Cancers du Sein Métastatiques - " Le retour gagnant des inhibiteurs de PARP " Véronique Diéras
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous
Cancers du Sein Métastatiques
« Le retour gagnant des inhibiteurs de PARP »
Véronique Diéras
Liens d’intérêt
• Les invitations à des congrès par des entreprises en lien avec
des produits de santé
– Roche, Novartis, Pfizer, GSK, EISAI, Astra Zeneca
• Les parts personnelles ou familiales dans le capital des
entreprises en lien avec des produits de santé
– Aucune
• Les rémunérations personnelles par des entreprises de produits
de santé :
• Consultant : Roche/Genentech, Novartis, Lilly, Pfizer, EISAI, NEKTAR, ABBVIE
• Intervention dans des conférences organisées par des entreprises de produits
de santé: Roche, Novartis, GSK, EISAI, Pfizer, Astra Zeneca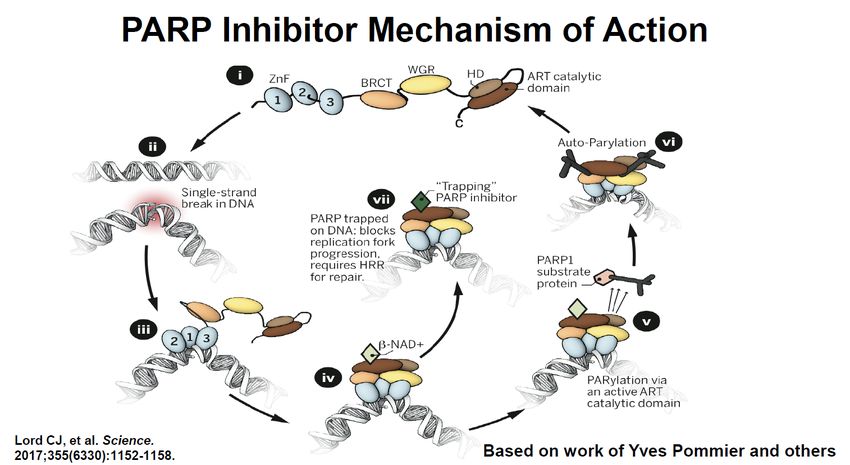
Plan • Introduction • Etudes « preuve de concept » inhibiteurs de PARP • Etudes randomisées • Perspectives • Conclusion
INTRODUCTION
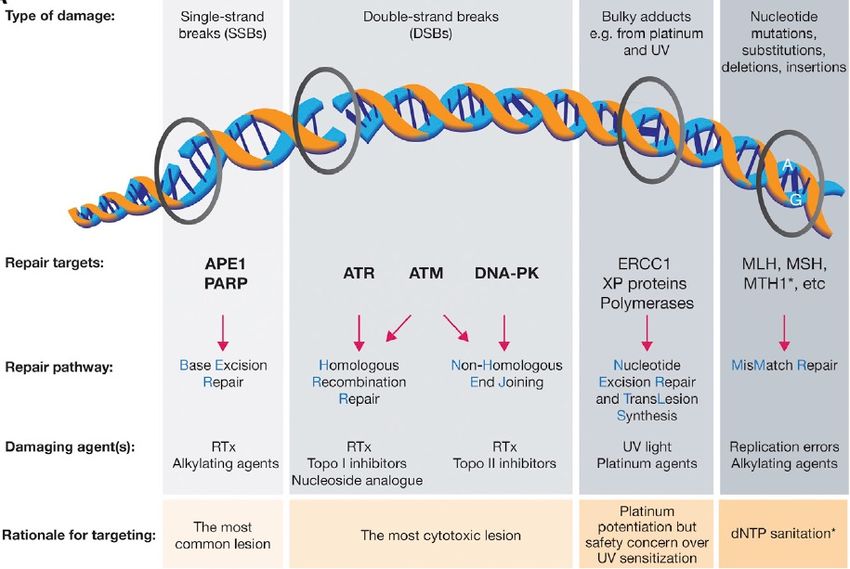
DDR Pathway and Cell Cycle targets
O’Connor, Molecular Cell, 2015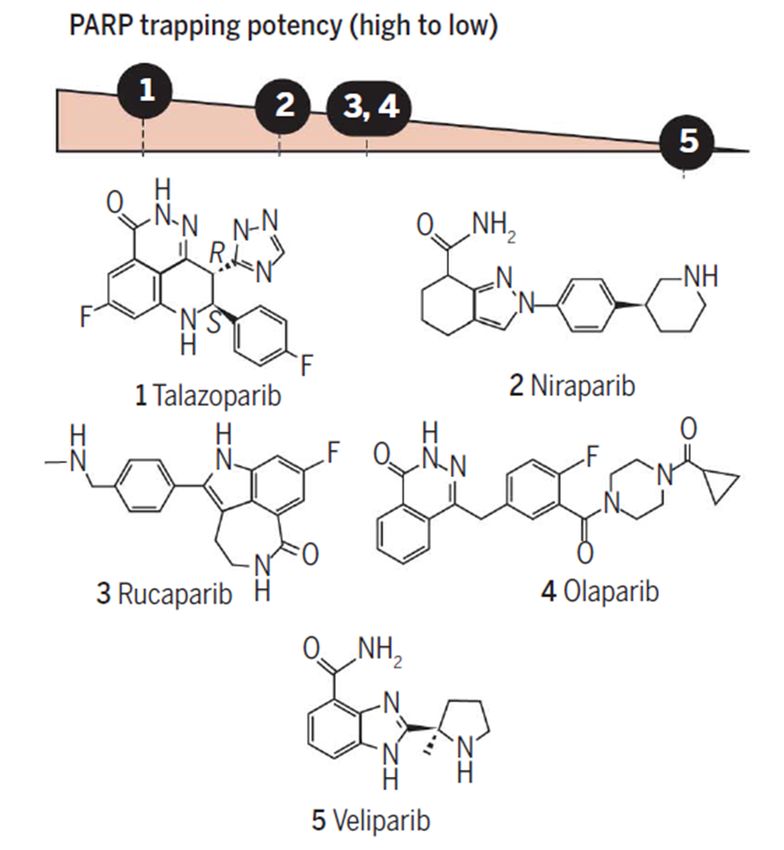
PARP inhibitors
