Explorations fonctionnelles en cardiologie congénitale et pédiatrique - Antoine Legendre DU de Cardiologie Pédiatrique 2019-2020 - f-static.net
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous

Explorations fonctionnelles en
cardiologie congénitale et
pédiatrique
Antoine Legendre
DU de Cardiologie Pédiatrique
2019-2020
Epreuve d’effort chez l’enfant Particularités
Avant: • Détendre l’enfant (parfois un peu de musique), calmer les hyperactifs… • Présence des parents : avantages et inconvénients… perso à priori sans les parents • Demander le niveau d’activité physique • Faire cracher les schweemgums • Pour les tous petits en faire un jeu • en faire un challenge, un plaisir, valoriser • Pour les réfractaires : expliquer l’enjeu… • Pour les plus jeunes : peu d’explication avant, on explique pendant • Adapter la taille du pédalier, hauteur de selles, taille du brassard • Si tapis : trop petit pour le velo (1m/20) ou ne sait pas pédaler (
Pendant: • Expliquer le pédalage avec rythme régulier : un vrai challenge • Fréquence de pédalage élevé entre 70 et 90 tr/mn • Coaching +++ • Bien valoriser • Apprendre à respirer, • Poser les questions sur les éventuels symptômes • Essayer d’atteindre au moins 85 % de la FMT • Rampe plutôt que paliers pour les moins de 10 ans • Faut pas que ça dure trop < 8 mn • Accélérer sur la fin ! Le sprint final après une mini pause éventuellement • Tapis : De 4 km/h jusqu’à 8-9 km/h avec pente de 4 à 7 % sur 5-6 min Apres: • Valoriser – féliciter. • Médaille pour les tout petits! • Puis la torture d’enlever les électrodes
Particularités du test d’effort chez l’enfant Vélo • à partir d’1m20 (7 ans) (2 selles) • selon l’âge, le sexe et la pratique d’un sport scolaire et en club • Echauffement de 15 à 40 watt • Incrément de 5 à 20 watt/min • Vitesse de pédalage : en général > 70 tr/min (< 90 tr/min) Tapis roulant • en général (4 à 6-7 ans) (pas de VO2, ECG de mvse qualité) De 4 km/h jusqu’à 8-9 km/h avec pente de 4 à 7 % sur 5-6 min VO2 max normes enfant : équation de Cooper Ped Research 1984

Test d’effort Risque 2500 tests • pas d’évenement grave (Tutarel 2013) 1375 tests : • arrêt du test pour arythmie dans 2,5 % des cas, • ST élévation ,0,5% • désaturation : 0,2 %) (Inuzuka 2012)
ECG d’effort
Pas de pathologie connue
A qui ?
• Symptômes Interrogatoire de l’enfant peu fiable: dès qu’il y a notion d’effort au sens large au sens large : douleur thoracique,
palpitation, malaise
• Même si échocardiographie normale
Pour voir quoi ?
• Trouble du rythme à l’effort :
• ESV/ESA salves d’effort
• Sous décalage de ST à l‘effort
• Trouble de conduction à l’effort
• Intolérance à l’effort
• Profil TA
• QT long ? (recup 6 min)
Pour dépister quoi ?
• Anomalie de naissance de la coronaire
• Myocardiopathie débutante
• Trouble du rythme à l’effort
• TVC
• HTA
99,…% des cas : normale, ne sait pas respirer sensation de cœur qui bat fort,
hyperventilation inadaptée…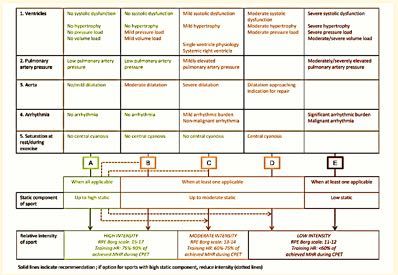
ECG d’effort Rythmologie • ESV bénignes ou malignes • Trouble de conduction supra-hissien ? • Maladie sinusale : accélération à l’effort • Pre-éxcitation maligne ou bénigne • QT long : 6’ de récup • Beta-bloquage • Pace maker •…
ECG d’effort Dépistage – suspicion échographique • Dépistage DVDA / QT long… • Suspicion d’anomalie coronaire : naissance ou trajet
Anomalies de trajet
• Peu contributive pour dépister une anomalie de naissance
• Peu contributive pour décision de réparer
• En général chirurgie systématique en cas de symptômes et/ou d’ischémie
prouvée et/ou de trajet inter aortico pulmonaire de la coronaire gaucheALCAPA
Test d’effort
Séquelles coronaires post chirurgicales
Réimplantation des coronaires : switch, ross, ALCAPA…
SWICH ARTERIEL ROSSEvènements coronaires après switch
artériel
Ou JTCS 20013,
Legendre Circulation 2003
Raimondi JACC imaging 2018post switch artériel
Recherche d’ischémie
Legendre circ 2003Test d’effort
Profil TA -coarctation opérée
HTA
- Les patients opérés d’une coarctation ont plus de risque d’être hypertendus
quelle que soit la qualité de la réparation
- Difficulté à définir l’HTA d’effort chez l’enfant
- Arche gothique : facteur de risque d’HTA d’effort ?
