Bilan - Traitement O.R.L. et Maxillo facial
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous
06/12/2012
Bilan - Traitement O.R.L. et
Maxillo facial
Paris
6 décembre 2012
Le fait de bien comprendre les interactions entre
- la respiration buccale exclusive
- la croissance faciale
- les anomalies respiratoires durant le
sommeil
- les risques inhérents à l’étroitesse des VADS
Chez un enfant pré pubertaire
Permet de diminuer de façon très nette le prix de sa
prise en charge
Christian Guilleminault
1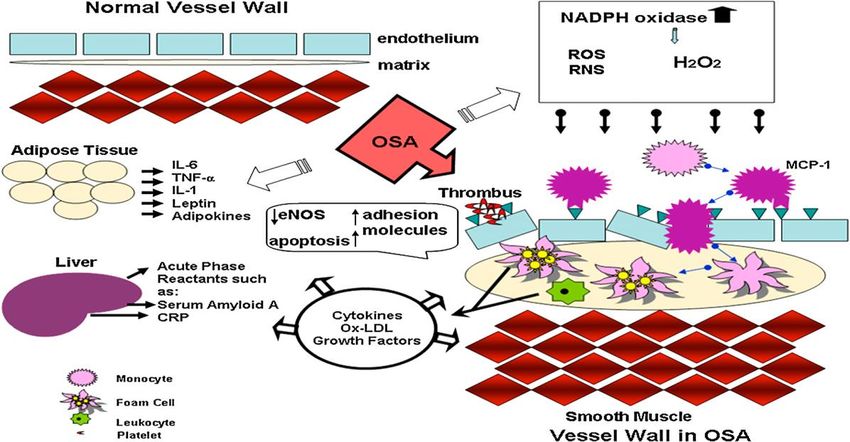
06/12/2012
Définition
L’anomalie fondamentale du SAOS est
la diminution du tonus musculaire
pendant le sommeil et donc par
conséquent une réduction du calibre
des VADS
« une guerre de couloir
aérien »
Définition
Il s’agit donc d’évaluer en
permanence les
responsabilités du
contenant / contenu
2
06/12/2012
Risque de SAOS chez l’enfant
Résistances nasales
Tissus lymphoïde
Compliance thoracique
Contrôle central
2mois 18mois
3
06/12/2012
4
06/12/2012
5
06/12/2012
Anomalies morphologiques
recherchées en rapport avec
l’O.R.L
6
06/12/2012
Obstructive sleep apnea syndrome due to adenotonsillar hypertrophy in infants
Michal Greenfeld
Le fait que l’origine du SOAS de l’enfant soit du à une anomalie neuromusculaire est sous
tendu par le fait que
- absence en éveil
- la présence d’HAVA ne signe le SAS que dans 2%
L’obstruction est due à 2 mécanismes
Contenant et contenu
C.L. Marcus, Pathophysiology of childhood obstructive sleep apnea: current concept, Respir.
Physiol. 119 (2000) 143/154
International Journal of Pediatric Otorhinolaryngology (2003) 67, 1055/1060
Facteurs de risque chez l’enfant
7
06/12/2012
Anomalies cranio-faciales et SAS
Incidence du SAS dans les anomalies
cranio faciales
• Robin 12,5%
• Apert –Crouzon –Pfeiffer 40%
• Achondroplasie 35%
• trisomie 21 45%
• mucopolysaccharidoses 89%
8
06/12/2012
Dimensions des VAS chez l’enfant apnéique
SAOS
Normal
Enfant et Voile du palais?
9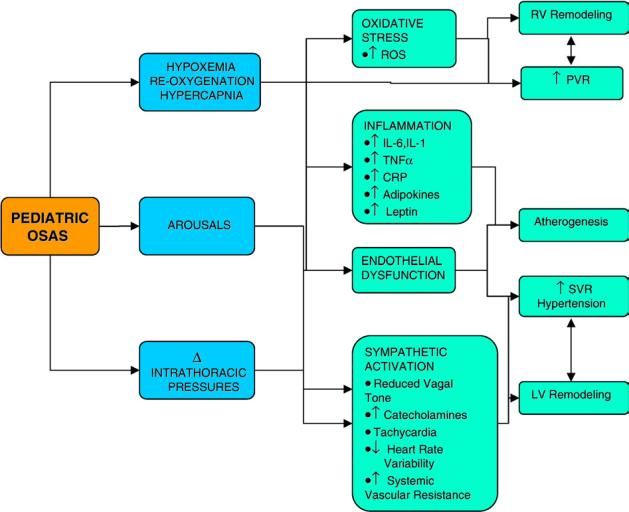
06/12/2012
The relationship between craniofacial anatomy and obstructive sleep apnoea
Chez les SAOS
1-Sont réduites
Les dimensions antéro-postérieures
Mandibulaires et maxillaires Contraction
La distance intermaxillaire
Le nasopahrynx
2-Sont agrandies
La longueur/épaisseur du voile Traction
L’hyoïde plus bas
AMA JOHAL J. Sleep Res. (2007) 16, 319–326
Traction
1006/12/2012
Contraction
La dysmorphose est–elle un élément
prédictif d’un syndrome d’apnée-
hypopnée ?
