LE SYNDROME DU CANAL CARPIEN - INTRODUCTION TRAITEMENT CHIRURGICAL PAR VOIE ENDOSCOPIQUE
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous
LE SYNDROME DU
CANAL CARPIEN
TRAITEMENT CHIRURGICAL PAR VOIE
ENDOSCOPIQUE
Dr O. DELAERE
Avril 2019
INTRODUCTION
1
HISTORIQUE
PAGET J. Lectures on surgical pathology.
Philadelphia: Lindsay & Blakiston; 1854
« the median nerve, where it passes under the
annular ligament, is enlarged with adhesions to
all the adjacent tissues, and induration of both it
and them »
2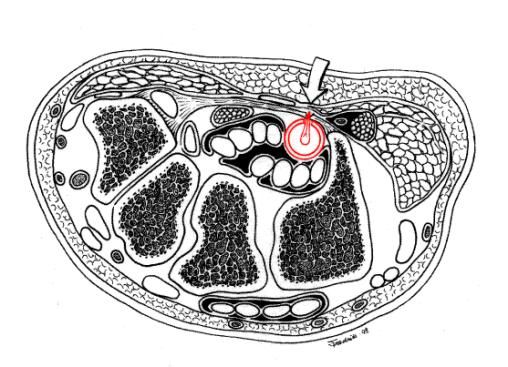
PUTNAM J.J. A series of cases of paresthesias,
mainly of the hand, or periodic recurrence, and possibly
of vaso-motor origin. Arch. Med. 1880; 4:147-62.
« Common symptom of recurrent nocturnal or
morning numbness affecting one or both hands, in
which the numbness could become so intense that
the sensation would progress to pain… »
Traitements historiques :
3
Traitements historiques :
. Amputation du bras
Traitements historiques :
. Amputation du bras
. Galvanisme
4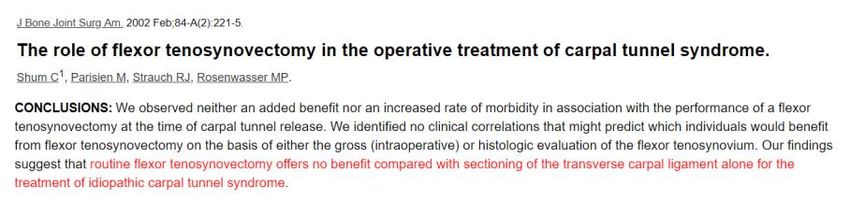
Traitements historiques :
. Amputation du bras
. Galvanisme
. Strychnine
Traitements historiques :
. Amputation du bras
. Galvanisme
. Strychnine
. Cannabis
5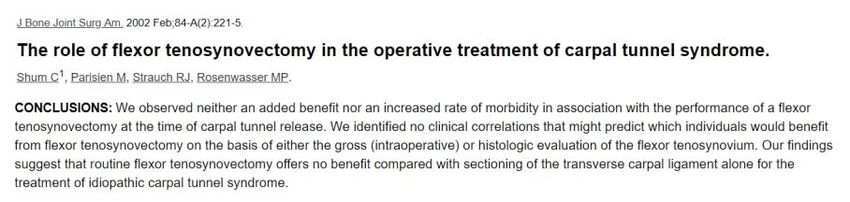
Traitements historiques :
. Résection de la première côte
Traitement le plus populaire durant les
quarante premières années du 20ème siècle !
MARIE P., FOIX C. Atrophie isolée de
l’éminence thénar d’origine névritique : rôle du ligament
annulaire antérieur du carpe dans la pathogénie de la
lésion. Rev. Neurol. 1913; 26 : 647-9.
6
MARIE P., FOIX C. Atrophie isolée de
l’éminence thénar d’origine névritique : rôle du ligament
annulaire antérieur du carpe dans la pathogénie de la
lésion. Rev. Neurol. 1913; 26 : 647-9.
« …proximal to the annular ligament a nodular
thickening is present which looks and feels like a
neuroma. Underlying the annular ligament,
however, the nerve suddenly becomes thin… »
MARIE P., FOIX C. Atrophie isolée de
l’éminence thénar d’origine névritique : rôle du ligament
annulaire antérieur du carpe dans la pathogénie de la
lésion. Rev. Neurol. 1913; 26 : 647-9.
« …Myelin sheets are progressively diminished…
and at the constriction they are nearly
completely absent… »
« …transsection of the ligament could stop the
development of these phenomena… »
7
LEARMONTH J.R. The principle of
decompression in the treatment of certain diseases of
peripheral nerves. Surg. Clin. North Am.1933;13:905-
13.
