR Traitement intraveineux Durée 14 jours
Antibiothérapie: SASM Pénicilline M: Oxacilline 2 grammes toutes les 4 heures Cloxacilline 2 grammes toutes les 4 heures ou Céphalosporine de première génération: Céfazoline 2 grammes toutes les 8 heures (maximum 100 mg/kg/24h) PAS de VANCOMYCINE (sauf rares cas d’anaphylaxie à la pénicilline)
Antibiothérapie: SARM Glycopeptides Vancomycine: Dose de charge 30 mg/kg/j puis PSE 15-20 mg/kg/j (ou en discontinue) Taux résiduel vancomycine 20-30mg/l Téicoplanine 12 mg/kg /12 heures 3-5 jours puis 12 mg/kg/24h Lipopeptides Daptomycine 8-10 mg/kg/jour IV (ttes les 48h si cl
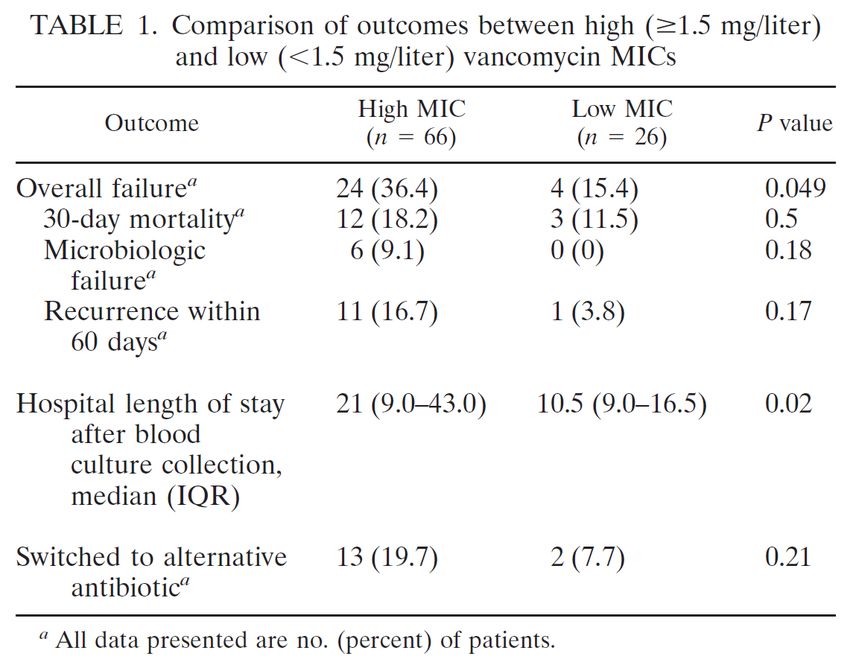
Bactériémie à SARM
Risque d’échec ou de récidive si CMI≥1,5mg/l
Relationship between vancomycin MIC and failure among patients with methicillin-resistant
Staphylococcus aureus bacteremia treated with vancomycin.
Lodise TP et al, Antimicrob Agents Chemother. 2008;52(9):3315.Traitements alternatifs
Après
Ceftaroline (Zinforo ®) antibiogramme
Linézolide (Zyvoxyd ®), bactériostatique 2nde intention
Myélotoxicité
RésistancesAntibiothérapie: SASM ou SARM Pas d’indication de bithérapie o Notamment pas d’intérêt de la RIFAMPICINE (Hors recommandations spécifiques: endocardite à SA sur prothèse valvulaire ou infection de matériel ortho/vasculaire non déposé) o Pas d’aminoside quand antibiogramme disponible
Durée de traitement:
14 jours MINIMUM
Clinical and microbiologic analysis of the risk factors for mortality in patients
Clinical management of Staphylococcus aureus bacteremia: a review. AUHolland TL,
with heterogeneous vancomycin-intermediate Staphylococcus aureus bacteremia. Chong YP, Park KH, Kim
Arnold C, Fowler VG Jr SOJAMA. 2014
ES, Kim MN, Kim SH, Lee SO, Choi SH, Jeong JY, Woo JH, Kim YS. Antimicrob Agents Chemother. 2015Durée de traitement:
14 jours MINIMUM
Clinical and microbiologic analysis of the risk factors for mortality in patients
Clinical management of Staphylococcus aureus bacteremia: a review. AUHolland TL,
with heterogeneous vancomycin-intermediate Staphylococcus aureus bacteremia. Chong YP, Park KH, Kim
Arnold C, Fowler VG Jr SOJAMA. 2014
ES, Kim MN, Kim SH, Lee SO, Choi SH, Jeong JY, Woo JH, Kim YS. Antimicrob Agents Chemother. 2015Antibiothérapie probabiliste Oxacilline +/- gentamicine Céfazoline 2gr/8 heures +/- gentamicine Vancomycine +/- gentamycine Daptomycine
Antibiothérapie: bien codifiée
“Infectious disease consultation — Bedside
infectious disease consultation is an important
component of management for patients with S.
aureus bacteremia and should occur whenever
feasible [9-17]. In one retrospective study
comparing bedside consultation with telephone
consultation for management of 342 patients with
S. aureus bacteremia, bedside consultation was
associated with a significantly lower 90-day
mortality (9 versus 29 percent; odds ratio [OR] 0.25;
95% CI 0.13-0.51) [14]. Another study noted that,
even among patients treated with an appropriate
duration of therapy, significantly fewer relapses were
observed among those who received bedside
consultation (6 versus 18 percent) [13].
Several other studies have also demonstrated that
bedside consultation by an infectious diseases
specialist is associated with better outcomes
including fewer deaths, fewer relapses, and lower
readmission rates than telephone consultation or no
consultation [12-14]. These findings underscore the
importance of serial examinations evaluating for
metastatic infection and/or clues to the source of
bacteremia.”Bactériémie à Staphylocoque: « points clés » Traitement: 14 jours en intraveineux minimum SAMS: Oxacilline ou Céfazoline SARM: Vanco ou Téicoplanine ou Daptomycine Durée totale de traitement: localisations secondaires??? Endocardite??? ETT+ examen clinique ETO Hémocultures de contrôle
Merci
Vous pouvez aussi lire

















