1106/12/2012
Craniofacial morphology and sleep apnea in children with obstructed upper airways:
Differences between genders
1-Axe facial
3-Profondeur face
77 G +F avec HAVA 4- ht faciale inf
46% SAS 5-angle mand
SEX RATIO 1
IAHG>IAHF
DOLICHOFACIAL=81%
IAH et MP, FD,VERT corrélés G pas chez la F
Analyse de Rickett’s (position de la mandibule et
direction de la croissance faciale)
Les dolichofaciaux (face longue et étroite) sont
majoritaires (BO et TRS)
Corrélations entre FD, MP et IAH seulement garçon
MP= direction croissance
FD= profondeur de la face donc mandibule r/ base
Renata Di Francesco Sleep Medicine xxx (2012)
Les patterns de l’enfant :
Intermédiaires entre SAS et contrôles
adultes
Face longue
Partie basse
1206/12/2012
Croissance mandibulaire et IAH
Croissance mandibulaire et IAH
1306/12/2012
Margaux 4 ans
Rétrognathisme mandibulaire
• iah=2
• Somnolence diurne
• agite +++
• nycturie +++
• Sieste
Classe II
1406/12/2012
Rétrognathisme mandibulaire
Examen O.R.L.
1506/12/2012
Amygdales
Mallampati
1606/12/2012
Stades de Friedman
Corrélation volume des amygdales et IAH
1706/12/2012
Pediatric tonsil size: Objective vs subjective measurements correlated to
overnight polysomnogram
IAH
P V A-A
A- Poids amygdale
B- Volume ’’
C- Distance inter-A
D- IAH pre-op
Taille subjective
(Mallampati)
Taille subjective est corrélée avec les mesures objectives A-B-C
Seules les mesures objectives sont corrélées avec sévérité du SAS (PSG) D
Otolaryngology - Head and Neck Surgery 2009
Et le nez ?
1806/12/2012
Mouth breathing: Adverse effects on facial growth, health, academics, and behavior
Yosh Jefferson
January 08, 2010
Résistance nasale
• Système capacitif
• Valve nasale
• Cycle nasal (2à4h chez 70% de la population)
• Reflexe « corporeo-nasal »
• RN enfant>adulte
• La symptomatologie d’obstruction n’est pas
corrélée avec la réalité
1906/12/2012
Relation of Nasal Air Flow to Nasal Cavity Dimensions
Toutes les resistances se situent de 0-3 cm et inexistantes de 3-5cm
Le volume est 1/proportionnel résistance nasale
3-5cm
0-3cm
0-5cm
Peak Nasal Inspiratory Flow
Arch Otolaryngol Head Neck Surg. 2009;135(6):565 Thomas Kjærgaard,
Rôle de la perméabilité nasale sur les dimensions
pharyngées aux 2 temps de la respiration
Radiology September 2005
Obstructive Sleep Apnea in Pediatric Patients: Evaluation with Cine MR Sleep Studies1
2006/12/2012
Perspectives
(obstruction nasale et TROS)
ON
1-↘flux nasalrécepteurs
↘ventilation/min + contraction phasique
génioglosse
2- ↗résistance ↗P°06/12/2012
30 enfants allergiques + RB
15 enfants contrôles +RN
Face longue
+retrognathe
Angle goniaque↗
Palais plus profond
60% de la croissance faciale
est effectuée à 4 ans
Les sutures sont non
modifiables à la puberté
2206/12/2012
Partitioning of inhaled ventilation between the nasal
and oral routes during sleep in normal subjects
MICHAEL F. FITZPATRICK, J Appl Physiol • VOL 94 • MARCH 2003 •
=
Avec résistance
nasale(effet paradoxal)
Pas de modifications du type de respiration buccale
pendant le sommeil pour patient sans résistance nasale
La position corporelle indifférente
REM-associated nasal obstruction: A study with acoustic rhinometry during sleep
+22,6%
+16,2%
+10,6%
+2,3%
Otolaryngology–Head and Neck Surgery (2008)
Luc G.T. Morris
2306/12/2012
Nasal nitric oxide in children with adenoidal hypertrophy: A
preliminary study
Le NO ↗chez
l’enfant VG+ mais
pas chez l’obstructif
S. Torretta International Journal of Pediatric Otorhinolaryngology 74 (2010)
Sleep impairment in allergic rhinitis, rhinosinusitis, and
nasal polyposis
Congestion nasale
-est commune et gênante dans les rhino sinusites ,atopie nasale et
polypose
-entraine une diminution de la filière nasale
-évaluation possible
-physiologique augmente en position couchée
-importante en début et fin de nuit
-s’aggrave au cours de la nuit par ↘du cortisol
-le symptôme le plus fréquent dans la rhinite allergique
-symptôme le plus gênant au regard du sommeil
Timothy J. Craig
American Journal of Otolaryngology–Head and Neck Medicine and Surgery 29 (2008) 209
2406/12/2012
High prevalence of allergic sensitization in children with habitual
snoring and obstructive sleep apnea.