- HTA d’effort dépiste t-elle l’HTA ou prédit elle une HTA future ?COURBE DE SURVIE APRES CURE DE
COARCTATION
100
90
Pourcentage de survie
80 Cause de décès tardif Nbre
70 Coronaropathie 10
60 Réintervention chirurgicale 7
50 Dissection aortique 6
40 Mort subite 7
30 Accident de la route 3
20 Autres 7
10 Inconnues 5
0
5 10 15 20 25 30 35 40 45 50
Années après chirurgie
Toro-Salazar OH Am j Cardiol 2002Coarctation opérée
• Arche gothique
Facteur de risque d’HTA d’effort et HTA (MAPA)
Ou JTCS 2006,
Donavazzan World Journal for
Pediatric and Congenital Heart
Surgery 2014Coarctation opérée
HTA d’effort chez l’enfant et adulte jeune
• James et al Circulation 1980
• Sieira et al apunt med sport 2010
• Becker Arq Bras Cardiol 2007Coarctation opérée
• HTA d’effort : pathologie ou pre pathologie
Luijendijk Am J Cardiol 2011HTA d’effort et sport • Profil TA normal : surveillance EE tous les 2 ans • Profil TA anormal : MAPA 24 h, • Recoarctation ? à scanner, IRM, KT à dilatation ? • Traitement ? IEC, BB si anomalie fonction morpho cardiaque ? • Eviction des sports à forte composante statique, compétition • Répéter l’EE et les MAPA ?
ECG d’effort
Rao et CMH
• Mauvaise adaptation tensionnelle : valeur pronostique
• RAO :
- Excès de post charge : bas débit
- Ischémie d’effort : bas débit +/- TDR
• CMH
- Trouble de la fonction diastolique / ischémie (TDR)
- Mauvaise adaptation des RVS
- Ischémie /TDR ventriculaire - auriculaireBicuspidie stenosante (14 ans)
FC Stroke volume
Gradient moyen 50 mmHg,
FE VG : 60%,
Hypertrophie modérée
Exercise
Augmentation PA
Pas d’ischémie
commisuroplastie
Gradient moyen
20 mmHgCardiopathies congénitales
Test d’effort cardiopulmonaire
(VO2max)Indications du test d’effort cardiopulmonaire • Vérifier et mesurer le symptôme d’intolérance à l’effort • Outils diagnostique • Outil pronostique • Envisager une grossesse • Aide à la décision thérapeutique • Outil de réhabilitation cardiaque
Test cardiopulmonaire
Vérifier et mesurer le symptôme d’intolérance à l’effort
• Difficulté pour le patient d’apprécier lui-même son degré
d’intolérance à l’effort (controversé)
• Bonne corrélation avec la classe NYHA et correspondance avec
patient en insuffisance cardiaque chronique
• Mesure avec valeur continue (VO2max) plutôt que par classe
Gratz 2009Guidelines 2018
• AHA Guidelines 2018
(Stout circulation 2018)Kempny EHJ 2012
Mais !!
• Quel est l’intérêt de cantonner des patients avec une certaine
cardiopathie à normalité une VO2 max spécifique? Alors même que:
• Les lésions sont extrêmement variables d’un pt à l’autre au sein d’un même
groupe
• Les indications de traitement/prise en charge de ces patients/ lésions résiduelles
doivent/sont sans cesse améliorée… pour augmenter la VO2 ?
