Séminaire de recherche translationnel SRLF, Paris 4 Décembre 2018 - La suppléance rénale : l'acte de naissance de la réanimation
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous
Séminaire de recherche translationnel SRLF, Paris 4 Décembre 2018 La suppléance rénale : l’acte de naissance de la réanimation Bertrand Souweine, Clermont-Ferrand Absence de conflits d’intérêts sur ce thème

Definition of critical care medicine
History of critical care medicine
History of renal replacement
therapy
Relationship between the dawn of
RRT and the birth of critical care
medicine
« Le mé'er que je fais, est le même que celui des sages-femmes, à cela
près que j'aide à la délivrance des hommes et non des femmes, et que
je soigne non les corps, mais les âmes en mal d'enfant. »
D’après Platon dans le Théétète citant Socrate
Definition of critical care medicine Intensive care medicine – or critical care medicine – is a branch of medicine concerned with the diagnosis and management of life-threatening conditions that may require sophisticated life support and monitoring Offered to those whose condition is potentially reversible and who have a good chance of surviving with intensive care support – A prime requisite for admission to an intensive care unit (ICU) is that the underlying condition can be overcome –

Definition of critical care medicine
Care delivered in special care units
Continuing on-site monitoring
• Use of “real time” electronic monitoring of vital signs,
hemodynamic and respiratory parameters, and
complementary measurements on blood and body fluid
Continuing on-site care management
• Physicians with training in critical care medicine referred
to as, intensivists, physically on site
• Professional nurses
• Therapists
• Clinical pharmacists
Individual techniques to support organ failure
Resuscitation by the
routine use of chest
compression, defibrillation
and pacemaker insertion
Vo l u m e m a n a g e m e n t
guided by measurement of
intravascular pressures
and cardiac output
Intubation and mechanical
ventilation
Hemodialysis (RRT)
Nutrition support
Extracorporeal life support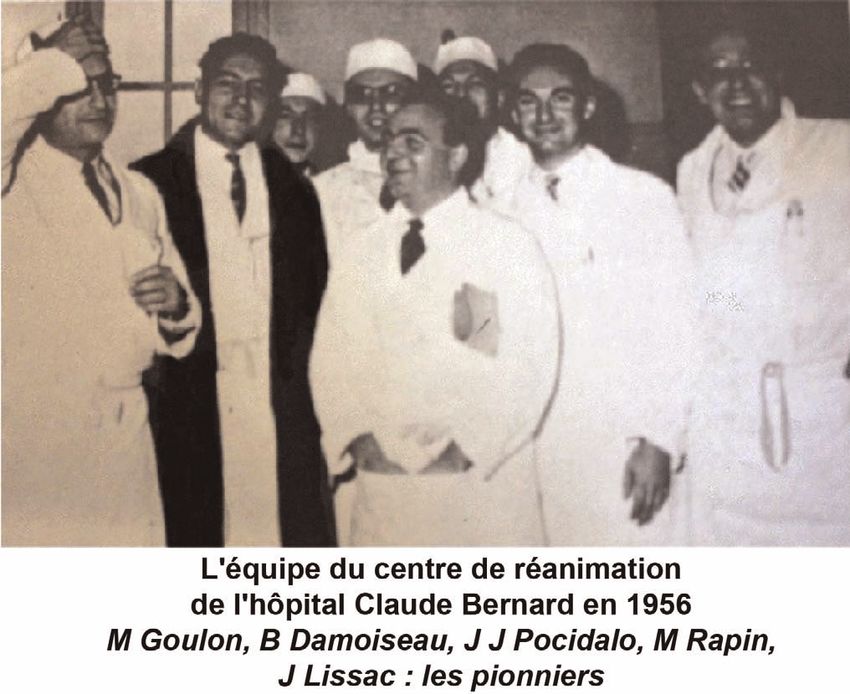
History of critical care medicine An illustration of the charge of the Light Brigade at Balaclava during the Crimean War
Florence Nightingale
1820 – 1910
demanded that the most
seriously ill patients were
placed in beds near to the
nursing station so that
they could be watched
more closely, creating an
early focus on the
importance of a separate
geographical area for
critically ill patients.