Sur 39 sujets 8/14 P+ SAS+=57%
-24 garçons 10/25 P- SAS+ =40%
-14>0 phadiatop(P+)
- 18 SAS (46%)
L’allergie est présente chez enfants ronfleurs
L’allergie est souvent associée à un risque élevé de SAS
McColley S, Carroll J, Curtis S, et al. Chest 1997; 111:170–173
Effect of Intranasal Obstruction on Breathing
during Sleep*
Paul M. Suratt Chest 1986;90;324-329
25Index d’apnées –hypopnées
Résistance cmH₂O L-1S-1
Orale
Nasale
Nasale
Orale
Spontanée
06/12/2012
2606/12/2012
Anatomical Basis of Sleep-Related Breathing
Abnormalities in Children With Nasal Obstruction
Yehuda Finkelstein
ARCH OTOLARYNGOL HEAD NECK SURG/VOL 126, MAY
2000
Fille 15 ans opérée des végétations à l’âge de 3ans
ON par rhinite atopique
Anatomical Basis of Sleep-Related Breathing
Abnormalities in Children With Nasal Obstruction
Yehuda Finkelstein
ARCH OTOLARYNGOL HEAD NECK SURG/VOL 126, MAY
2000
Overjet (surplomb)
Overbite (béance-ouverture antérieur)
Os hyoïde dorsiflexion de langue
Classe II
Fermeture angle base du crâne
2706/12/2012
Traitement
Existe-t-il des éléments
prédictifs cliniques
impliquant la
participation des V.A.
et Amygdales ?
2806/12/2012 Obstructive sleep apnea syndrome due to adenotonsillar hypertrophy in infants Michal Greenfeld L’idée est de déterminer les enfants apnéiques uniquement dus à HAVA et âgés de
06/12/2012
Facteur de risque de persistance de
SAOS post-opératoire
• Obésité 88% AHI ≥1/h
75% AHI≥2/h
51%≥5/h
OR 3,2 à 4,1
• IAH
• Age06/12/2012
Obesity and Obstructive Sleep Apnea
obesity
PROCEEDINGS OF THE AMERICAN THORACIC SOCIETY VOL 5 2008 Schwartz, Patil, Laffan, et al
The Correlation Among Obesity, Apnea- Hypopnea
Index, and Tonsil Size in Children
CHEST 2006; 130:1751
3106/12/2012
Relative Contributions of Body Mass Index and Adenotonsillar
Hypertrophy
Non obèse Obèse
Ehab Dayyat, Leila Kheirandish-Gozal, CHEST 2009; 136:137–144
Poids et post op
3206/12/2012
Relative Contributions of Body Mass Index andAdenotonsillar
Hypertrophy
Pour un IAH non différent entre O et NO il faut tenir compte de la taille des A = plus petites
Young
Old
Conclusion : l’explication physiopathologique du SAS chez
l’O. tient plus de l’infiltration graisseuse que de
l’hypertrophie des AA
Ehab Dayyat, Leila Kheirandish-Gozal, CHEST 2009; 136:137–144
Effect of Obesity and Medical Comorbidities on Outcomes After
Adjunct Surgery for Obstructive Sleep Apnea in Cases of
Adenotonsillectomy Failure
Conclusions Lingual tonsillar hypertrophy and
occult laryngomalacia are 2 important causes of
residual OSAS after adenotonsillectomy.
However, they tend to affect distinct
populations of children, and though appropriate
surgical correction can improve AHI, cure rates
are significantly worse for overweight children
undergoing lingual tonsillectomy and for
children with medical comorbidities undergoing
supraglottoplasty.
Dylan K. Chan Arch Otolaryngol Head Neck Surg. 2012
3306/12/2012
Facteur de risque de persistance de
SAOS post-opératoire
• Obésité 88% AHI ≥1/h
75% AHI≥2/h
51%≥5/h
OR 3,2 à 4,1
• IAH
• Age06/12/2012
Magnetic Resonance Imaging of the Upper Airway Structure
of Children with Obstructive Sleep Apnea Syndrome
RAANAN ARENS, ALLAN I. PACK Am J Respir Crit Care Med Vol 164. 2001
Outcomes of Adenotonsillectomy in
Patients With Prader-Willi Syndrome
• Six of our patients were girls (46%); 8 had genetic characteristics
consistent with deletion (61%), and the remaining 5 had genetic
characteristics consistent with uniparental disomy (39%). The median age
at T&A was 3 years (age range, 6 months to 11 years), and the median age
at start of growth hormone treatment was 8.5 months (range, 2 months
to 6 years). Nine of the 13 patients had mild to moderate obstructive sleep
apnea (OSA) or obstructive hypoventilation (69%); in 8 of these 9,
breathing normalized after T&A. Four children had severe OSA prior to
surgery (31%). Breathing normalized in 2 of these after surgery, but 2 had
PSG findings of residual combined obstructive and central apneas
postoperatively.
• Conclusions Adenotonsillectomy, while effective in most children with
PWS who demonstrate mild to moderate OSA, may not be curative in
children with severe OSA. An increase in central apneas can occur in some
children with PWS postoperatively, and it is important to repeat PSG after
surgery. Further studies are necessary to determine optimal treatment for
some children with PWS and sleep-disordered breathing.