Breast Cancer Clinical Trials
Compound Company Clinical trials BC
Olaparib Kudos / Phase III ABC (OLYMPIAD)
AZD2281 Lynparsa© AstraZeneca Phase III adjuvant (OLYMPIA)
Veliparib Abbvie Phase II randomized and III BROCADE
ABT 888 MBC BRCAm
Phase III BRIGHTNESS Neo-ADJ TNBC
Rucaparib Pfizer/ Metastatic BRCAness
AGO4699 Clovis Adjuvant TNBC + de « BRCAness »
PF036338 no germline mutation BRCA1/2
Niraparib Merck/TESARO Phase III ABC (BRAVO)
MK4827
Talazoparib Biomarin Phase III ABC (EMBRACA) phases II
BMN 673
PARP Inhibitor
Murai J, Cancer Res 2012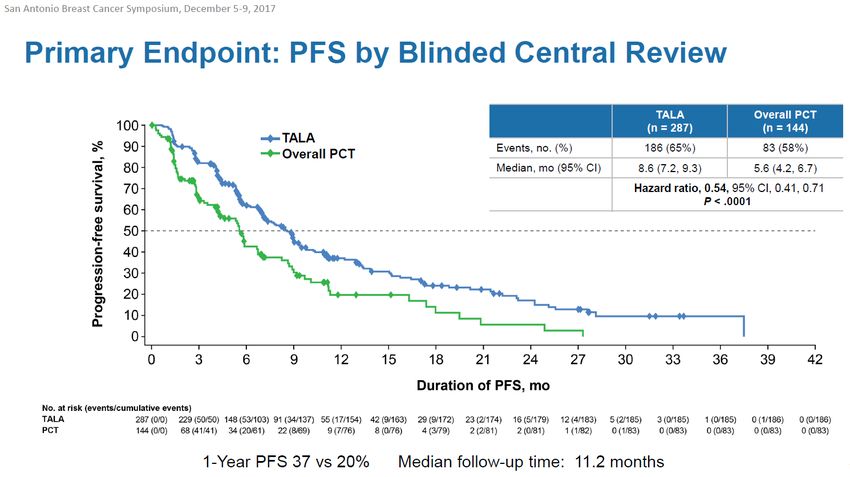
PARP inhibitors Lord CJ and Ashworth A, Science 2017
PARP inhibitors
PARP trapping
potency
Ø # Cytotoxic
effects
Ø Design of
combination
therapies
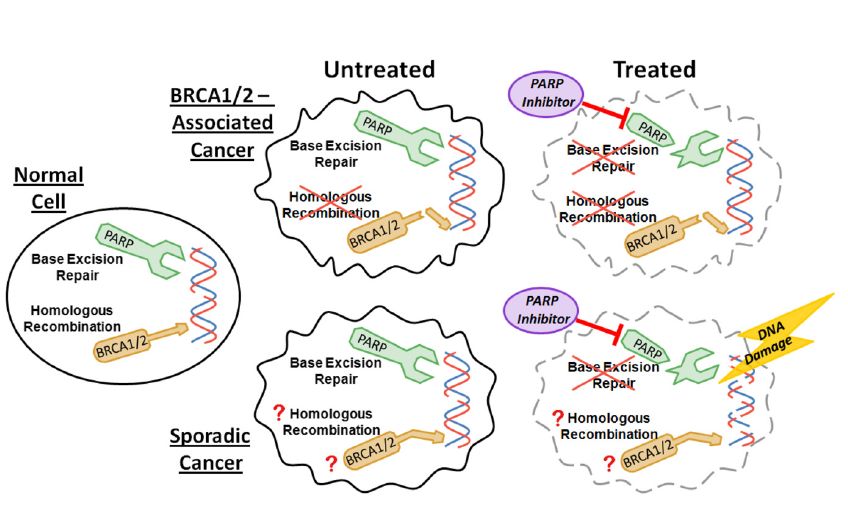
Lord CJ and Ashworth A, Science 2017PARP inhibitor treatment in BRAC1/2 associated and sporadic cancers BRACness Ellisen LW Cancer Cell 2011
Resistance to PARP inhibitors
Upregulation Restauration
PgP BRCA1/2
Loss PARP
expression Inactivation
DNA repair
proteins
Lord and Ashworth Nat Genet 2014 53BP1, REV7Resistance to PARP inhibitors
Upregulation Restauration