The birth of critical care medicine

(14..-1494)
Claudius Galien (130–200)
Andreas Vesalius (1515–1564)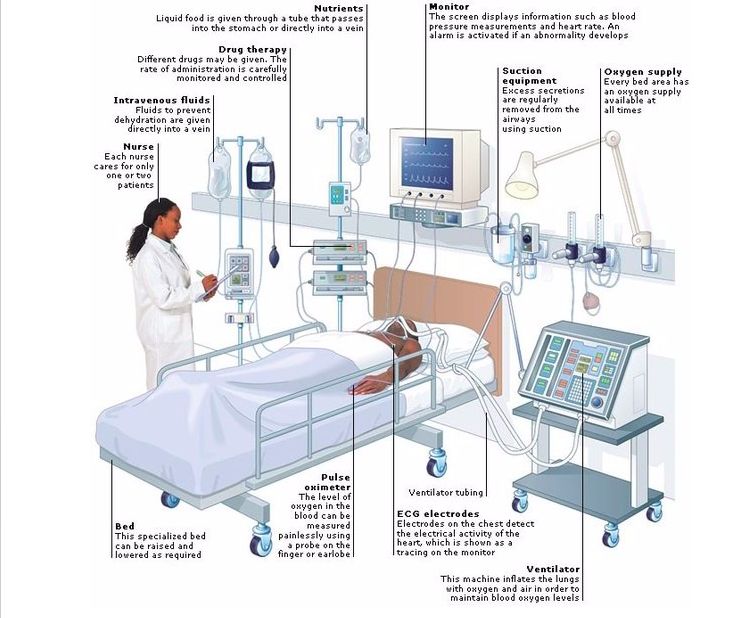
« En résumé, c’est donc le manque d’oxygène ou l’asphyxie qui amène la mort dans l’empoisonnement par le curare. S’il en est ainsi, c’est l’oxygène qu’il faut rendre pour rappeler à la vie, et le contrepoison sera simplement la respiration artificielle, c’est-à-dire un soufflet qui, remplaçant les mouvements respiratoires éteints, introduira graduellement et avec des précautions convenables de l’air pur dans les poumons. On peut dire alors que l’on tient dans ses mains l’existence de l’individu empoisonné ».
The birth of critical care medicine took place in Copenhagen, Denmark, during and after the poliomyelitis epidemic in 1952/1953.
The Blegdam Hospital, responsible for the treatment of poliomyelitis, counted only one tank respirator and six cuirass respirators for a daily admission of 6–12 patients with respiratory failure
History of Critical Care Medicine
A last desperate attempt to save the life of a 12-year-old
turned out surprisingly well
Henry Cai Alexander Lassen (1900–1974)
Mogens Björneboe Bjørn Ibsen
A young patient with poliomyelitis being manually ventilated by a medical student during the poliomyelitis epidemic in Copenhagen, 1953
[Source: Medical History Museum in Copenhagen]Meeting at Bergham hospital, 27 August 1952
Bjørn Ibsen, however, attributed the high blood pressure and
the high “total CO2 content” in plasma to an accumulation1085of
carbon dioxide in the patient’s blood. The high “total CO2
content” was,care according to more
achievements but long remained astonishingly silent
about his intensive contribution, Ibsen took Ibsen, not an expression of a
metabolic
pioneering workalkalosis
on intensive care but it have
indicated,
pride in his discoveries on the treatment of shock than his
[9]. There been quite to the contrary, a
respiratory
work concerning acidosis.
speculations [10] over why Ibsen chose to publish his
this new branch of anaesthesiology as
late as 1958, in a small journal and in a language
unknown to most of the world (Danish) [11]. Ibsen was
nevertheless an ambitious physician: He decided to
become an anaesthesiologist because it would take too
long to reach a senior position as a surgeon, and travelled
to the USA to learn state-of-the-art anaesthesia from
Dr. Beecher (Massachusetts General Hospital) [12].
Ibsen humbly pointed out ‘‘what we did was just to use
the principles and techniques, which served us well in the
operating theatre, also on patients with medical diseases’’
[10]. After having carefully collected historical facts,
some so far unpublished, and after interviewing Ibsen, I
came to the conclusion that he placed his performance in
perspective to the mentoring and inspirational role played
in the development of intensive care by another
colleague: Mogens Björneboe.
The poliomyelitis epidemic in Denmark in 1952 was
dramatic by all standards. The number of patients with Fig. 1 A young patient with poliomyelitis being manually ventilated
respiratory failure was higher than in any other European by a medical student during the poliomyelitis epidemic in Copenha-
gen, 1953 [Source: Medical History Museum in Copenhagen]
country [2]. The Blegdam Hospital, responsible for the
treatment of poliomyelitis, counted only one tank respira-
Bjørn Ibsen (1915-2007)
tor and six cuirass respirators for a daily admission of 6–12
December [6]. Bertelsen and Cronqvist determined that the
first ‘‘real’’ intensive care patient was a 43-year-old maleHistory of Critical Care Medicine Over 300 patients developed respiratory paralysis within a few weeks, and the ventilator facilities at the infectious disease hospital were completely overwhelmed. The heroic solution was to call medical students to provide round-the-clock manual ventilation using a rubber bag attached to a tracheostomy tube. One report states that 1,500 students in all took part in this activity with a total of 165,000 h
Engström 150 Carl Günther Engström (1915-1982)
La réanimation en France
Branche issue des salles
d'opération et de réveil, réalisée
par les médecins anesthésistes
Branche issue de
l’Hôpital Claude-Bernard
pour la réanimation
respiratoire
Branche issue de l’Hôpital
Necker pour la réanimation
métaboliqueHistoire de la réanimation en France En France c’est le 1er septembre 1954 que devait s’ouvrir le centre de réanimation neuro respiratoire de l’Hôpital Claude Bernard sous la responsabilité du Pr Pierre Mollaret avec comme mode de fonctionnement, novateur pour l’époque, la présence d’un médecin 24h/24h.