• Les patients connus pour être sédentaires
Mieux vaut affiner les outils de détections des facteurs limitants de la
VO2Test cardiopulmonaire
Diagnostic
Shunt Droite – Gauche à l’effort
• Par CIA/PFO par défaut de compliance du VD
• VD défaillant (Fallot),
• VD restrictif (APSI, SVP…),
• Ebstein…
Hyperventilation : augmentation de VE/VCO2
Desaturation
Diminution de la Pet CO2Test cardiopulmonaire valeur pronostique • Pic de VO2 (< 64% th) • Reserve de FC (> 71/min) • Saturation de repos • Baisse de la saturation à l’effort de plus de 5% • Pente VE/VCO2 (non cyanosé) (39) • Seuil ventilatoire • Âge
Test cardiopulmonaire
valeur pronostique
Diller 2005Test cardiopulmonaire valeur pronostique
Inuzuka 2012
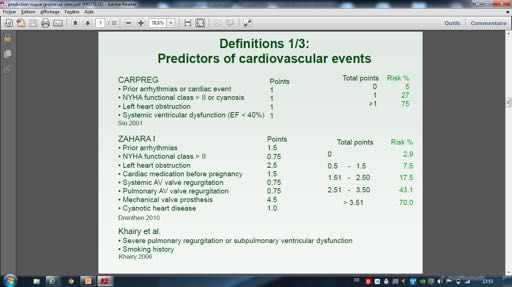
Grossesse : prédiction du risque
• VO2max < 22, FC max
zation laboratories index ≥160 specially mL/m equipped
, or RV with devices volume
end-systolic may be applied in an
e and tools used in ACHD intervention are needed 9. Although correction ofatrial the hemodynamic
arrhythmia, lesion
and no contraindications
Test cardiopulmonaire
index ≥80 mL/m 2
, or RV end-diastolic volume perPR), year), and unfa- egies collectively app
6. There are data that indicate that pulmonary valve maylead-related
be clinically complications,
to anticoagulation.
- and personnel trained in their use. Such equipment (ie, beneficial, pulmonary outcome compared w
replacement ≥2x LVperformed end-diastolic volume).
prior to specific ventric- vorable
valve patient-reported
replacement 12. Catheteroutcomes,
alone ablation can be useful
has not including
consistentlyin adults im-
. Fontan surgery has
AND GUIDELINES
and expertise RVdiffer from those found in RVOT
catheteri-
ular c. issystolic pressure due to obstruction after Fontan palliation with intra-atrial
- size associated with normalization of RV paired
been QoL,C-LD
IIademonstrated anxiety,todepression, reduce
reentrant risk of
tachycardia and psychosexual
or subsequent
focal atrial tion of atrial refracto
zation laboratories devotedpressure primarily to diagnostic
Décision thérapeutique
volumes. ≥2/3 systemic
However, it is not yet evident that this VT or SCD.S4.3.5-42S4.3.5-15,S4.3.5-17,S4.3.5-40
complications. Thus,tachycardia.
in addition to pulmonary S4.4.2-13–S4.4.2-15
c catheterization and coronary
Stout etd.al Progressive interventions. ring, and intra-atrial c
reduction in objective exercise valve replacement, VT 2018revision
13. surgery ACHD Guideline
and/or
surgery, ICD implan- or nus node dysfunction
e correlates
2. For patients tolerance with an improvement
at low or intermediate risk of obstruc- in mortality. 8. In patients with repaired
Fontan
arrhythmia
TOF and moderate
including
surgery as indicated, is
tation may PRbe considered. S4.3.5-43
surgery for during long-term follo
g tive Clinically,
coronary it increasing
Thedisease,
therefore CT coronaryisuse most compelling
of angiography
CMR in the long-
to per- greater who are undergoing
reasonable for adults cardiac
with atriopulmonary
d can form
be an pulmonary
pathways
term alternative
follow-up valve
is beyond
tofor replacement
the scope of these
cardiacpatients withif repaired
catheterization 2 of the fol-
guide-
4.3.6. aRight
TOF Recommendations separate lesion
IIa Ventricle–to-Pulmonary
for TOF (Continued) (eg,Fontan RVOT aneurysm, TR, branch has been associated
connections with recurrent
CLINICAL STATEMENTS
C-LD atrial tachyarrhythmias refractory to the single ventricle, in
lines but canS4.3.5-1,S4.3.5-9,S4.3.5-12–S4.3.5-14
be found elsewhere, such as the
e lowing are met: artery Artery PA stenosis,
Conduit residualpharmacological
VS D, arrhythmia ablation,
AND GUIDELINES
COR LOE Recommendations
for assessinghas provided
coronary
“PACES/HRS quantification
Expert course and
Consensus of patency.