PgP BRCA1/2
Loss PARP
expression Inactivation
DNA repair
proteins Same as platinum
Lord and Ashworth Nat Genet 2014 53BP1, REV7 drugsETUDES « PREUVE DE CONCEPT » MONOTHERAPIE
OLAPARIB MBC
BRCA mutated
N (62) %
BRCA1 37 59.7
BRCA2 25 40.3
Prior number regimens
Mean 4,6
SD 2
N % 95%CI
OR 8 12.9 5.7-23.9
Stable disease > 8 weeks 29 47 34-59.9 Kaufman B, JCO 2015
Prior platinum salt
NO 4 20 5.7-43.7
YES 4 9.5 2.7-22.6Olaparib
Triple Negative Breast Cancer
BRCA Non BRCA Total
n=8 n= 15 n= 23
OR 0 0 0
Stable disease 5 (63%) 2 (13%) 7 (30%)
Progressive 3 (38%) 12 (80%) 15 (65%)
disease
Not evaluable 0 1 (7%) 1 (4%)
• No confirmed response to
olaparib
• Small sample size or heavily
pretreated characteristics ?
• Biology BRACness # TNBC
Gelmon K Lancet Oncol 2011NIRAPARIB
• Oral daily • Antitumor activity in BRACm
• 30mg → 400mg
tumors
• DLT thrombocytopenia
• Phase II 300mg/day • ORR 2/4 BRACm BC
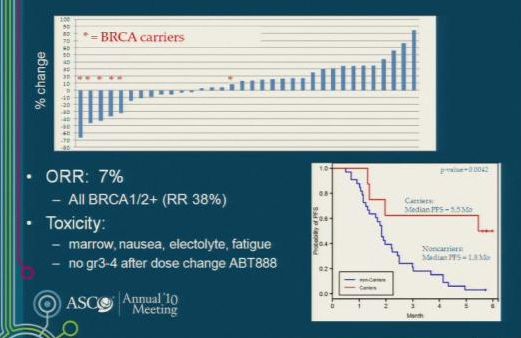
Sandhu SK Lancet Oncol 2013TALAZOPARIB
• AE: fatigue, anemia
• G3/4 anemia, thrombocytopenia
• Recommended dose 1 mg/day
• ORR 50%
• CBR 86%
• mPFS 34,6 weeks (CI95% 27.1-
54)
• Disparity BRCA1/2 ?