Réanimation (2011) 20:72-78 73
Engström 150
Construction
Pr Hamburger, qui modifia leàmodèleClaude Bernard
de Kolff et Merrill
aux États-Unis et réalisa, pour la première fois au monde,
er
1 septembre du1954,RPR puis
date de l’ouverture du
du centre de réani-
mation neurorespiratoire de l’hôpital Claude Bernard à Paris.
„Claude Bernard“ (JJ Pocidalo)
une séance d’hémodialyse, le 10 novembre 1954. À cette
époque, la dialyse intestinale par perfusion digestive et la
Jusque-là en effet, on ne disposait, pour aider un malade à
respirer, que du bouche-à-bouche, de la désobstruction pha-
dialyse péritonéale effectuée avec deux drains d’entrée et ryngée et de la méthode de Schaefer. L’oxygénothérapie seLa suppléance rénale : l’acte fondateur
de la réanimation : non
mais…La suppléance rénale : un des actes fondateurs de la réanimation
Arétée de Capadocce (?90-120) La fonction rénale est d’assurer la sécrétion de l'urine à partir du sang et son évacuation vers la vessie. L'unique fonction de celle-ci est d'expulser l'urine.
"Tout boucher sait que les reins
sont reliés à la vessie par les
uretères".
Galien rejette la filtration
Claudius Galien (130–200)“Dans l’expérimenta'on sur les corps bruts, il n’y a à tenir compte que d’un seul milieu, c’est le milieu cosmique extérieur : tandis que chez les êtres vivants élevés, il y a au moins deux milieux à considérer : le milieu extérieur ou extra-organique et le milieu intérieur ou intra-organique. [...] Car, ainsi que je l’ai déjà̀ dit ailleurs, la complexité́ due à l’existence d’un milieu organique intérieur est la seule raison des grandes difficultés que nous rencontrons dans la détermina'on expérimentale des phénomènes de la vie et dans l’applica'on des moyens capables de les modifier.”
• La défaillance rénale conduit à l’accumulation dans le sang et la totalité de l’organisme de substances toxiques normalement excrétées par le rein • Ces substances pourraient être éliminées à l’aide d’un processus de diffusion à travers une membrane • Le remplacement de la fonction rénale par l’hémodialyse
Osmose : un phénomène physique de diffusion
René Joachim Henri Dutrochet (1776-1847)
Transfert d’eau à travers des membranes animales en
fonction des différences de concentration en substances
dissoutes qui existent de part et d’autre de la membraneThomas Graham
Principe des membranes semi-perméables
1854
En séparant par une membrane de vessie de
bœuf deux compartiments, dont l’un l’eau, et
l’autre de l’eau pure seulement, on obtient,
après un temps d’équilibration, des
concentrations identiques des deux côtés de
la membrane pour les petites molécules.
• 1861, Fait passer l'urée contenue dans de l'urine vers de l'eau
au travers de cette membrane
• Crée le nom de« dialyse », du grec « dissolution, séparation»John Haycraft
1884 Ü>] -V ÀÀ\ ÀÕ`] > >ÌV>}Õ>Ì «i«Ì`i
VÌÌ}° ÜiÛiÀ] Ã Vi ÃÌÕ>ÌÃ]
ÀÌiÃ Ì i ÀÕ` «Ài«>À>Ì `` VVÕÀ
i` >Þ vÕÀÌ iÀ VV> ÕÃi v Ì Ã «Ài«>À>
iiÃÃ] Ì i £ÎäÃ] ÀÕ` iÝ«iÀiVi`
i Ì i ÀiV ÃÕÀ}i /iÀiÀ Ì Õ} Ì
Þ v ÀÕ` }iiÀ>Ì >` ÀiVi`i`
VÌ iiV ià >à > ` v `ÀÕ} vÕà À>Ì iÀ
À iÃÃ ®«ÕÀi iÝÌÀ>VÌÃ Ì iÀiv £Ó®° VÌÛi
Li VÌÕÕÃÞ Àii>Ãi` Ì Ì i L` `ÕÀ
L` ÃÕV} Ìi] LÕÌ > V«iÌÃ v }ÕÀi £\Medicinal leech
i`V> iiV (Hirudo
ÀÕ` medicinalis)
i`V>î ÀiÃÌ} >` Ü>Ì
}®°
iV LÌiÃ] L` ÃÕV}] >` ÀÕ` vÕ
` LÞ Ì i ÃÌ° /iÀiÀ V>i` Ã iÌ `
}º° / Ã Ü «ii` Ì i `À vÀ > LÀ>` >LÕÌ Èääqnää >ÌÌ ÀL ÕÌà /1®É} «ÀÌi° Ì i v
}° 1vÀÌÕ>ÌiÞ] Ì Ã ÀiÛÛ> v i`V> Ü} Þi>ÀÃ Ì iÃi «ÀVi`ÕÀià ÜiÀi VÃ`iÀ>LÞ «ÀÛi` LÞ
Ì
>}iÌÃ Ü>Ã ÃÌ««i` V«iÌiÞ Ü i Ì iÀ ÌÀ`ÕVÌ v iiVÌÀ`>ÞÃÃ Ü iÀi Ì i >ViÌi«ÀiV«Ì>Ìi`