Lésions post-traumatiques
8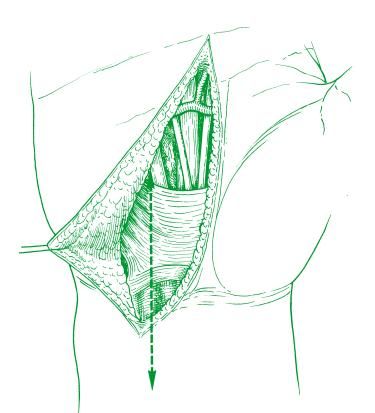
PHALEN G.S. Spontaneous compression of the
median nerve at the wrist. JAMA 1951;145:1128-32.
PHALEN G.S. Spontaneous compression of the
median nerve at the wrist. JAMA 1951;145:1128-32.
.Examen clinique : signe de TINEL
9
PHALEN G.S. Spontaneous compression of the
median nerve at the wrist. JAMA 1951;145:1128-32.
.Examen clinique : signe de TINEL
.Examen clinique : signe de PHALEN
PHALEN G.S. Spontaneous compression of the
median nerve at the wrist. JAMA 1951;145:1128-32.
.Examen clinique : signe de TINEL
.Examen clinique : signe de PHALEN
.Etiologie : hypertrophie synoviale des
fléchisseurs
10PHALEN G.S. Spontaneous compression of the
median nerve at the wrist. JAMA 1951;145:1128-32.
.Examen clinique : signe de TINEL
.Examen clinique : signe de PHALEN
.Etiologie : hypertrophie synoviale des
fléchisseurs
.Traitement alternatif : attelle
d’immobilisation
PHALEN G.S. Spontaneous compression of the
median nerve at the wrist. JAMA 1951;145:1128-32.
.Examen clinique : signe de TINEL
.Examen clinique : signe de PHALEN
.Etiologie : hypertrophie synoviale des
fléchisseurs
.Traitement alternatif : attelle
d’immobilisation
.Traitement alternatif : injection d’un
corticoïde
11INCIDENCE ET PREVALENCE
INCIDENCE ET PREVALENCE
90% de tous les syndromes canalaires
12INCIDENCE ET PREVALENCE
90% de tous les syndromes canalaires
10% de risque d’attraper la maladie dans sa vie
INCIDENCE ET PREVALENCE
90% de tous les syndromes canalaires
10% de risque d’attraper la maladie dans sa vie
PREVALENCE SIMILAIRE CHEZ L’HOMME ET CHEZ LA FEMME SOUS LES 60 ANS
(Etudes randomisées)
13INCIDENCE ET PREVALENCE
90% de tous les syndromes canalaires
10% de risque d’attraper la maladie dans sa vie
PREVALENCE SIMILAIRE CHEZ L’HOMME ET CHEZ LA FEMME SOUS LES 60 ANS
(Etudes randomisées)
RATIO AUGMENTE JUSQU’À 4 F / 1H APRES 65 ANS
ETIOLOGIE DU S.C.C.
14ETIOLOGIE DU S.C.C.
FORME LA PLUS COMMUNE = IDIOPATHIQUE
ETIOLOGIE DU S.C.C.
FORME LA PLUS COMMUNE = IDIOPATHIQUE
PHYSIOPATHOLOGIE ENCORE LARGEMENT INCOMPRISE !
15ETIOLOGIE DU S.C.C.
FORME LA PLUS COMMUNE = IDIOPATHIQUE
PHYSIOPATHOLOGIE ENCORE LARGEMENT INCOMPRISE !
PROCESSUS ESSENTIELLEMENT NON-INFLAMMATOIRE A L’ANA-PATH
(épaississement et fibrose synoviale, prolifération vasculaire, hyperplasie
intimale, modifications du collagène)
16ETIOLOGIE DU S.C.C.
FORMES SECONDAIRES : ANOMALIES DU CONTENANT
Fractures du radius distal ou traumatismes du carpe
Arthrose ou arthrite du poignet
Rhizarthrose
Acromégalie
17ETIOLOGIE DU S.C.C.
FORMES SECONDAIRES : ANOMALIES DU CONTENU
Ténosynovites inflammatoires : lupus, P.R.
Ténosynovites métaboliques : amyloïdose, Diabète I et II, goutte,
chondrocalcinose
Oedème interstitiel : grossesse, hypothyroïdie, insuffisance rénale
(fistules a/v)
Anomalies musculaires : muscles surnuméraires, d’insertion trop
proximale (lombricaux) ou trop distale (FSD)
Processus expansifs intra-canalaires (kystes, tumeurs…)
Obésité
ETIOLOGIE DU S.C.C.
MALADIE
PROFESSIONNELLE ?