Stacy L. Meyer Arch Otolaryngol Head Neck Surg. 2012
3506/12/2012
Facteur de risque de persistance de
SAOS post-opératoire
• Obésité 88% AHI ≥1/h
75% AHI≥2/h
51%≥5/h
OR 3,2 à 4,1
• IAH
• Age06/12/2012
Facteur de risque de persistance de
SAOS post-opératoire
• Obésité 88% AHI ≥1/h
75% AHI≥2/h
51%≥5/h
OR 3,2 à 4,1
• IAH
• Age06/12/2012
Adenotonsillectomy and obstructive sleep apnea in
children: A prospective survey
207 enfants 14 ans ayant subi une AA dont 199 1
intégrés dans l’étude avec PSG = 97 échecs
2
Échecs sont
Mallampati 3 ou 4
Rétrognathie
Hypertrophie des cornets
inférieurs 3+
Déviation de la cloison 3
4
Christian Guilleminault Otolaryngology–Head and Neck Surgery, 2007
Amygdales palatines
3806/12/2012
L’amygdalectomie
• Amygdaloadénoïdectomie indiscutée
• Adénoïdectomie-seule discutée
• Contre indications avec entre autres la division palatine
sous muqueuse et adénoïdectomie
• Effets secondaires douleur, dysphagie , amaigrissement
• Rares complications graves : hémorragie, sténose
pharyngée, incompétence, mort
• P.S.G. post opératoire ?
• 226% dépenses supplémentaires
• Ambulatoire vs Hospitalisation si IAH≥10/h ou
SO²60mm Hg
3906/12/2012
Amygdalectomie partielle
• Résultats controversés
• Tunkel et al 93% IAH≤1
• 0,5% à 16 % de récidive
• Repousse à 3,8 année !!!!!
• Nécessite d’être plus vigilant au long cours
(surveillance post-opératoire)
Amygdalectomie pour S.A.S.
Quid de la littérature ?
• 80% de bons résultats
Mitchell RB. Adenotonsillectomy for obstructive sleep apnea in children: outcome evaluated by pre- and postoperative
polysomnography. Laryngoscope 2007;117:1844–1854.
Montgomery-Downs HE, O’Brien LM, Gulliver TE, Gozal D. Polysomnographic characteristics in normal preschool and early
school-aged children. Pediatrics 2006;117:741–753. (l’indication n’est que rarement posée devant ces résultats)
• 45 et 75% dans certaines études en récidive
Guilleminault C Adenotonsillectomy and obstructive sleep apnea in children: a prospective survey. Otolaryngol Head Neck
Surg 2007;136:169– 175
Tauman R, Persistence of obstructive sleep apnea syndrome in children after adenotonsillectomy. J Pediatr 2006;149:803–
808.
• Récidives plus tardives
Guilleminault. Morphometric facial changes and obstructive sleep apnea in adolescents. J Pediatr 1989;114:997–999.
• Prediction : des enfants recidivants noirs , obèses, histoire familiale , recul de 5,5±4,6 ans
Morton Predictors of sleep-disordered breathing in children with a history of tonsillectomy and/or adenoidectomy. Sleep
2001;24:823
Conclusion
Etude des traitements associés à l’amygdaloadénoïdectomie autres que
chirurgie craniofaciale , trachéotomie , prise en charge de l’obésité
4006/12/2012
The effectiveness of tonsillectomy and adenoidectomy in the
treatment of pediatric obstructive sleep apnea/hypopnea
syndrome: A meta-analysis
14 études retenues de niveau 4
Forest plots
Variation de l’IAH post-op.
Pre=16,8
Post =2,42
Δ = 13,92
13,92
Scott E. Brietzke Otolaryngology–Head and Neck Surgery (2006)
The effectiveness of tonsillectomy and adenoidectomy in the
treatment of pediatric obstructive sleep apnea/hypopnea
syndrome: A meta-analysis
14 études retenues de niveau 4
Forest plots
% succès post-op.