ÕÀVià -ÕÌ >ÃÌiÀ ÕÀ«i Ü>à ÌiÀ iÝÌÀ>VÌà ÜiÀi vÕÀÌ iÀ «ÕÀvi` Vi« >i iLÀ>ið / à Ài
7>À ° Ì >LÕÌ Ì i Ã>i Ìi] iÜ «ÜiÀ ÃÕÌi` ÀÕ` «Ài«>À>ÌÃ ÜÌ > >VÌÛÌÞ v Ó]xääqÓ]Çää
iÃÛi >ÌÕÀ> i«>À® >` ÃÞÌ iÌV VÕ /1É}° vÕÀÌ iÀ iÃÌi v Ì i «Ài«>À>ÌÛi «ÕÀvV>Ì v
Ìà LiV>i >Û>>Li >` à «ÀÛi` Ì Li ÀÕ` Ü>Ã Ì i ÌÀ`ÕVÌ v «>«iÀ iiVÌÀ« ÀiÃð
}ð / ÕÃ] Ì i vÕÌÕÀi v ÀÕ` Ü>à ÕViÀ `ÕVÌi` >À}i Ài>VÌ ÛiÃÃiÃ] Ì Ã ÀiÃÕÌi` Ì i «ÕÀvV>Ì
LiVi > `ÀÕ} vÀ VV> ÕÃi µÕÌi `ÕLÌ v ÀÕ` ÜÌ > ëiVvV >VÌÛÌÞ v n]äääq]äää /1É} Ì i
i >ÌÕÀ> Ì>Ìà ÃÕ««Þ >` Ì i iÝÃÌ ``i v Ì i £Èäà >` Ü >Üi` vÕÀÌ iÀ « >À>V}V>
Õ}Ã Ü V `` Ì >Ûi Ì iÃi Ì>Ìð ÌiÃÌ}°Gangrene 5 The hospital took care of 119 persons, 83 of them
Tetanus
Nephritis
Antonino D’Antona (1842-1913) was the first
5
2
inhospitalized
were describing the
for fractures, crush
wounds, internal dis
eases due to the quake (mainly rheumatism) an
Total
syndrome with renal failure following the Messina
22
earthquake of
minor surgeries. For each of them a narrative was re
December 28, 1908 ported and available for care. In the report (Figure 1
read to the German Society of Surgery in 1909 [7], v
Colmers referred to fractures, the gangrene due t
Carmela Bisaccia1, Natale Gaspare De Santo2, Luca S. De Santo3
compression (drückgangrene), the necrotic process o
(1) Mazzini Institute, Naples, Italy skin and muscles, and on the care and the healing o
(2) Department of Medicine, Second University of Naples, Naples,the Italywounds. There were 6 deaths. The hospital pro
(3) Chair of Heart Surgery, University of Foggia, Foggia, Italy vided ambulatory care to some 300 patients. From
Address correspondence to:
the report, which was enriched by illustration
emergese-mail:
Carmela Bisaccia; Mazzini Institute, Naples, Italy; Cell:+39 335 7084426; a good description of rabdomyolysis. Th
cbisacc@tin.it
kidney and the urinary tract are mentioned on 10 oc
casions. The reasons are highlighted in Table 1. H
did not see patients with shock because of the tim
Abstract elapsedhis
Because from
latethe eventhe(14
arrival, diddays).
not treat patients with s
rabdomyolysis.
Report of Rocco TheCaminiti
third medical report is that of Rocc
igure 4.
There is confusion about the first description of the association between
rofessor Antonino D'Antona (1868-1946), collaborator
Rocco Caminiti of D’Antona
was Chief at the
of surgery atUniversity
the Loret
crush syndrome and renal failure. It has been traditionally attributed to ofHospital
surgery in
at the Loreto Hospital. He directed
Naples and Clinical Professor of a rescue
Surgerg
Bywaters and Beall. The present study aims to analyze the problem by Giovanni and Reggio Calabria. In 1910, he reported on r
analyzing medical reports on the Messina-Reggio
3 Calabria earth-quake of patients treated in the place of the disaster. Therefore t
December 28, 1908 by using documents heretofore unknown. It indicates that Antonino D’Antona holds the priority for
demonstrates that first description of rabdomyolysis with renal failure is rabdomyolysis and kidney injury. There is no longer a p
attributed to Antonino D’Antona (1842- 1913). D’Antona, professor of Bywaters syndrome.
surgery at the University of Naples, coordinated the health net organized in
Naples to assist persons wounded during the quake. Many of them in shock Key words: Antonino D’Antona, Franz von Colmers,
were transferred to Naples by ships. Franz von Colmers (1875-1960) was the renal failure, Rocco Caminiti
chief surgeon of the German Mission of the Red Cross after the quake.
Figure 1.