Statementventricularon the size,
therapy and catheter
sure, reduced cardiac
ablation who have preserved systolic
a. Mild or moderate
function,
Recognition and and PR. RV
However,
Management or LV systolicthere isdysfunction
of Arrhythmias lack ofin con- Therapeutic coronary artery revascularization,
Recommendations for Right Ventricle–to-PA Conduit ventricular function and
aortic
severe atrial
root re- protein-losing entero
3.4.7. Exercise
b. Severe Testing
sensus
ACHD.” RV dilation
regarding
S4.3.4-21 optimal(RV end-diastolic
indications andvolume timing placement),
Referenced studies it may
that support
percutaneous)
be reasonable
5. Pulmonary valve replacement (surgical or
dilation.
recommendations
for relief of symptoms is
to concurrently
are summarized
S4.4.2-16–S4.4.2-18
atrial pacing may be f
7.ofSystemic
pulmonary valve
desaturation 2 replacement
and arrhythmias in this
are popula-
fre- perform
in Online Data Supplementpulmonary 44. valve with replacement. S4.3.5-41
pulmonary Fontan con
Recommendations index ≥160Testing
for Exercise mL/m , or RV end-systolic volume I B-NR
recommended
TOF and
for14.patients
moderate or greater
Pulmonary
PR to
repaired
vasoactive medications
with
can be
quently
tion. signs of worsening
Pulmonary valve replacement hemodynamics, results pro-in re- IIa B-R beneficial improve exercise capacity in
Referenced studies that support
index
gressive ≥80 recommendations
TR,mL/mor volume 2
, or RV
worsening are summarized volume
end-diastolic
RV function. Surgery
9. Although
COR Stout et al
LOE correction
Recommendations
cardiovascular symptoms of
adults the
not with
otherwise hemodynamic
Fontan repair. lesion cardiac lateral tunnels S4.4.2-19–S4.4.2-25
duction of RV and relief of PR; however,
pulmonary thrombotic complicati
Downloaded from http://ahajournals.org by on December 31, 2019
explained. S4.3.5-9–S4.3.5-11
in Online Data Supplement 11.
for the tricuspid valve as wellfor as outcomes.
closure of theMany (ie, PR), may be 15.
Diagnostic clinically
Antiplatelet beneficial,
therapy or anticoagulation
COR
≥2x LVRecommendations
these
LOEASD or
end-diastolic
are only surrogates volume).
stretched patent foramen ovale and ar-
6.
valve replacement
Pulmonary valve replacement
1. Coronary alone
with
(surgical
a vitamin
artery has
compression not
K antagonist testing consistently
may be
with
ular pacing may be p
or percutaneous) is reasonable for
c. RV patients
systolic with repaired
pressure due TOF to mayRVOT deny symptoms
obstruction Recommendations simultaneous
for Fontan consideredcoronary
Palliation in ofadults after
angiography
Single Fontan
Ventricle and tanselected
in compared with pla
patients,
rhythmia surgerywith can be cardiopulmonary
beneficial. When ar-
CLINICAL STATEMENTS
preservation
B-NR of ventricular size and function
yet 1. In patients
demonstrate ACHD,
reduced exercise tolerance. been IIb demonstrated towith reduce
palliation without risk
knownin of
orthesubsequent
suspected randomized
approach. studies de
S4.4.2-45,S4.4.2-46
Downloaded from http://ahajournals.org by on December 31, 2019
IIa B-NR Physiology (Continued)
in asymptomatic high-pressure
patients balloon
repaired dilation conduit
rhythmia
≥2/3 systemic surgery is required,
pressure canitbetypically
useful forinvolves a I B-NR
AND GUIDELINES
exercise testing 2018 ACHD
(CPET) Guideline
IIa Pulmonary
B-NR
modifiedbaseline valve
right atrial replacement
maze procedure. in such
In the pres-patients VT or SCD.