82,9%
82,9%
Scott E. Brietzke Otolaryngology–Head and Neck Surgery (2006)
4106/12/2012
The effectiveness of tonsillectomy and adenoidectomy in the
treatment of pediatric obstructive sleep apnea/hypopnea
syndrome: A meta-analysis
14 études retenues de niveau 4
Forest plots Hedge’s
Réduction IAH après AA
Si > 1 = bon
1,43
Scott E. Brietzke Otolaryngology–Head and Neck Surgery (2006)
The effectiveness of tonsillectomy and adenoidectomy in the
treatment of pediatric obstructive sleep apnea/hypopnea
syndrome: A meta-analysis
14 études retenues de niveau 4
Conclusion
100% des enfants AA ne sont pas totalement guéris
La vigilance doit être accrue concernant la guérison putative
Repérer les SAS post-op (ne pas penser qu’après AA = guérison)
PSG chez les SAS compliqués : neuromusculaires
obèses
cranio-faciaux
trisomie 21
Penser à HAVA, race, dimension des VADS , sexe , âge pour évaluer les
enfants
Scott E. Brietzke Otolaryngology–Head and Neck Surgery (2006)
4206/12/2012
Updated systematic review of tonsillectomy and adenoidectomy for treatment
of pediatric obstructive sleep apnea/hypopnea syndrome
1079 patients ≤ 18ans (âge moyen = 6,5)
IAH 18,6 4,9
↘ de 12,4 /h
12,4
Michael Friedman,
Otolaryngology–Head and Neck Surgery (2009)
Updated systematic review of tonsillectomy and adenoidectomy for treatment
of pediatric obstructive sleep apnea/hypopnea syndrome
1079 patients ≤ 18ans (âge moyen = 6,5)
IAH06/12/2012
Updated systematic review of tonsillectomy and adenoidectomy for treatment
of pediatric obstructive sleep apnea/hypopnea syndrome
1079 patients ≤ 18ans (âge moyen = 6,5)
IAH06/12/2012
Adenotonsillectomy Outcomes in Treatment of Obstructive
Sleep Apnea in Children
A Multicenter Retrospective Study
Measurements and Main Results: Data from 578 children (mean age, 6.9 ± 3.8 yr) were
analyzed, of which approximately 50% of included children were obese. AT resulted in a
significant AHI reduction from 18.2 ± 21.4 to 4.1 ± 6.4/hour total sleep time (P < 0.001). Of the
578 children, only 157 (27.2%) had complete resolution of OSAS (i.e., post-AT AHI 7 yr) or obese children. In addition, the presence of severe OSAS in
nonobese children or of chronic asthma warrants post-AT nocturnal polysomnography, in view of
the higher risk for residual OSAS.
American Journal of Respiratory and Critical
David Gozal Care Medicine Vol 182. pp. 676-683, (2010)
Adenotonsillectomy Outcomes in Treatment of Obstructive Sleep Apnea in Children
A Multicenter Retrospective Study
50,6% obèses
576 e-7a-50%obèses-IAH(184)-157
guéris-pejoratifs = âge+IMC et asthme
et preIAH chez les non obèses
Rakesh Bhattacharjee Am J Respir Crit Care Med Vol 182. , 2010
4506/12/2012
Qu’attendre d’une intervention sur
les amygdales en dehors des effets
sur la respiration pendant le
sommeil ?
Metabolic Alterations and Systemic Inflammation inObstructive Sleep
Apnea among Nonobese and Obese Prepubertal Children
David Gozal
Après AA la correction du SAS induit une baisse significative des
lipides et des marqueurs inflammatoires
Am J Respir Crit Care Med Vol 177. pp 1142–1149, 2008
4606/12/2012
Plasma Adhesion Molecules in ChildrenWith Sleep-Disordered
Breathing*
Molécule d’adhésion Louise M. O’Brien
intracellulaire P-selectine bio marqueur activation plaquettaire
ME
39 SAS>5/h
47 106/12/2012
Proprioception muqueuse pharyngée postérieure
1,5
3,5
4,5
Guilleminault et al. 122 (3): 866. (2002)
Growth and Biochemical Markers of Growth in Children With Snoring and
Obstructive Sleep Apnea
Peter Nieminen, Tuija Löppönen, Uolevi Tolonen, Peter Lanning, Mikael Knip,
and Heikki Löppönen
Pediatrics, Apr 2002;
4806/12/2012
Effets cardio-vasculaires chez enfant
Cardiovascular Complications of Obstructive Sleep Apnea Syndrome:
Evidence from Children
Rakesh Bhattacharjee
Enfant 8ans non obèse IAH5
Retard de reperfusion ( artère
radiale – métacarpienne ) doppler
Progress in Cardiovascular Diseases, Vol. 51, No. 5 (March/April), 2009:
PERSISTENCE OF OBSTRUCTIVE SLEEP APNEA SYNDROME IN
CHILDREN J Pediatr 2006;149:803-8
AFTER ADENOTONSILLECTOMY
RIVA TAUMAN
Obèses Non-obèses
Post amygdalectomie
L.M. O'Brien Obesity increases the risk for persisting obstructive sleep apnea after
treatment in children, Int J Pediatr Otorhinolaryngol 70 (2006),
77,5% guerison non obèse et 45% obèse
Mitchell and J. Kelly, Outcome of adenotonsillectomy for severe obstructive
sleep apnea in children, Int J Pediatr Otorhinolaryngol 68 (2004)
4906/12/2012
Adenotonsillectomy for obstructive sleep apnea in obese children: A meta-analysis
Dary J. Costa, MD
Otolaryngology–Head and Neck Surgery, 2009
IAH ≠ pre/post-op
Nadir SaO² ↗pre/post-op
Amélioration sans totale guérison
Cognition, sleep and respiration in at-risk children treated for obstructive sleep apnoea
H.E. Montgomery-Downs Eur Respir J 2005; 25: 336–342
Les enfants préscolaires sont améliorés en postopératoire qualité sommeil et cognition sans
jamais atteindre les contrôles
5006/12/2012
Adenotonsillectomy Improves Neurocognitive Function in
Children with Obstructive Sleep Apnea Syndrome
ns
Les fonctions cognitives sont améliorées après AA ce qui marque leur caractère réversible
Bat-Chen Friedman SLEEP 2003;26(8):999-1005
Traitement nasal
5106/12/2012
Upper airway resistance syndrome: effect of nasal
dilation, sleep stage and sleep position.