The paper of Dr. Colmers on his surgical activity in Syracuse after the
quake
renal failure and raised the possibility that theJohn Abel artificial kidney
1913
Hemodialysis sessions in dogs
Anticoagulation with hirudin
On the removal of diffusible substances from the circulating
blood of living animals by dialysis
Abel JJ, J Pharmacol Exp Ther 1914;4:13—4.George Haas
1923
EER de15 minutes
Membranes colloïde
1922, UFH utilisée à partir de 1940
1927, Cellophane
Haas G. Dialysieren des strömenden Blutes am Lebenden. Klin Wochenschr 1923; 2: 1888WW 2
Willem Kolff, le père des générateur de dialyse 1943 • En 1945, une femme de 67 ans dans le coma urémique repris conscience après 11 heures sur la machine de Kolff He obtained a PhD degree summa cum laude at University of Groningen on the subject
History of Dialysis 1947: Nils S Alwall came up with a dialyzer to carry out the process of ultrafiltration and remove excess fluids from the body. Nils S Alwall (1904-1986)
Mobile Army Surgical Hospital (MASH) 1950-1953 300 L dialysates were used during each 6-hour dialysis
Among the injured soldiers who reached medical care, acute renal failure inverted the casualties’ reasonable survival expectancy of 90% to 95% without renal failure to a 5% to 10% survival rate The probable causesin these young, hypercatabolic, oliguric soldiers. • Potassium intoxication that produced cardiac arrest; • Fluid volume overload (to ‘‘wash out’’ the oliguric kidneys) that produced pulmonary edema; • ‘‘Uremic coma’’ with severe azotemia • Metabolic acidosis,
Each dialysis was therefore a medical-chemical-surgical-
schan
patient—care tour de force
gure 5 The Kolff-Brigham dialyzer in operation, Renal Figure 6 The team headquarters for recording and comput-
nter, Korea, 1954. ing research data.
Teschan PE, Hemodialysis International 2011; 15:3–7History of Dialysis
Epuration extra-rénale en France 1950s Derot et Legrain, Hamburger et Richet, Traeger Exsanguino transfusion, Marcel Bessis (1917-1994) médecin hématologue en 1947, néphrite urémique
traitement avaient
(futur prix Nobel de physiologie montré que la rétention d'urée n'était qu'un élément du syndrome
ou méde-
fondateur de l’école de diabétologie de
Juste après la guerre,
humoral, sans doute moins dangereux que l'hyperkaliémie, l'acidose ou l'hyperhydra-
cine, en 1980) était tation
de ceux-là.
etc., toutes causes fréquentes de mort. Et ce domaine était celui qui avait
il réputation
fait la entendit parler
de Necker.
l’Hôtel-Dieu de Paris
des travaux d’un médecin néerlandais, le
Dr Willem Johan Kolff,
Dès l'arrivée à Necker, la dialyse intestinale fut mise en oeuvre, peu puissante,
qui pratiquait unepénible pour le patient et nécessitant une surveillance humorale
prolongée des heures,
épuration extra-rénale par hémofiltration
continue. En e!et, la perfusion dans le jéjunum de 4 litres par heure n'était pas sans
aléas enqu’il
avec un dispositif original raison desmis
avait modifications incessantes du temps de transit et de l'emplacement
avec Pierre Tanret, ils mettent au point, les
le train et se renditpar
de l'extrémité de la sonde, modifiant et les passages passifs à travers la paroi intestinale
au point [4]. MauriceetDérot,
encoreen
auxencore
plus
Pays-Bas
1948, prit
les transferts
pour
plus d'échecs.
actifs. Des succès enivrants ont été acquis, contrebalancés
Aussi est-ce avec soulagement que fut saluée la mise en
premiers, la dialyse péritonéale et son
service du
rencontrer ce précurseur,
les plans du dispositif
et Rein Artificiel
revint avec de Kol!-Merrill en novembre 1954 qui, l'expérience aidant, fut
bientôt quelque peu amélioré et appelé Necker. Le pronostic des insu#sances aiguës
qu’il fit construire
réversibles fut transformé.
application dans l’hépatonéphrite de la
par les ateliers de l’Assistance publique
de Paris (peut-on s’imaginer cela de
septicémie post-abortum,
nos jours !!) [5]. J’ai aidé à utiliser cette
même machine lorsque j’étais externe
Figure 1. Le Professeur Maurice Dérot dans le service à l’Hôtel-Dieu, au début
(1901-1985).
Maurice Dérot (1901-1985) des années 1960, puis interne à la fin de
cette même décennie. Il s’agissait d’une
la nutrition et la diététique, avec son ami énorme « lessiveuse », en réalité une
le Pr Henri Bour, à qui il restera attaché cuve en inox de plus d’un mètre de dia-
tout au long de sa vie professionnelle. mètre, au centre de laquelle se trouvait
1948, M Dérot se rend un long tube de cellophane enroulé en
cylindre, dans lequel le sang du patient
Maurice Dérot, l’Hôtel-Dieu était propulsé, alors qu’à l’extérieur
aux Pays Bas et obtient
et la néphrologie circulait, à l’air libre, la « sauce » électro-
lytique chargée des échanges ioniques
l’accord de Kolff
Cette première orientation découle de
sa formation auprès de Louis Pasteur-
et des toxines à éliminer (la membrane
se fissurait régulièrement et l’énorme
Valéry-Radot. Ses premiers travaux quantité de liquide de la cuve se colorait
portent, rappelons le, sur la créatinine de rouge : on peut aisément imaginer le
sérique [1]. Sa première publication branle-bas de combat entrainé par cet
notable porte, en 1935, sur les hépato- incident ; il fallait très rapidement clam-
néphrites [2], sujet qu’il n’abandonnera per et mettre en place une deuxième
jamais ensuite. Les réalisations remar- membrane qui « trempait » non loin de
quables dans le domaine ont été de là, prête à l’usage ; Alors
la séance durait des
que la Néphrologie était une discipline presque désarmée jusqu'en 1950, en
Gabriel Richet et Marcel Legrain, Boston
créer une école de néphrologie à l’Hô-
tel-Dieu, école qui est restée riche de
heures… y comprisquatre la nuit).