TOF and
COR dysfunction
S4.3.5-42
ventricular
LOE and moderate
Thus, thrombus,
enlargement
is indicated
Recommendations
in
before addition
thromboembolic
or right ventricle–to-PAto pulmonary
events, or prior
therapy.
mias is discussed in
S4.4.2-22,S4.4.2-23
th
functional assessment and serial conduit arrhythmia. or greater S4.4.2-26
d. Progressive
has
encebeen of AF,
reduction
associatedadditionwith
theS3.4.7-1,S3.4.7-2
testing.
in improved
of a left
objective
atrial Coxfunctional
exercise
Maze valve replacement,
PR.
stenting or transcatheter valve
VT surgery and/or ICD implan- Corticosteroids, See Section 3.3 sp
S4.3.5-1,S4.3.5-9,S4.3.5-12–S4.3.5-14
Diagnostic (Continued)placement.16. Reoperation or intervention for structural/
S4.3.6-1,S4.3.6-2
tolerance
status.
III S4.3.5-9,S4.3.5-10
procedure can be beneficial to reduce the risk tation 7.may
Primarybe considered.
prevention therapy isS4.3.5-43
ICDanatomic reasonable in a Fontan
abnormalities helpful
should for Fontan
perform surge pa
attributable to moderate or greater
2. In symptomatic patientsPR,with and ACHD, can a IIa B-NR 2. InTOF 10.
andItmultiple
patients maywith bestented
reasonable rightto ventricle–to-PA
perform
The
7. size of increasing
recurrent
Riskand/or
factors AF. use of CMR in the long- CLINICAL STATEMENTS in adults with risk factors
the
othersetting
proceduresof protei
in th
RVfor SCDtestinclude:
6-minute walk can be usefulistoRV objectively IIb C-LD palliated
conduitscatheterization
and worseningpatient with symptoms
in asymptomatic
PS or PR, evaluation or with
adults
improve
IIa RV C-LD function if there for SCD.
failure of thepalliation
Fontanshould
circulation
S4.3.5-15–S4.3.5-17
may be
AND GUIDELINES
dilation or term 8. The
a.follow-up
decreased
use
LV systolic of the
for
assess symptom bidirectional
patients
or diastolic cavopulmonary
withcapacity,
dysfunction
severity, functional repaired TOF 4.3.6. I Right 8. Ventricle–to-Pulmonary
IIb B-NR C-EO
for conduit after Fontan
complications to evaluate
be sponsive
ommendations to other on ther
dia
isRV ejection fraction. Surgical pulmonary valve replacement may
considered. S4.4.2-27
shunt much more to common in children than in performed, hemodynamics, oxygenation to
including fluoroscopy andevaluate
cardiac
has b. and
Nonsustained
provided response
quantification VT therapy.S3.4.7-3,S3.4.7-4
of ventricular size, Artery Conduit be reasonable for adults with repaired TOF fewer systemic
for routine testingeffectand
2. PR resulting from treatment
adults. Whenof it isolated
is appliedPSinmay the have
adult, it is usu-
IIb C-EO for stent function
fracture
and moderate or greater PR with other
toandguide optimal
blood medical,
cultures to
ever, close monitorin
function,c. QRS and duration
RVPR. ≥180function,
sizeHowever, ms interventional and/or surgical therapy.
withthere isRVlack of con- assess for IE. S4.3.6-3,S4.3.6-4
progressive impact on
ally reserved for and
patients severe and dysfunc- Synopsis
Recommendations
lesions requiring surgical interventions.
for Right Ventricle–to-PA Conduit remains necessary.S4.4.2
d. Extensive RV scarring Recommendation
Recommendation-Specific
may resultsensus
in tion regarding
symptoms, with
e.notInducible
such
concern optimal
that
sustained
pulmonary
that indications
the
VT
rightvalve
atentirety
and
ventricle
electrophysiological
timing
will Therapeutic
Fontan
Referenced
9. Pulmonary
repairs
studies that
3. In adults with right
valve
are
to arrhythmia
replacement,
the
support
management,
and most common
recommendations
arrhythmia, may be
ventricle–to-PA conduit
in addition
congestive palliation
are summarizedof sin- sidered; it is a therapy
with aHF, unexplained
replacement of
Supportive Text pulmonary
would tolerate
be valvesupporting
considered. replacement
Serial thefollow-up in of
this stroke
popula- IIb in Online
C-EO Data
IIa gle ventricleC-LD Supplement
considered for
physiology
11.