La dilatation nasale ↘ stade 1
↘ temps de désat
Bahammam A, Tate R, Mangreda J, et al Sleep 1999; 22:592–598
Effect of improved nasal breathing on obstructive sleep apnea
Summary of PSG results before and after nasal
surgery for OSA Chirurgie nasale
Subjectivement amélioration
-respiration nasale 98%
-énergie diurne ↗78%
inchangé ou aggravé 22%
CPAP titration levels before and after nasal surgery -ronflement ↘ou=0 34%
for OSA inchangé 66%
2 corrections
P° PPC
↘ SaO²
MICHAEL FRIEDMAN, Otolaryngology–Head and Neck Surgery January 2000
5206/12/2012
Efficacy of fluticasone nasal spray for pediatric obstructive sleep apnea
Robert T. Brouillette
Ratio VG/choanes
0,99 0,75
5306/12/2012
Nasal Obstruction in Children with Sleep-disordered
Breathing
Sullivan, Kasey Li, Ch. Guilleminault
Meilleurs résultats dans le
groupe AA+RF(1,3) lorsque
recommandée
Que sans RF (3,5)
Annals Academy of Medicine August 2008,Vol. 37 No. 8
Changes in dentofacial morphology after adeno-/tonsillectomy in young children with
obstructive sleep apnoea — a 5-year follow-up study
Zettergren-Wijk, L. et al . Eur J Orthod 2006 28:319
5406/12/2012
Skeletal effects to the maxilla after rapid maxillary expansion
assessed with cone-beam computed tomography
Garrett et al American Journal of Orthodontics and Dentofacial Orthopedics July 2008
Am J Orthod Dentofac Orthop 107;268,
1995
5506/12/2012
Rapid Maxillary Expansion in Children with Obstructive
Sleep ApneaSyndrome
Paola Pirelli SLEEP,Vol. 27, No. 4, 2004
SAS et antileucotriènes
• L’association nasocorticoïdes et
ALT(montelukast) chez des SAS entre 1-5
augmente la guérison définitive en post
amygdalectomie
Kheirandish L, Intranasal steroids and oral leukotriene modifier therapy in residual
sleep-disordered breathing after tonsillectomy and adenoidectomy in children.
Pediatrics 2006;117:e61
Goldbart AD Leukotriene modifier therapy for mild sleep-disordered breathing
children. Am J Respir Crit Care Med 2005;172:364–370 .
5606/12/2012
« Une forêt d’arbres décisionnels »
Sans jamais oublier les éléments du raisonnement clinique que sont
1. La puissance thérapeutique de la PPC même chez l’enfant
2. La place de la somnolence diurne excessive et ses répercussions neurocognitives
sur un cerveau en constante évolution
3. La présence d’une obésité ou Sd Métabolique de plus en plus marquée en
Europe
4. Les antécédents familiaux cardio-vasculaires qui imposent un suivi à long terme
5. La place de l’ORL valeur ajoutée indispensable due à la prise de décision
thérapeutique
6. La place de l’ODF qui par son action « interceptrice » va permettre d’augmenter
le volume des voies aérodigestives supérieures et donc de diminuer la résistance
au passage
7. L’urgence du traitement permettant de prevenir l’installation du SAOS de l’adulte
qu’il est bien difficile de traiter
Childhood Obstructive Sleep Apnea: One or Two Distinct Disease Entities?
Sleep Med Clin 2 (2007) 433–444 Ehab Dayyat, , Leila Kheirandish-Gozal, , David Gozal,
5706/12/2012
Childhood Obstructive Sleep Apnea: One or Two Distinct Disease Entities?
Ehab Dayyat, MD, Leila Kheirandish-Gozal, MD, David Gozal, MD*
Sleep Med Clin 2 (2007) 433–444
Associations between sleep-disordered breathing symptoms and facial and dental
morphometry, assessed with screening examinations
Symptomatologie pédiatrique
Nuit Jour
• Position de sommeil bizarre • Respiration buccale
• Ronflement permanant et fort
• Eveils confusionnels • Soif matinale
• Endormissement difficile • SDE ou fatigue
• Eveils difficiles
• Enurésie
• Timidité , dépression
• Bave • Troubles comportementaux
• Respiration buccale • TADH
• Migraines
• Sueurs • Agressivité
• Mps • Irritabilité
• Somniloquie
• Somnambulisme • Deficit apprentissage
• Pauses constatées • Deficit academique
Nelly T. Huynh Am J Orthod Dentofacial Orthop 2011
5806/12/2012
Croissance faciale = les facteurs de
modification
Déviation
cloison nasale
Diminution
Écoulement orifices
postérieur piriformes
Hypertrophie Baisse flux nasal
amygdales et
végétations
Extension de la
Position basse de Respiration tête
langue buccale
Étroitesse maxillaire Position basse de
mandibule
Ronflement
Enfant ronfleur Pauses
+ Sommeil agité
Tb cognitifs
Cassure courbe poids
Grosses amygdales
Symptômes Cœur et poumon
normal
évoquant SAS
- -
Anomalies cranio-
+ Continuer
l’examen
faciales Présence classique
Trisomie facteur de complet
Maladie
neuromusculaire
risque +
Hypoventilation - Recherche
Maladie métabolique Il y a-t-il un
SAOS
risque cardio-
vasculaire ?