• BRCA2 55%
• BRCA1 38%
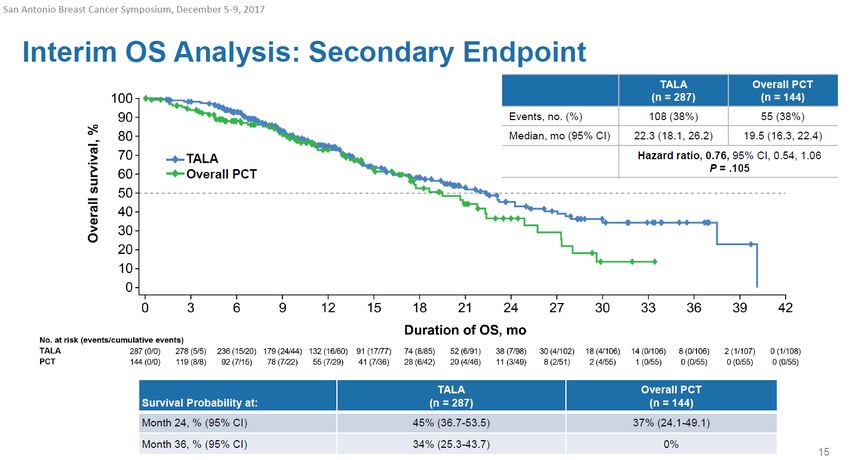
de Bono Cancer Discovery 2017TALAZOPARIB
50% response rate
Lord CJ and Ashworth A, Science 2017, de Bono Cancer Discovery 2017,
Turner ASCO 2017Cancers du sein 26
Cancers du sein métastatiques
Étude ABRAZO : phase II du talazoparib
Pourcentage maximal de changement des lésions cibles
en fonction des récepteurs hormonaux
Cohorte 1 Cohorte 2
diamètres des lésions cibles (%)
100 100
Modification de la somme des
TN (RE– et RP– et HER2–) TN (RE– et RP– et HER2–)
RH+ RE et/ou RP+ RH+ RE et/ou RP+
50 50
0 0
-30 % -30 %
-50 * * -50
*
* *
* *
-100 -100
*
Taux de RO pour les TN = 26 % * Patients en cours de traitement à la date de la fermeture
et HR+ HER2± = 29 % de la base de données le 1 er septembre 2016.
La Lettre du Cancérologue Congrès américain d’oncologie 2017 - D’après Turner NC et al., abstr. 1007, actualiséVELIPARIB Isakoff 2010
Dosing Schedules of Rucaparib
in gBRCA Mutation Carriers
No responders by ORR to rucaparib in MBC
39% SD ≥12 weeks
Schedule or differences in tumor biology or pretreatment ?
Drew Y British Journal of Cancer 2016Most common toxicities with PARPI
Clinical Hematological
• Nausea/vomiting • Neutropenia
• Fatigue • Anemia
• Anorexia • Thrombopenia
• Headache
• Diarrhea More grades 3-4:
• Constipation - Olaparib
• Dizziness
- Niraparib
• Alopecia
- Talazoparib
• DysgueusiaPARP inhibitors as single agents • Different compounds in preclinical – Catalytic / Trapping • Efficacy in mBRCA • Different pattern of toxicities • Limits: size of populations / tumoral heterogeneity : pretreatment • Head to head comparaison ????