44.
adults
ventricular
Anticoagulation
with
seenrepaired TOF
inisadults.
dysfunction
vitamin K
Theforphysiology
or cyanosis cardiac Supportive
anecdotal experience Text
studyS4.3.4-6,S4.3.4-15 Preoperative catheterization
volume. and moderate or greater antagonist
PR and ventricular recommended adults with
for clinicaltion.evaluation,
Pulmonary CPET, and imaging to eval-
largestvalve studyreplacement results in re- catheterization is reasonable to assess the needed. S4.4.2-28,S4.4.2-30
A
to The of patients with CORis complex,I LOE withRecommendations
long-term consequences
Fontan palliation with known or related
suspectedto 1. Atrial tachyarrhy
1. Patients
uate for duction
symptoms,with determine
ACHD
exercise
hemodynamics
often
intolerance overestimate and feasibility
attribut- their repaired
of tachyarrhythmia.
C-EO hemodynamics.thrombus, thromboembolic events, or prior
may be
S4.3.6-5,S4.3.6-6
applied in an
TOF of
applyingand RVthe volume
ICDs included
bidirectional and cavopulmonary
relief of PR; however,
121limitations.
patients from 11
shunt the obligatory elevation in central venous pressure and adults with Fon
able to physical
PR, and/orcapabilities
RV onlydilation and or underreport
RV dysfunction will in older
Diagnostic
Therapeutic
reduced cardiac output.toProposed
atrial arrhythmia, and no contraindications
medical therapy for egies with
collectively
substantial appm
these Northare
becomes American surrogates
progressively and more for
European outcomes.
important
sites followed Many Synopsis
for anticoagulation.
allowIn contrast
appropriate to
timing patients
of with
intervention acquired
if needed. heart di- the “failing Fontan,”12.which
4. 1. Coronary
Right artery
ventricle–to-PA may compression
manifest
conduit testing
asinprotein-
intervention with outcome compared
arrhythmias may w
patientsa patients,
with
median particularly
repaired
ofACHD 3.7 years those
TOFwith maylongstanding
after deny
ICD symptoms
haveimplantation.
hy-
ex-lead Long-term survival after surgeryis for Catheter
TOF
simultaneous ablation
continues coronary can be useful
toangiography adults
and
3. Theresease,
are nopatients
data to with
pertension suggest
with LV may
appropriate
hypertrophy, never timing
which can losing enteropathy, reasonable
hepatic for adults
dysfunction,
after Fontan
with
palliation with
right ventricle–
lower extrem-
intra-atrial Fontan
poorly surgery
tolerated, has
yet Overall,
demonstrate 30% ofreduced patients received exercise at tolerance.
least 1 ap-improve. However,
Downloaded from http://ahajournal
IIaresidualC-LD hemodynamic
to-PA conduitand
high-pressure andballoonelectro-
moderate dilation
or greater in the conduit
perienced
for pulmonary to“normal”
valve replacement
diastolic function.
dysfunction in Decline
the
and presence in physical
elevated pulmonary
physiological
IIaI ity venous B-NR
abnormalities
B-NRcongestion,
are PR is
common and/or
reentrant
orindicated
moderate in or exercise
tachycardia or limitation,
greater
adulthood.
before rightstenosis (Table has
focal atrial
ventricle–to-PA
tion of atrial refracto
compromise oft
propriate
Pulmonary ICD
valve discharge,
replacement corresponding
in such to annual
patients tachycardia. S4.4.2-13–S4.4.2-15
of RVcapacity
dilation, maypressures.
but it occur is likelyimperceptibly
inappropriate over to di- many included many different 22) with modalities,
reduced functional although there
capacity or valve is ring, and
Therefore, they c
intra-atrial
has appropriate
been associated shock rates with of 7.7% andfunctional
improved 9.8% forAdults with repaired TOF face an increased
conduit stenting
13. Fontan revision
arrhythmia.
risk or oftranscatheter
ar-
surgery, including nus node dysfunction
S4.3.6-7–S4.3.6-11
l rectlyyears.
extrapolate the Consequently,
S3.4.7-1,S3.4.7-2 data applicable to patients
tools more precise limited proven benefit in published
placement. S4.3.6-1,S4.3.6-2 research. Options including urgent
4.3.5. Tetralogy
primary andof secondary
Fallot prevention indications,rhythmias, exercise intolerance, HF, and deathsurgery
arrhythmia begin- as indicated, is
- TOF.status.
with than S4.3.1.1-1 S4.3.5-9,S4.3.5-10
patient However, RV dilation
historyforS4.3.5-16
are or dysfunc- ning in early for medical
adulthood. therapy
5. Right include aldosterone
ventricle–to-PA
S4.3.5-1,S4.3.5-18–S4.3.5-20
Surgical conduit
re- antagonists
intervention or during erslong-term
who can follo
hel
TOF necessary for evaluation 2. In be reasonable
patients with forstented
adults with rightatriopulmonary
ventricle–to-PA
respectively.