ans elle entra dans l'ère thérapeutique avec la maîtrise des désordres hydro-
Toute cette activité était pilotée par le PrSoc Nephrologie :: d'hier et d'aujourd'hui 03/1
Jean Hamburger rechercher dans un cas d'anurie prolongée, en principe réversible, de telles anomalies, à
les corriger et à provoquer ainsi la reprise des fonctions rénales. Fort de ce succès, il
poursuivit ses travaux au laboratoire tout en élargissant le champ de son investigation
clinique. Il ne faisait qu'appliquer le principe que la bonne médecine exige une
recherche conjointe. Necker devint alors le premier centre français où, dans toute la
pathologie mais spécialement en Néphrologie, les désordres hydro-électrolytiques
étaient dépistés, analysés et traités. Les succès obtenus valurent au service un a"ux de
Définition des secteurs hydriques du corps humain
patients de tout le territoire et même de l'étranger.
Les insu!sances rénales aiguës et la dialyse
Parmi les cas venant à Necker se trouvaient nombre d'anuries, toxiques, infectieuses
post-opératoires, post-abortum ou médicales soit encore immunologiques tels les
accidents des transfusions qui étaient alors nombreux. Le contrôle des apports d'eau et
Les insuffisances rénales aigues et la dialyse (dialyse
de sel était ine#cace pour corriger toutes les anomalies humorales exposant à un risque
létal. Il fallait donc soustraire de l'organisme ce que le rein n'éliminait pas,
temporairement, puisque l'expérience de la guerre avait enseigné que de telles atteintes
rénales pouvaient être spontanément réversibles. Le service était bien préparé à utiliser
intestinale / dialyse péritonéale à 2 drains)
la dialyse, dont l'intérêt était encore mis en doute. En e!et, les premiers essais de ce
traitement avaient montré que la rétention d'urée n'était qu'un élément du syndrome
humoral, sans doute moins dangereux que l'hyperkaliémie, l'acidose ou l'hyperhydra-
tation etc., toutes causes fréquentes de mort. Et ce domaine était celui qui avait
fait la réputation de Necker.
Dès l'arrivée à Necker, la dialyse intestinale fut mise en oeuvre, peu puissante,
prolongée des heures, pénible pour le patient et nécessitant une surveillance humorale
Méthodes de suppléance devaient aider à passer le cap la
continue. En e!et, la perfusion dans le jéjunum de 4 litres par heure n'était pas sans
aléas en raison des modifications incessantes du temps de transit et de l'emplacement
de l'extrémité de la sonde, modifiant et les passages passifs à travers la paroi intestinale
plupart des insuffisances rénales aigues et des désordres
et encore plus les transferts actifs. Des succès enivrants ont été acquis, contrebalancés
par encore plus d'échecs. Aussi est-ce avec soulagement que fut saluée la mise en
service du Rein Artificiel de Kol!-Merrill en novembre 1954 qui, l'expérience aidant, fut
bientôt quelque peu amélioré et appelé Necker. Le pronostic des insu#sances aiguës
graves de l’équilibre hydro-électrolytique
réversibles fut transformé.
Alors que la Néphrologie était une discipline presque désarmée jusqu'en 1950, en
quatre ans elle entra dans l'ère thérapeutique avec la maîtrise des désordres hydro-Epuration extra-rénale en France 1950s Derot et Legrain, Hamburger et Richet, Traeger 1950s • Maurice Dérot, Marcel Legrain, ,premières publications françaises sur le RA • Jean Hamburger et Gabriel Richet > 150 sessions de RA (Kolff-Merill) Le rein de Kolff-Merrill modifié par Hamburger fut fabriqué par Usifroid et diffusé en province… 300 kg..