PARP I combo with cytotoxic CT
Study Tumor type No of Investigation Results
patients
BC/total
(BRCAm BC)
Olaparib
Dent R TNBC 19/19 Olaparib 200 mg BID + ORR 37%
PTX 90mg/m²
Balmana J BC OC 42/54 (17) Olaparib 50-200 mg ORR 41%
pancreatic bid continuously vs BRCAm 71%
intermittent + CDDP Hematologic
75mg/m² toxicity
Lee J BRCAm OC 8/45 (8) Olaparib 100-400mg ORR 52%
and BC bid + CBDCA (AUC 3-5) BRCAm 88%
Veliparib
Isakoff SJ BC 41/41 (8) Veliparib 40 mg bid ORR 13%
+TMZ 150 mg/m² BRCAm50%
Somlo GJ BRCAm 26/26 Veliparib (50-200mg) ORR 46%
+PTX (80mg/m²) +
CBDCA (AUC 5-6)Conclusion PARPI combo with
cytotoxic CT
• Enhanced toxicity when combining systemic
DNA damaging agents with PARPI
– Overlapping MoA and resistance
• Less damaging agent and a PARPI / Full dose
of DNA damaging agent ??
– « High PARPI/low Chemo »
• Biomarkers
– DNA genomic
– ProteomicETUDES RANDOMISÉES
PARP inhibitors pivotal studies
Metastatic relapse
Diagnosis
Neoadjuvant Surgery Adjuvant Advanced
olaparib, olaparib niraparib,
veliparib olaparib,
veliparib,
talazoparibPARPI monotherapy vs SOC CT monotherapy
PARPI at MTD as
continuous exposure
PFS
gBRCA mutation carriers Physician’s
Anthracycline taxane R choice
resistant BC SOC
Vinorelbine
Eribulin
Niraparib BRAVO trial EORTC BIG Capecitabine
Gemcitabine
Talazoparib EMBRACA
Olaparib OLYMPIADOlympiAD Cancers du sein 21
Cancers du sein métastatiques
• CSM HER2– • Critère principal
• RO+ et/ou RP+ ou TN - SSP (RECIST 1.1,
Olaparib BICR)
• Mutation BRCA germinale
Traitement jusqu’à progression
300 mg p.o. 2 fois/j
délétère connue
ou suspectée délétère
• Traitements antérieurs par • Critères secondaires
anthracyclines et taxanes - Temps jusqu’à
• ≤ 2 lignes antérieures de CT la 2e progression
au stade métastatique
R 2:1
ou le décès
• Maladie RH+ ayant progressé - SG
sous ≥ 1 HT CT au choix de - Taux de RO
ou inéligible à une HT l’investigateur - Tolérance
• Si traitement antérieur • Capécitabine - QdV (EORTC-
à base de platine • Éribuline QLQ-C30)
- Pas de progression • Vinorelbine
au cours du traitement
adjuvant
- ≥ 12 mois entre
la dernière dose
de traitement
à base de platine
et la randomisation
CSM : cancer du sein métastatique ; BICR : revue centralisée indépendante en aveugle.
Robson M,duNEJM
La Lettre 2017
Cancérologue Congrès américain d’oncologie 2017 - D’après Robson ME et al., abstr. LBA4, actualiséOLYMPIAD
OLYMPIAD
Cancers du sein 22
Cancers du sein métastatiques
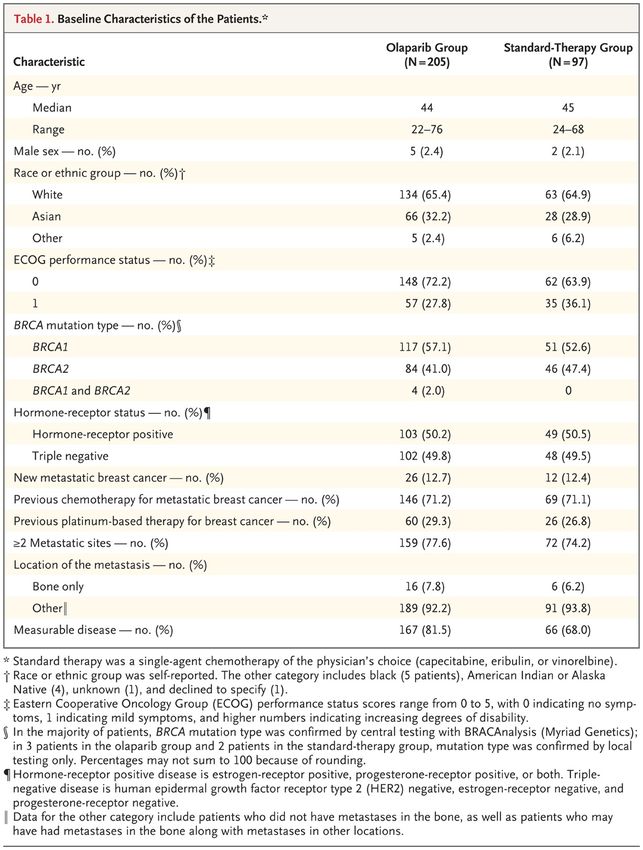
Étude OlympiAD (2)
Caractéristiques des patients
Olaparib
Chimiothérapie
300 mg p.o. 2 fois/j