Recommendations Unlike patients with acquiredpair of TOF has subcutaneous
evolved over may
unfractionated
time, reasonable
with relief for
heparin,of asymptomatic
the which may sta- has been associated
s 7. Risk
tion should
and serial factors
improve,
follow-up forat
or SCD
ofleast include:
not
functional progress
capacity. fur-
are CPET conduits Fontan connections
and worsening with recurrent
PS orconduit
PR, evaluation strategies, even i
HF,
Referenced
evidence
studies that
suggests
support
that patients
recommendations
with TOF who adults with
atrialright ventricle–to-PA
and catheterStout 2019
RVOT obstruction IIausually C-LD
involving tachyarrhythmias
infundibulotomy, refractory to the single ventricle, in
ther, provides
if the volume
a. summarized
LV overload
systolic or
in Online Data from
diastolic PR dysfunction
Supplement is 43.
alleviated
(See Section 4.3.6. for IIb bilize the proteoglycan
B-NR
andfor layer
conduit of the
complications gut. PAH should therapies
be thrombotic thera
, objective,
have inducible reproducible,
sustained and
polymorphicrepeatable ofVTright(hazard resection ofIobstructive B-NRmuscle bundles,
severe stenosis
pharmacological
and the
or therapy
severe
use of
regurgitation
by pulmonary
recommendations
valve
regarding
replacement.
evaluation and management
Thus, although and are of increasing interest.
withperformed,
reduced Endothelin
RV including
ejection antagonists
fluoroscopy
fraction or RVto have
evaluate sure, reduced
into accountcardiac the
m b.ventricle–to-PA
assessment Nonsustained
ratio: of 12.9)
the fareVT
cardiovascular,
conduits.)
as poorlyrespiratory,as or worse than thosea patch to enlarge
ablation who have preserved systolic
beenthe pathway
studied in afrom
dilation.
single the
for stent right
RCT, fracture ventricle
which andshowed
blood cultures
improved to protein-losing entero
S4.3.6-12–S4.3.6-14
ventricular function and severe atrial mation and poteEbstein
Maladie d’Ebstein
Indication opératoire
• Tolérance fonctionnelle
• Fonction VD
• Importance de la fuite
• Cyanose
• TDR
• Réparabilité de la valve antérieure
Echo, IRM, Holter, EE + VO2maxVO2
Le débit cardiaque au pic apporte un
complément en plus de la VO2 et pente
VE/VCO2 dans la stratification du risque
est patients insuffisants cardiaques
Myers 2013
Wilson 1995VO2 = déterminant cardiaque ?
• Le débit cardiaque : fort déterminant de la VO2max
Fallot Fontan patients
p = 0,0002 10
r = 0.43
60 8
IC (L/mn/m2)
6
Peak VO2 mL/kg
40
4
20 2
0
0 0 10 20 30 40
0 5 10 15
VO2 (mL/Kg))
CI L/mn/m2“
Peut on relier la diminution de la VO2 max à la
lésion cardiaque ?
Quels sont les déterminants de la VO2max ?
”Facteurs influençant la VO2max
Performance
cardiaque
Fonction
pulmonaire VO2 Hémoglobine
Utilisation
périphérique
de l’O2Test cardiopulmonaire Décision thérapeutique Fonction cardiaque • Détection précoce de l’altération de la fonction ventriculaire • Détection de l’altération ventriculaire dans les conditions de charge anormales (fuite+++) • Detection de l’altération de la fonction diastolique • Detection de de l’altération de ventricule droit ou unique
Limitation cardiaque/vasculaire
Lésion résiduelle • Sténose pulm/Ao
valvulaire… • Augmentaion des
• Diastolique RVP/RVS
• Systolique
Augmentation
Altération
de la post
myocardique
charge
Defaut de Insuffisance
precharge chronotrope
• DCPT • Chirurgie
• Beta bloquantlimitations extracardiaques
Dysfonction pulmonaire
• Chirurgie
• malformatif
Troubles
Psychologiques
• Surprotection, Déconditionne-
• Faible activité
φ ment
• Retard mental
Maladie squelettique
• ScolioseTest cardiopulmonaire
Décision thérapeutique
• Ventilatoires
Épuisement de la réserve ventilatoire (VMV –VE max/VMV)x100
avec VMV = 35 (ou 40) x VEMS
normalement 30 ±15%
• Deconditionnement musculaire peripherique
Seuil ventilatoire abaissé (% th) : non sedentaire > 55 %
• Eliminer l’anémie= Q x (CaO2-CvO2)
= k x DO2 x PvO2
= VI x 0,2093 – VE x FEO2Evaluer les déterminants de la VO2 max VO2 = VES x FC x (CaO2-CvO2) Déterminant cardiaque Déterminant musculaire périphérique On mesure en pratique VO2 et FC….
