Exploration de l'insuffisance valvulaire aortique en IRM: place par rapport à l'échographie - JM Serfaty, K. Warin Fresse Service d'imagerie ...
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous
Exploration de l’insuffisance
valvulaire aortique en IRM: place
par rapport à l’échographie
JM Serfaty, K. Warin Fresse
Service d’imagerie cardiaque et vasculaire
diagnostique
CHU Nantes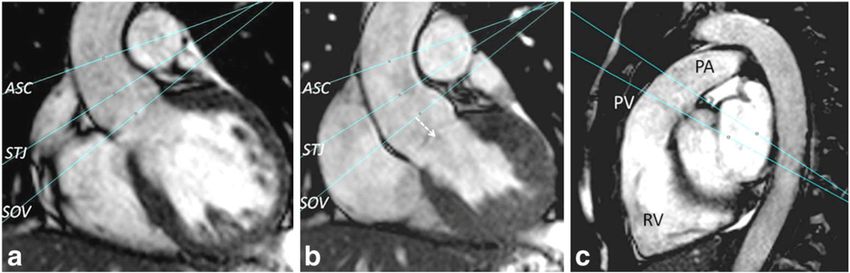
Physiopathologie • Dilatation racine de l’aorte non coaptation des valves – Marfan et appariés – Bicuspidie – Dilatation idiopathique – Dissection – Aortites • Maladie des valves – Calcifications séniles – Bicuspidie (prolapsus valve fusionnée) – Endocardite – RAA +- prolapsus associé des valves
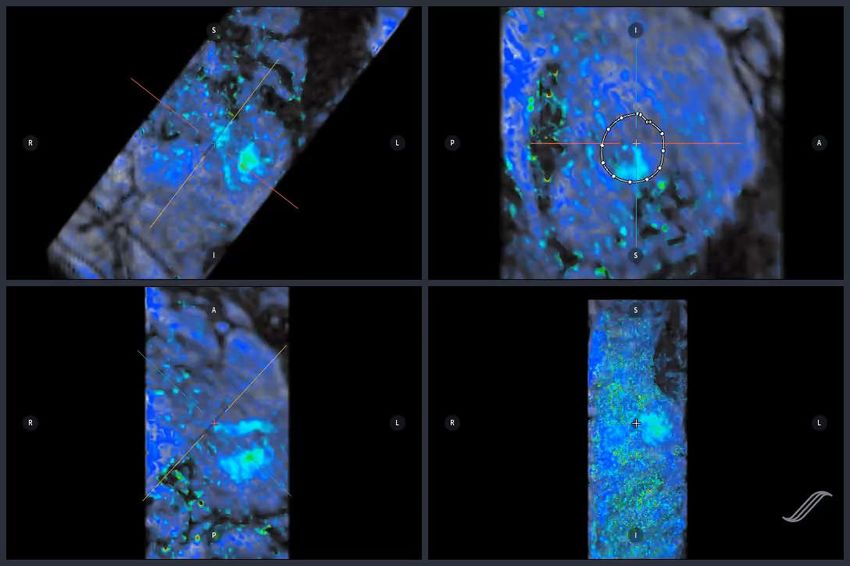
Figure 35.2.1 Definition of aortic root and ascending aortic phenotypes and mechanisms of aortic regurgitation (AR) (echocardiographic
view) and direction of the regurgitant jet (Doppler view).
Chapter: Aor c regurgita on Author(s): Pilar Tornos Mas and Emmanuel Lansac From: ESC CardioMed (DRAFT)
Downloaded from Oxford Medicine Online. © Oxford University Press, 2018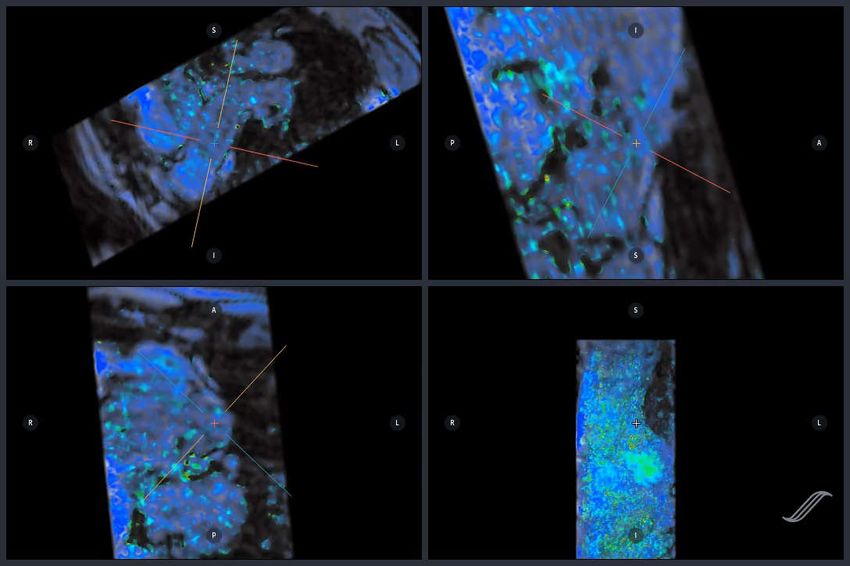
Management of aortic
regurgitation
Groupe 1
AORTIQUE
Chapter: Aor c regurgita on Author(s): Pilar Tornos Mas and Emmanuel Lansac From: ESC CardioMed (DRAFT)