Spécialiste (orl,pneumo,
neuro...)
Exploration cardio-
vasculaire
5906/12/2012
Recherche
SAOS
+ Ambulatoire PV
Oxymétrie
PSG gold st+++
Enregistrement audio
Enregistrement de sieste
+
PSG>0
+ +
Obésité
Clinique sommeil
Amygdales
spécialisé
+
Traitement médical06/12/2012
Respiration buccale exclusive
Dysmorphose dento-squelettique
Traitement ODF
Traitement ORL médical et/ou chirurgical
Traitement ORL
Associations between sleep-disordered breathing symptoms and facial and dental
morphometry, assessed with screening examinations
vertical
transversal
Nelly T. Huynh Am J Orthod Dentofacial Orthop 2011
6106/12/2012
Neck circumference and other clinical features in
the diagnosis of the obstructive sleep apnoea
syndrome
Robert J 0 Davies, Nabeel J Ali, John R Stradling
Thorax 1992;47:101-105 Neck
Snoring Predicts Hyperactivity Four Years Later
Le suivi sur 4 ans montre que le ronflement et
autres symptomes évoquant un trouble
respiratoire du sommeil (TRS) sont des facteurs
de risque forts pour voir émerger une
hyperactivité ou la voir s’aggraver
Ces éléments confirment bien que le non
traitement des TRS contribue à l’aggravtion ou
le developpement d’une hyperactivité
Ronald D. Chervin SLEEP, Vol. 28, No. 7, 2005
6206/12/2012
Young T, Palta M, Dempsey J, et al. The occurrence of sleep-disordered breathing
among middle-aged adults. N Engl J Med 1993; 328:1230–1235
Davies R, Stradling J. The epidemiology of sleep apnea. Thorax 1996; 51(suppl 2):S65–
S70
≥4% ≥3%
obésité
+20%
+20% croyant que ≥4% était trop haut
Obésité = l’auteur a augmenté les chiffres croyant que
sa cohorte était plus maigre que celle des USA et
c’était faux
La participation de la SDE est peu
fréquente
Does nasal decongestion improve obstructive
sleep apnea?
J. Sleep Res. (2008) 17, 444–449
6306/12/2012
Metabolic Alterations and Systemic Inflammation in Obstructive Sleep
Apnea among Nonobese and Obese Prepubertal Children
SAS n’induit pas de RI chez les enfants non obèses OSA mais semble jouer un rôle important chez les obèses
L’amélioration significative du profil lipidique,CRP et apolipoprotéineB après AA dans les 2 groupes semble dire que le SAS
joue un rôle pathogénique certain dans l’homéostasie lipidiqueet le système inflammatoire indépendamment de l’obésité
David Gozal1 and Leila Kheirandish-Gozal A J R C C M Vol 177. pp 1142–1149, 2008
C-reactive Protein, Obstructive Sleep Apnea, and Cognitive
Dysfunction in School-aged Children
0,48(SAS+TNC)0,21(SAS-TNC)
0,18 (non SAS)0,36 (SAS)
Enfants ronfleurs SAS
non SAS
SAS neurocognitifs (TNC)
non neurocognitifs
CRP est plus haute
SAS + TNC
Leila Kheirandish-Gozal Am J Respir Crit Care Med Vol 176. pp 188–193, 2007
6406/12/2012
Cardiovascular Morbidity in Obstructive Sleep Apnea Oxidative Stress,
Inflammation, and Much More Am J Respir Crit Care Med Vol 177. pp 369–375, 2008
David Gozal and Leila Kheirandish-Gozal
Metabolic Alterations and Systemic Inflammation in Obstructive Sleep
Apnea among Nonobese and Obese Prepubertal Children
HTA et SAOS chez l’enfant
Marcus CL, Greene MG, Carroll JL. Blood pressure in children with obstructive sleep apnea.
Am J Respir Crit Care Med 1998;157:1098– 1103.
Amin RS, Carroll JL, Jeffries JL, Grone C, Bean JA, Chini B, Bokulic R, Daniels SR. Twenty-four-
hour ambulatory blood pressure in children with sleep-disordered breathing. Am J Respir Crit
Care Med 2004;169:950–956.
Enright PL, Goodwin JL, Sherrill DL, Quan JR, Quan SF; Tucson Children’s Assessment of Sleep
Apnea Study. Blood pressure elevation associated with sleep-related breathing disorder in a
community sample of white and Hispanic children: the Tucson Children’s Assessment of
Sleep Apnea Study. Arch Pediatr Adolesc Med 2003;157:901– 90
David Gozal Am J Respir Crit Care Med Vol 177. pp 1142–1149, 2008
6506/12/2012
Metabolic Alterations and Systemic Inflammation in Obstructive Sleep
Apnea among Nonobese and Obese Prepubertal Children
Hypertrophie ventriculaire
gauche et SAOS chez l’enfant
Amin RS, Kimball TR, Kalra M, Jeffries JL, Carroll JL, Bean JA, Witt SA, Glascock BJ, Daniels SR. Left ventricular function in
children with sleep-disordered breathing. Am J Cardiol 2005;95:801–804
Vit passage v. mitrale
David Gozal Am J Respir Crit Care Med Vol 177. pp 1142–1149, 2008
Metabolic Alterations and Systemic Inflammation in Obstructive Sleep
Apnea among Nonobese and Obese Prepubertal Children
HTA et SAOS chez l’enfant
Marcus CL, Greene MG, Carroll JL. Blood pressure in children with obstructive sleep apnea.