18 There is support for substantially more than a doubling of risk when
repetitive wrist movements (repeated palmar flexion and extension of the
wrist) occupy a major part of the working day…
Forceful gripping can also more than double the risk of CTS
There is support for substantially more than a doubling of risk when
repetitive wrist movements (repeated palmar flexion and extension of the
wrist) occupy a major part of the working day…
Forceful gripping can also more than double the risk of CTS
19 There is support for substantially more than a doubling of risk when
repetitive wrist movements (repeated palmar flexion and extension of the
wrist) occupy a major part of the working day…
Forceful gripping can also more than double the risk of CTS
20 PHENOMENES DE RAYNAUD MULTIPLIES PAR 6,9 (Indice de fiabilité élevé)
PHENOMENES DE RAYNAUD MULTIPLIES PAR 6,9 (Indice de fiabilité élevé)
S.C.C. MULTIPLIE PAR 2,9 (indice de fiabilité + faible)
21 Excessive computer use, particularly mouse usage might be a minor
occupational risk factor for CTS
Excessive computer use, particularly mouse usage might be a minor
occupational risk factor for CTS
22DIAGNOSTIC
. ANAMNESE (Paresthésies nocturnes)
. EXAMEN CLINIQUE (Tinel, Phalen, Compression test…)
DIAGNOSTIC
. ANAMNESE (Paresthésies nocturnes)
. EXAMEN CLINIQUE (Tinel, Phalen, Compresion test…)
SENSIBILITE ET SPECIFICITE
DE 80 à 90% DANS LE DIAGNOSTIC DU S.C.C
23DIAGNOSTIC
. EXAMENS COMPLEMENTAIRES…
E.M.G.
24E.M.G.
SENSIBILITE / SPECIFICITE entre 80 et 90%
E.M.G.
SENSIBILITE / SPECIFICITE entre 80 et 90%
FAUX POSITIFS ET FAUX NEGATIFS (16 à 34%)
25E.M.G.
SENSIBILITE / SPECIFICITE entre 80 et 90%
FAUX POSITIFS ET FAUX NEGATIFS (16 à 34%)
E.M.G. A L’AIGUILLE : PERMET SURTOUT D’EXCLURE D’AUTRES ETIOLOGIES
(RADICULOPATHIE CERVICALE)
E.M.G.
SENSIBILITE / SPECIFICITE entre 80 et 90%
FAUX POSITIFS ET FAUX NEGATIFS (16 à 34%)
E.M.G. A L’AIGUILLE : PERMET SURTOUT D’EXCLURE D’AUTRES ETIOLOGIES
(RADICULOPATHIE CERVICALE)
V.C.S INFERIEURES A 40 M/S ET L.D.M. SUPERIEURES A 4,4 ms EVOCATRICES D’UNE
INDICATION CHIRURGICALE
26E.M.G.
SENSIBILITE / SPECIFICITE entre 80 et 90%
FAUX POSITIFS ET FAUX NEGATIFS (16 à 34%)
E.M.G. A L’AIGUILLE : PERMET SURTOUT D’EXCLURE D’AUTRES ETIOLOGIES
(RADICULOPATHIE CERVICALE)
V.C.S INFERIEURES A 40 M/S ET L.D.M. SUPERIEURES A 4,4 ms EVOCATRICES D’UNE
INDICATION CHIRURGICALE
LA L.D.M. EST LA VALEUR LA PLUS SUSCEPTIBLE DE REVENIR A LA NORMALE
EN POST-OP
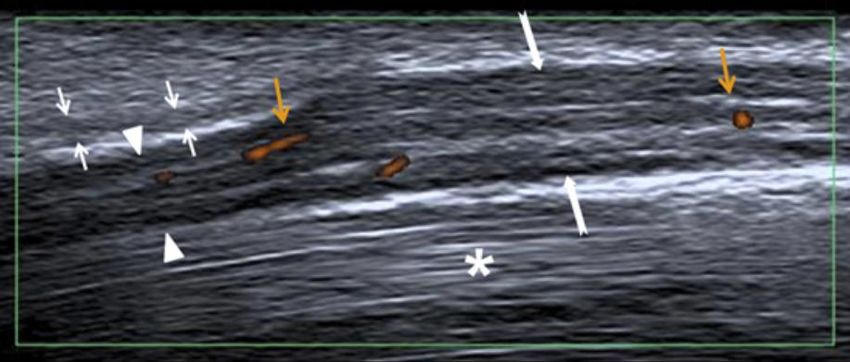
Echographie
Elargissement du nerf médian en
amont du rétinaculum des
fléchisseurs Calibre >12 mm2 : +/- 80% de
sensibilité/spécificité pour le
diagnostic d’un S.C.C.
Amincissement du nerf médian
sous le rétinaculum des
fléchisseurs
Hyperémie intraneurale
Epaississement du rétinaculum
Meyer P, Lintingre P-F, Pesquer L, Poussange N, Silvestre A, Dallaudière B. The Median
des fléchisseurs Nerve at the Carpal Tunnel … and Elsewhere. Journal of the Belgian Society of Radiology.