Downloaded from Oxford Medicine Online. © Oxford University Press, 2018
Management of aortic
regurgitation
Groupe 2
NON AORTIQUE
FUITE SEVERE
symptomatique
Chapter: Aor c regurgita on Author(s): Pilar Tornos Mas and Emmanuel Lansac From: ESC CardioMed (DRAFT)
Downloaded from Oxford Medicine Online. © Oxford University Press, 2018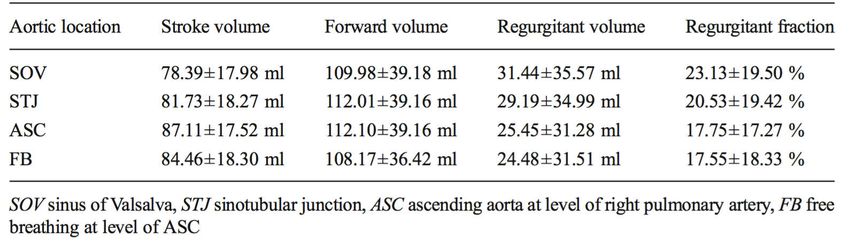
Management of aortic
regurgitation
Groupe 2
NON AORTIQUE
FUITE SEVERE
Asymptomatique
FEVG < 50% ou
Volumes VG augmentés
Chapter: Aor c regurgita on Author(s): Pilar Tornos Mas and Emmanuel Lansac From: ESC CardioMed (DRAFT)
Downloaded from Oxford Medicine Online. © Oxford University Press, 2018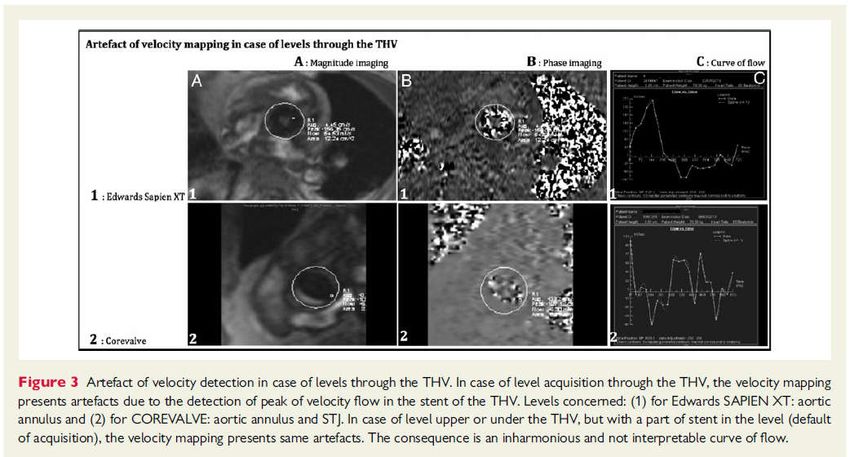
Groupe 1 : AORTIQUE
Marfan sans FDR > 50mm chirurgie INDIQUEE
ESC 2017
Groupe 1 : AORTIQUE
Marfan + FDR, ou mutation TGFBR1-R2 > 45mm
Bicuspidie + FDR ou Coarctation > 50mm chirurgie CONSIDEREE
Tout patient >55mm
FDR: histoire familiale, HTA, >3mm/an
ESC 2017
Groupe 1 : AORTIQUE
Réparation valvulaire si : patient jeune + dilatation aortique + valve tricuspide
ESC 2017
Groupe 2 : NON AORTIQUE, fuite SEVERE
ESC 2017Sinus de Valsava
Sinus de Valsava Prolapsus valve aortique Prolapsus valve aortique
Figure 35.2.1 Definition of aortic root and ascending aortic phenotypes and mechanisms of aortic regurgitation (AR) (echocardiographic
view) and direction of the regurgitant jet (Doppler view).