Am J Respir Crit Care Med 1998;157:1098– 1103.
Amin RS, Carroll JL, Jeffries JL, Grone C, Bean JA, Chini B, Bokulic R, Daniels SR. Twenty-four-
hour ambulatory blood pressure in children with sleep-disordered breathing. Am J Respir Crit
Care Med 2004;169:950–956.
Enright PL, Goodwin JL, Sherrill DL, Quan JR, Quan SF; Tucson Children’s Assessment of Sleep
Apnea Study. Blood pressure elevation associated with sleep-related breathing disorder in a
community sample of white and Hispanic children: the Tucson Children’s Assessment of
Sleep Apnea Study. Arch Pediatr Adolesc Med 2003;157:901– 90
David Gozal Am J Respir Crit Care Med Vol 177. pp 1142–1149, 2008
6606/12/2012
Blood Pressure in Children with Obstructive Sleep Apnea
L’IAH est moins significatif que le IMC
Les enfants SAS et PS ont une TA >
enfants contrôles
La diastolique est plus élevée chez le
SAS
CAROLE L. MARCUS AM J RESPIR CRIT CARE MED 1998;157:1098–1103
LONG-TERM FOLLOW-UP OF NEUROCOGNITIVE PERFORMANCE IN
CHILDREN WITH SLEEP DISORDERED BREATHING
Method. In a sample of 27 frequently snoring children aged 3-12 years and referred
for AT due to suspected SDB and 32 non-snoring control children matched for age
and gender, neurocognitive performance and polysomnography was reported at
baseline, 6 month
follow-up (and after AT for SDB children) and 4 year
ollow-up.
Results. Results show significant deficits across all threetime points in SDB children
relative to controls in general intelligence, executive function, and language skills. In
contrast, initial improvement in visuospatial ability in SDB children was maintained at
4 year followup.
Conclusion. The long-term neurocognitive deficits observed raise concern regarding the
effectiveness of AT in correcting neurocognitive deficits in children with SDB. The results also
raise the question as to the optimal timing and treatment for SDB as well as the need for
alternative or complimentary treatment strategies.
Kohler MJ
6706/12/2012 Cardiovascular Disease and Sleep Disordered Breathing: Are Children Vulnerable? Commentary on O’Driscoll et al. Acute cardiovascular changes with obstructive events in children with sleep disordered breathing. SLEEP 2009;32:1265-71. Contradictions L’association de P°
06/12/2012
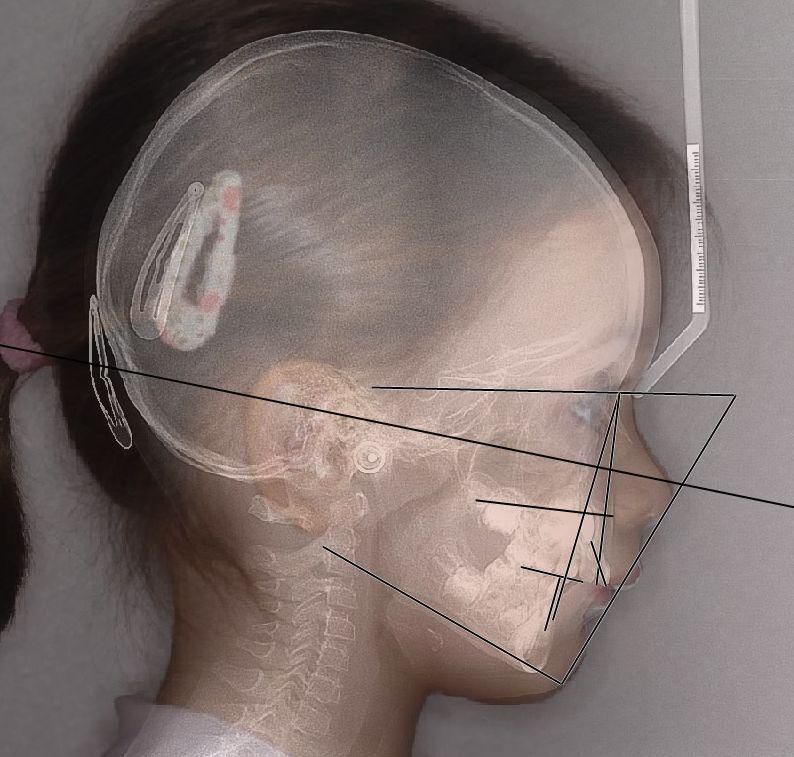
Plan facial
FX angle axe facial
FD angle profondeur
faciale 29 enfants (LFH)
-arc mandibulaire > (MA)
-hauteur faciale totale>(TFH)
Axe facial
69Vous pouvez aussi lire