(n = 97)
(n = 205)
Âge, années (médian, écart) 44 (22-76) 45 (24-68)
Hommes, n (%) 5 (2) 2 (2)
Caucasiens, n (%) 134 (65) 63 (65)
Statut BRCA, n (%)
BRCA1 117 (57) 51 (53)
BRCA2 84 (41) 46 (47)
Les 2 4 (2) 0
Statut RH, n (%)
RE+ et/ou RP+ 103 (50) 49 (51)
TN 102 (50) 48 (49)
CT antérieure au stade
146 (71) 69 (71)
métastatique, n (%)
Traitement antérieur
60 (29) 26 (27)
à base de platine, n (%)
La Lettre du Cancérologue Congrès américain d’oncologie 2017 - D’après Robson ME et al., abstr. LBA4, actualiséCancers du sein 23
Cancers du sein métastatiques
Étude OlympiAD (3)
Survie sans progression, revue centralisée indépendante en aveugle
Progression/ SSP médiane
décès, n (%) (mois)
Olaparib 300 mg x 2/j 163 (79,5) 7,0
CT 71 (73,2) 4,2
HR = 0,58 ; IC95 : 0,43-0,80 ; p = 0,0009
Patient(e)s (n)
205 177 154 107 94 69 40 23 21 11 4 3 2 1 0
97 63 44 25 21 11 8 4 4 1 1 1 1 0 0
La Lettre du Cancérologue Congrès américain d’oncologie 2017 - D’après Robson ME et al., abstr. LBA4, actualiséCancers du sein 24
Cancers du sein métastatiques
Étude OlympiAD (4)
Survie globale : analyse intermédiaire ; maturité des données : 46 %
Décès, SG médiane
n (%) (mois)
Olaparib 300 mg x 2/j 94 (45,9) 19,3
CT 46 (47,4) 19,6
HR = 0,90 ; IC95 : 0,63-1,29 ; p = 0,5665
Patient(e)s (n)
205 205 199 189 178 159 146 109 78 46 30 18 14 8 4 0
97 92 85 78 74 69 62 50 34 24 13 9 7 4 2 0
La Lettre du Cancérologue Congrès américain d’oncologie 2017 - D’après Robson ME et al., abstr. LBA4, actualiséCancers du sein
OLYMPIAD Tolérance Cancers du sein métastatiques
25
Effets indésirables (tous grades) ≥ 15 % des patients
Nausées 58 35
Anémie 40 26
Vomissement 30 15
Fatigue 29 23
Neutropénie 27 50
Diarrhée 21 22
Céphalées 20 15
Toux 17 7
Diminution des globules blancs 16 21
Perte d’appétit 16 12
Pyrexie 14 18
Augmentation des ALT 11 18 Olaparib 300 mg 2 fois/j
(n = 205)
Augmentation des AST 9 17
CT
Syndrome mains-pieds 1 21 (n = 91)
75 50 25 0 25 50 75
Effets indésirables (%)
La Lettre du Cancérologue Congrès américain d’oncologie 2017 - D’après Robson ME et al., abstr. LBA4, actualiséPhase III : Questions
• Biomarqueurs de réponse
– Mécanismes de
résistance/mutations
– ctDNA
• Comparaison en 1° ligne?
– Anthracyclines, taxanes, platines
• Bénéfice en survie?
• Quid des autres PARPis ?
– PARP trappingPARPI monotherapy vs SOC CT monotherapy • Exclusion criteria: resistance to platinum salts • No Platinum salt in control arm (SOC)… • No stratification according BRAC mutation • OLYMPIAD and EMBRACA improve PFS • Others phase III BRAVO • Other strategies as maintenance therapy ?