FIG. 4. Number of dialyses employed prophylactically in 15 patients and survival (4,5), more recently we have been involved in
Prophylactic hemodialysis in the treatment of
with acute renal failure. the measurement of the dose of delivered dialysis in the
acute renal failure patient (too little indeed) and will be par-
arteries were also used, as well as a variety of other
ticipating in a multicenter, NIH-sponsored research study on
superficial veins. The cannulae delivered and accepted an
acute renal failure that will examine the possible parameters
acute renal failure
adequate blood flow (75-250 ml./min); among arteries
(frequency, dose, continuous versus intermittent, and nutri-
for an approximate average of 10 days (range, from one
tional parameters) that may improve the still poor outcome
to 22 days) each, while the average life of a single-chan-
of patients with acute renal failure.
nel venous cannula was about seven days (range, from
A careful reading of the report by Teschan et a!. in this
one to 20 days). Averages of 6. 1 and 4.3 dialyses were
issue also shows that the article contains the first description
served by the arterial and venous cannulae, respectively.
of regional heparinization (using heparin and protamine
When these cannulae became nonfunctional, surgical
infusion) the importance
and of adequate nutrition in such
cannulation of further vessels, or of the same vessel at a
patients as well. The regional heparization and the practical
different site, was undertaken. In addition, multichannel
assay for heparin was later published separately in the New
cannulae* were also used, and these were usually func-
England Journal of Medicine (6). More importantly,
tioning and not associated with thrombi after from one to
Teschan and his team clearly articulated the need to start
three weeks’ use. Insertion of the cannulae on the day
prior to dialysis prevented oozing from cutdowns during dialysis early in the course of renal failure, using “an orga-
nized, disciplined and well supported team of trained phy-
dialysis, even under total heparinization.
sicians, nurses and technicians” and the “executive resolve
Cultures from the lumen of the seabed cannulae some-
times revealed growth of organisms within a few days of
. . . to carry it out without allowing inertia . . . to result in
procrastination and delay”, and to apply dialysis to the
the insertion. The organism recovered in such instances
was usually an Aerobacter-Kiebsiella, suggesting that con-
“relatively healthy patient” instead of the waiting for the
tamination may have occurred in the process of handling patient to become “relatively ill”. It is time that we learned
the cannulae. Despite various technical maneuvers
this wisdom.
designed to eliminate this problem, most-but not all- References
dialyses in most of these patients were associated with a
1. Teschan PE, Post RS, Smith LH Jr: Posttraumatic renal insuffi-
30- to 60-minute shaking chill, beginning from 30 to 60
ciency in military casualties. I. Clinical characteristics. II. Man-
minutes after the start of dialysis, frequently with a rise in
agement, use ofan artificial kidney, prognosis. Am J Med 18: 172-
* Fabricated by Cordis Corporation, 24 1 Northeast 36th Street, 186(I); 187-198(11), 1955
Miami 37, Florida. 2. Teschan PE: Hemodialysis in military casualties. TransASAlO 1:
52-54, 1955
3. Teschan PE, Baxter CR, O’Brien RF, Freyhof NM, Hall WH:
Prophylactic hemodialysis in the treatment of acute renal failure.
Ann Intern Med 53: 992-1016, 1960
4. Hakim RM, Wingard RL, Parker RA: Effect of the dialysis mem-
brane in the treatment of patients with acute renal failure. N Engi
JMed33l: 1338-1342, 1994
5. Himmelfarb J, Tolkoff-Rubin N, Chandran P, Parker RA, Wingard
RL, Hakim RM: A Multicenter Comparison of Dialysis Mem-
branes in the Treatment of Acute Renal Failure Requiring Dial-
ysis. JAm Soc Nephml 9: 257-266, 1998
6. Darby JP, Sorensen R, O’Brien TF, Teschan PE: An efficient
heparin assay for monitoring regional heparinization and hemo-
FIG. 5. Plastic cannulae fitted for chronic vessel cannulation and dialysis. N Engi J Med 262: 654-657, 1960
heparin instillation.
Teschan P, Ann Intern Med. 1960 Nov;53:992-1016.112 Had do-not-resuscitate order in place
At ICU discharge
Timing of RRT in AKI
2.00±1.26 2.19±1.47 0.15
336 Were enrolled in another mortality trial
31 Did not give consent
At hospital discharge 1.46±0.98 1.61±1.30
144 Had other reason 0.31
* Plus–minus values are means ±SD. 488 Underwent randomization
† Acute kidney injury in failure stage was defined according to the RIFLE classification.
‡ This category includes patients in the delayed-strategy group who met criteria for emergency renal-replacement therapy. Metabolic acido-
sis was defined as a pH less than 7.15 and a base deficit of more than 5 mmol per liter or a bicarbonate level of 18 mmol or less per liter.
Hyperkalemia was defined as a potassium level of more than 6.5 246 mmol per liter
Were assigned with
to receive characteristic electrocardiographic
early changes.
242 Were assigned The
to receive me-
delayed
Table S1. Criteria mandating RRT initiation
dian pH in the
anddelayed RRTpotassium
median strategy group*
values were calculated only in patients who underwent
renal-replacement therapy renal-replacement therapy because they met
renal-replacement therapythese
Oliguria or anuria for more than 72 hours after randomization
specific criteria. Fluid overload was defined as extravascular fluid overload that was refractory to diuretics, with pulmonary edema. Other
Serum urea concentration of more than 40 mmol/liter
reasons included worsening of the patient’s clinical status, with acidosis and hyperkalemia below the prespecified threshold, associated
Serum potassium concentration of more than 6 mmol/liter
with hyperlactatemia, with the need for emergency renal-replacement therapy as determined by the clinician treating the patient.