Chapter: Aor c regurgita on Author(s): Pilar Tornos Mas and Emmanuel Lansac From: ESC CardioMed (DRAFT)
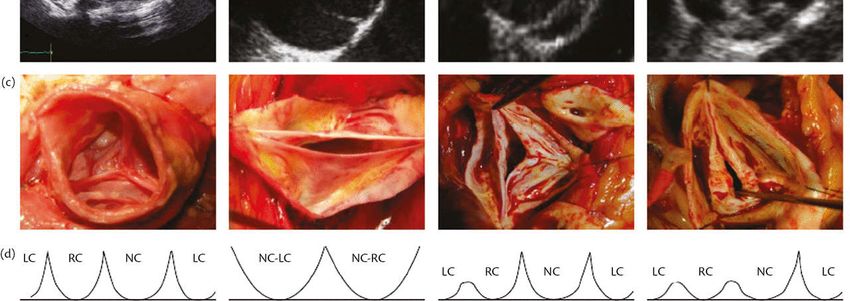
Downloaded from Oxford Medicine Online. © Oxford University Press, 2018Figure 35.2.2 Classification of aortic valve pathology: tricuspid, bicuspid (0 or 1 raphes), and unicuspid. (a) Diagram. (b) Echocardiographic
views. (c) Pathology specimens. (d) LC, left coronary; NC, non-coronary; RC, right coronary.
ETT
Se: 56%
Sp : 86%
Chapter: Aor c regurgita on Author(s): Pilar Tornos Mas and Emmanuel Lansac From: ESC CardioMed (DRAFT)
Downloaded from Oxford Medicine Online. © Oxford University Press, 2018Figure 35.2.4 Definition of coaptation height (cH) and effective height (eH) of aortic valve cusps. STJ,
sinotubular junction.
eH: effective height
Chapter: Aor c regurgita on Author(s): Pilar Tornos Mas and Emmanuel Lansac From: ESC CardioMed (DRAFT)
Downloaded from Oxford Medicine Online. © Oxford University Press, 2018AORTE ASCENDANTE IRM sans injection Scanner injecté synchronisé Bicuspidie type 1
QUANTIFICATION DE LA FUITE (valve NATIVE)
Utile si discordance entre clinique et mesures écho
La mesure IRM de la fuite est moins variable que l’ETT et ETO
Précis pour :
Quantification de la fuite
Volume VG
FEVG
AHA Guidelines 2014Circ Cardiovasc Imaging. 2013;6:48-57
ECHOGRAPHIE IRM
Circ Cardiovasc Imaging. 2013;6:48-57Recommendation : Mesure sur la JST Le mieux corrélé à Stroke VG - VD Eur Radiol 2015
Comparaison de
reflux turbulents à
des méthodes
indépendantes de
ces turbulences
TE non précisé
Recommandé :
Stroke Ao – Stroke APulm
Pediatric Radiol 2014CIRC 2012
Seuil: Fraction Régurgitation > 33 %
Seuil : Vol VG TD : > 246ml2015
ETT: faible (73%), modérée (10%), sévère (16%)
Un jet régurgitant (33%), 2 jets (60%), 3 jets (7%)
Pas de jet central
7% des patients avaient une fenêtre acoustique limitée
2015 Meilleure mesure : coupe au dessus de la prothèse
Vérifier que le volume éjecté aortique = VE VG, l’absence d’artefact de flux, et
une courbe harmonieuse
2015> 14% Fuite modérée ou sévère
Kappa = 0.33
Pour les Fuite modérées :
ETT sous-estime / IRM
IRM
ECHOMortalité supérieure si fuite post-TAVR 135 patients after TAVR 3 centres Mesure fraction de régurgitation 40 jours après TAVR vs Echo 6 jours post TAVR Suivi 2 ans Endpoint : Mortalité, Rehospitalisation
COPD : BPCO
IRM Echographie Mortalité Mortalité Rehospitalisation Rehospitalisation
• Limites:
– Pas d’écho 3D
– Différence de timing entre ETT et IRM
• IRM vs Echo
– Mesure quantitative vs semi- en écho, dédié à la valve native (fuites
post-TAVI para-valvulaires excentrées)
– Mesure reproductible > echo
– Patients peu échogènes
– Peu gêné par les jets excentrés > echo
– Pas de sous-estimation des fuites aortiques > echo• Indications
– Patients peu échogènes
– ETT et/ou ETO douteuses
– Fuite faible à modérée à l’ETT avec symptômes ou signes
d’insuffisance cardiaque
– Fuite modérée à sévère à l’ETT
• Intérêt du suivi par IRM : quantification de la fuite et
du volume VG
• Décision de gestes complémentaireIRM 3T, 4D flow
Post injection bolus
Arterys
Critères diagnostiques :
•Diamètre jet / Ch chasse VG : 65%
•Longueur jet / longueur VG : 50%
•Jet régurgitant dans l’aorte descendante : non / traces / oui
K=0,88Courtoisie Benjamin Dubourg
Logiciel : Arterys
Courtesie : Elie MousseauCONCLUSION • Patient avec valve native – Anatomie de l’aorte – Sévérité de la régurgitation – Fraction d’éjection et volume VG • Patient avec valve post-TAVR – Sévérité de la fuite • Technique – 4D flow
Vous pouvez aussi lire

















