2018;102(1):17. DOI: http://doi.org/10.5334/jbsr.1354
27 Our study demonstrates that there are differences in the sensitivity and
specificity profiles of NCS and US, which may beneficially complement one
another when used together
Our study demonstrates that there are differences in the sensitivity and
specificity profiles of NCS and US, which may beneficially complement one
another when used together
28 CT SCAN, IRM…
Processus expansifs intra-
canalaires
Meyer P, Lintingre P-F, Pesquer L, Poussange N,
Silvestre A, Dallaudière B. The Median Nerve at
the Carpal Tunnel … and Elsewhere. Journal of
the Belgian Society of Radiology.
2018;102(1):17. DOI:
http://doi.org/10.5334/jbsr.1354
Kyste synovial
Lipome
Classification selon les
symptômes et la clinique
29Classification selon les
symptômes et la clinique
Mild CTS
Nocturnal paresthesias
Swelling and pain relieved by shaking hand or changing hand position
Classification selon les
symptômes et la clinique
Mild CTS
Nocturnal paresthesias
Swelling and pain relieved by shaking hand or changing hand position
Moderate CTS
Symptoms persist during the day
Decreasing sensation results in finger clumsiness
30Classification selon les
symptômes et la clinique
Mild CTS
Nocturnal paresthesias
Swelling and pain relieved by shaking hand or changing hand position
Moderate CTS
Symptoms persist during the day
Decreasing sensation results in finger clumsiness
Severe CTS
Numbness without pain
Atrophy of the thenar eminence may occur
Mild CTS
Nocturnal paresthesias
Swelling and pain relieved by shaking hand
or changing hand position
Altérations métaboliques
rapidement réversibles
.Congestion veineuse
.Oedème intrafasciculaire
.Hypoxie
31 Moderate CTS Démyélinisation
Symptoms persist during the (Sensitive, puis
day motrice)
Decreasing sensation results in
finger clumsiness
sensation results in finger
Altérations
clumsiness structurelles
plus lentement réversibles
EMG :
.LDM
.VC
Severe CTS Dégénérescence
Numbness without pain axonale
Atrophy of the thenar
eminence may occur
of the thenar eminence may occur
Altérations structurelles
partiellement
irréversibles
EMG :
.LDM
.VC
.Perte amplitude
32TRAITEMENT
. ATTELLE DE POIGNET
. INFILTRATION
. CHIRURGIE
33TRAITEMENT CHIRURGICAL
34TRAITEMENT CHIRURGICAL
O.C.T.R.
TRAITEMENT CHIRURGICAL
Utilité des
Gestes associés ?
35EPINEUROTOMIE ?
EPINEUROTOMIE ?
36SYNOVECTOMIE DES FLECHISSEURS ?
SYNOVECTOMIE DES FLECHISSEURS ?
37CHIRURGIE MINI-INVASIVE
CHIRURGIE MINI-INVASIVE
Limitation des inconvénients post-
opératoires
Douleurs cicatricielles
Perte de force
Délais d’incapacité de travail
38CHIRURGIE ENDOSCOPIQUE
CHIRURGIE ENDOSCOPIQUE
OKUTSU 1987
39CHIRURGIE ENDOSCOPIQUE
CHOW 1989
CHIRURGIE ENDOSCOPIQUE
AGEE & KING 1990
40CHIRURGIE ENDOSCOPIQUE
MENON 1993
41 Conclusions
: High-level evidence from
randomized controlled trials indicates
that …
Récupération de la force (pinch + grip)
42Sensibilité cicatricielle
Durée d’incapacité de travail
43Durée d’incapacité de travail
Différence moyenne : 9 jours en faveur de la technique
endoscopique
COMPLICATIONS…
44> 500.000 Patients
Complications
Infections : 5/1000 ECTR versus 8/1000 OCTR
45 Complications
Infections : 5/1000 ECTR versus 8/1000 OCTR
Déhiscence de plaie : 1,5/1000 ECTR versus 3/1000 OCTR
Complications
Infections : 5/1000 ECTR versus 8/1000 OCTR
Déhiscence de plaie : 1,5/1000 ECTR versus 3/1000 OCTR
Lésion iatrogène du nerf médian :
1,7
0,59
46 Complications
Lésion iatrogène du nerf médian :
Complications
Lésion iatrogène du nerf médian :
47 Complications
Lésion iatrogène du nerf médian :
Complications
Récidive / Réintervention
48 Complications
Récidive / Réintervention
Complications
Algodystrophie
49 Coût
Coût
50 Coût
> 500.000 Patients
MERCI!
51Vous pouvez aussi lire