Serum potassium concentration of more than 5.5 mmol/liter despite medical treatment (bicarbonate and/or
§ Other criterion was worsening of multiple organ failure that mandated
7 Did not receive the initiation of renal-replacement therapy
239 Received 93 Did not in the opinion of the149
receive cli-
Received
glucose-insulin infusion) renal-replacement therapy renal-replacement therapy renal-replacement therapy renal-replacement therapy
nician caring for the patient, confirmed by an increase of at least 2 points in the SOFA score (not a prespecified criterion for emergency
pH below 7.15 in a context of pure metabolic acidosis (PaCO2 below 35 mmHg) or in a context of mixed
renal-replacement therapy).
acidosis with PaCO2 of 50 mmHg or more without possibility of increasing alveolar ventilation
¶ The number of days free of renal-replacement therapy, mechanical ventilation, or vasopressor therapy was calculated according to the
Acute pulmonary edema due to fluid overload responsible for severe hypoxemia requiring oxygen flow 2 Died before renal-replace- 21 Died before renal-replace- 41 Underwent renal-replace-
number of days the patient was alive without the intervention
rate of more than 5 l/min to maintain an SpO2 of more than 95% or an FiO2 greater than 50% in patients ment therapyatwasday 28; patients who 134
initiated died
Diedwere assigned zero free days.
ment therapy was initiated ment therapy before 48 hr
∥ In patients who received renal-replacement
already on invasive or non-invasive mechanical ventilation and despite diuretic therapy
therapy, the1 renal component
Had catheter-insertion failureof the SOFA score was calculated 70 on the basis
Had spontaneous of urine
recovery output only.
because condition that
4 Had spontaneous recovery of renal function met criteria for emergency
** Creatinine values are for all living patients who were nooflonger receiving renal-replacement therapy.
renal function 2 Did not receive renal- renal-replacement therapy
! 1 Died replacement therapy for had developed
other reasons 28 Died
108 Underwent renal-replace-
ment therapy after 48 hr
59 Died
performed easily or safely in patients with hemo-
dynamic instability in the early phases of septic 1.00and Follow-up.
Figure 1. Screening, Randomization,
shock, so starting such therapy earlier would not
ICU denotes intensive care unit.
improve fluid balance.
Proportion Surviving
Primary Outcome 0.75
Our results show that initiating renal-replace- Further stratification according to center and
Follow-up data at 90 days were available for 477 adjustment for preexisting chronic renal failure
ment therapy too early could unnecessarilypatients
ex- (98%). The early initiation of renal- and exposure to nephrotoxic agents did not
Delayed strategy
pose patients in whom renal dysfunction would replacement therapy did not0.50result in lower mor- change the results.
tality at 90 days than the delayed strategy; 138 of
have recovered spontaneously to the risks associ-
239 patients (58%) in the early-strategy group Secondary Outcomes
Early strategy
ated with renal-replacement therapy. Indeed, 29% 0.25
died and 128 of 238 patients (54%) in the de- The delayed strategy resulted in a significantly
of the patients in the delayed-strategy grouplayed-strategy
did group died (P = 0.38)P=0.52 (Table 2). larger number of days free of renal-replacement
not require renal-replacement therapy because 0.00
1435
they had spontaneous recovery of renal function, n engl
0 j med 379;15
30 nejm.org60 October 11,902018 120 150 180
although 26% of these patients (18 of 70 pa- The New England Journal of Medicine
Days since Randomization
Downloaded from nejm.org at INSERM DISC DOC on November 26, 2018. For personal use only. No other uses without permission.
tients) subsequently died, which is similar to No. at Risk Copyright © 2018 Massachusetts Medical Society. All rights reserved.
Delayed strategy 242 137 117 112 107 105 101
rates reported in other studies. It is possible
22
Early strategy 246 127 109 99 98 92 92
that more patients might have recovered without
renal-replacement therapy if the delay had been Figure 2. Overall Survival among Patients Assigned to Early Renal-Replacement
longer than 48 hours, as was observed in a re- Therapy and Delayed Renal-Replacement Therapy.
cent study.12 Mortality was higher among pa- In the early-strategy group, renal-replacement therapy was initiated within
tients assigned to the delayed-strategy group who 12 hours after documentation of acute kidney injury. In the delayed-strategy
met criteria for emergency renal-replacement ther- group, renal-replacement therapy was initiated 48 hours after the documen-
tation of acute kidney injury, if renal recovery had not occurred. If criteria
apy (68%
Gaudry S, N Engl J Med [28 of 41 patients]) than among those
375:122–133 Barbar SD, N were
Engl J byMed 2018;379:1431-42.
for emergency renal-replacement therapy met a patient in thisPickkers et al. Page 20
Current practice in RRT for AKI
Delayed > early
Fig. 3.
Current practice in RRT for AKI. The current standard of timing, vascular access, modality,
dose, anticoagulation and weaning from renal replacement therapy. RCT randomised
controlled trial, US ultrasound, CRRT continuous renal replacement therapy, IHD
intermittent haemodialysis
Adapted from Pickkers P, Intensive Care Med 2017;49:1198-1209Vous pouvez aussi lire