PARPI in combination with CT vs SOC CT Primary endpoint: PFS Secondary endpoints OS, CBR, ORR, Safety and tolerability Han, Dieras, Annals Oncology 2017
PARPI in combination with CT vs SOC CT
BROCADE 2
Han, Dieras, Annals Oncology 2017PARPI in combination with CT vs SOC CT: BROCADE 2
Comparable safety profile
Han, Dieras, Annals Oncology 2017VELIPARIB TEMOZOLOMIDE
Han, Dieras, Annals Oncology 2017PERSPECTIVES
Adaptative Randomization of Veliparib-Carboplatin Treatment
in Breast Cancer
Neo-adjuvant setting
TNBC
Rugo HS N Eng J Med 2016DNA Repair Pathways
Ding J, Trends in Pharmacological
Sciences 2006DNA Repair Pathways
Targets under investigation
NU7441
AMA37
IC60211
ATMi IC86621
KU 55933
O-BG CP 466722
Patri ATRi
n SC202994
NU6027
Rucaparib AZ20 MP470
Methoxyan Olaparib VE821
ine KA A
Veliparib
Niraparib
Stimasterol
(TRC102) talazopari
CRT Oleanolic
b
0044876 acid
Ding J, Trends in Pharmacological
AR03 Edgeworin
Sciences 2006
BetulinicPARP Targeted combinations
currently in clinical trials
• + Immune check point inhibitors
– Higher mutagenic load
• + VEGF/R inhibitors
– bevacizumab, cedinarib
• + DNA damage response inhibitors
– ATR inhibitor
> 70 clinical trials: clinicaltrials.govBiomarkers of PARP inhibitor sensitivity
Single gene biomarkers BRCAness
• BRCA1/2 sporadic mutation • Gene expression signatures
• BRAC1 promoter methylation • Genomic instability
• PTEN deficiency • Complex mutations (TP53)
• ATM mutation • Genomic « scar » of HR
• MRE11 dominant negative deficiency
mutations
• FANCF promoter
methylation….
• PARP1 levels ?
• PAR polymer levels…
• SLFN11 Complexicity added with
combinations
Turner N, Aschworth A BCRT 2011CONCLUSION
Evidence available • DNA damage/repair pathways
Evidence available • DNA damage/repair pathways • Concept synthetic lethality
Evidence available • DNA damage/repair pathways • Concept synthetic lethality • BRAC1 / BRCA2 mutation
Evidence available
• DNA damage/repair pathways
• Concept synthetic lethality
• BRAC1 / BRCA2 mutation
• Acquired loss of BRCA1 function/defects in
HRR other than BRCA 1 / 2Evidence available
• DNA damage/repair pathways
• Concept synthetic lethality
• BRAC1 / BRCA2 mutation
• Acquired loss of BRCA1 function/defects in
HRR other than BRCA 1 / 2
• Prolongation PFS in clinical trials with PARP
inhibition
– OLYMPIAD / EMBRACAUnsolved problems • Early stages – BRIGHTNESS – OLYMPIA
Unsolved problems • Early stages • Best agent in each clinical context
Unsolved problems • Early stages • Best agent in each clinical context • Long term side effects
Unsolved problems • Early stages • Best agent in each clinical context • Long term side effects • OS prolongation
Unsolved problems • Early stages • Best agent in each clinical context • Long term side effects • OS prolongation • Combination therapies
Unsolved problems
• Early stages
• Best agent in each clinical context
• Long term side effects
• OS prolongation
• Combination therapies
• New treatment targets for HRR-proficient
casesUnsolved problems • Early stages • Best agent in each clinical context • Long term side effects • OS prolongation • Combination therapies • New treatment targets for HRR-proficient cases • Mechanisms of clinical resistance
Unsolved problems • Early stages • Best agent in each clinical context • Long term side effects • OS prolongation • Combination therapies • New treatment targets for HRR-proficient cases • Mechanisms of clinical resistance • Predictive biomarkers
Unsolved problems • Early stages • Best agent in each clinical context • Long term side effects • OS prolongation • Combination therapies • New treatment targets for HRR-proficient cases • Mechanisms of clinical resistance • Predictive biomarkers
MERCI DE VOTRE ATTENTION
Vous pouvez aussi lire