Déterminants cardiaque ? • La FC • Le pouls d’O2 = VO2/FC = VES x (CaO2 – CvO2) • Pente VE/VCO2 • Pente VO2/watt •…
Pouls d’O2
= VO2/FC = VES x DAV
• Valeur pronostique dans l’insuffisance cardiaque
• Valeur de la cinétique dans les cardiopathies ischémique
• Peu d’effet du RVP sur pouls d’O2 : valver dès que le pouls d’O2 est
anormal ? pb de la DAV (Legendre 2015)
• Population de Fontan : pas de corrélation pouls d’O2/VES (Legendre 2017)Pouls d’O2 = déterminants cardiaque ?
Fallot
Fontan patients
16
14
12
O2 pulse (ml))
10
8
6
4
2
0
0 20 40 60 80 100
SV
Legendre 2017,
Guirgis 2019Pente VE/VCO2
- Acidose métabolique précoce (faible débit cardiaque…)
- Control respiratoire altéré
- Chemorefelexe
- Ergorecepteurs O2 O
Pulmonary Venous Circuit
2
- Augmentation de l’espace mort O2
- Vaso regulation pulmonaire altérée CO2 CO
2
Cardio-
Pulmonary
Interface
Left
Atrium-
Ventriicle
- Altération de la fonction VD
Pulmonary Arterial Circuit
Systemic Arterial Circuit
Chemo/
Ergo
Receptor and`
CO2
O2
ANS Balance
- HTAP (post capillaire…) Right
Atrium-
A Skelettal
- Sténoses sur l’arbre artériel pulmonaire Ventricle
V Musccle
- Cyanose
CO2
Systemic Venous Circuit
- Hyperventilation FIG 1. Conceptual model for cardiovascular, pulmonary, and systemic circuits involved in gas
exchange from the atmosphere to the skeletal muscle. ANS, autonomic nervous system. (Color
version of figure is available online.) Myers 2015
Rehabilitation (EACPR) recommended the assessment of the VE/VCO2
slope in all patients with HF undergoing CPX, irrespective of etiology.23
The recommendation to express the VE/VCO2 relationship as a slope
(throughout exercise) as opposed to a ratio (expressed at a given time
point) stems from the rationale that expression of VE and VCO2 dataPente VE/VCO2 = déterminant cardiaque ?
• Pente VE/VCO2
VE/VCO2 slope - IC
14
12
10
8
6
4
2
0
0 10 20 30 40 50
Fallot adulte Enfant CHD
Guirgis 2019Et si on mesurait de déterminant cardiaque !
VO2 = VO2 =
VES x FC x (CaO2-CvO2) k x DO2 x PvO2
DIFFUSION
Déterminant cardiaque Déterminant musculaires périphériques
PvO2 Distance capillaire
Densité
capillaires/mitochondriesCaO2
VO2 = Q x (Ca02-Cv02)
Q
Ca02 = Hbx1,34xSa02 + dissolved O2
Dissolved 02 very low
Cardiac output Sa02 = 100%
Hb = 14g/dL
So, CaO2 = 200 ml/L
CvO2
(deduced)
SvO2
PvO2
VO2 max is a function of PvO2 (curve)cipe de FICK On connait
V02, Q,
Ca02 CvO2
Q max x CaO2 max
VO2 Et la courbe de dissociation de l’Hb
(Hill Equation)
On peut calculer PvO2 et Q x Ca02 max
VO2 Equation de Fick
max
0 PvO2 au pic 100 PvO2Diffusion tissulaire de l’oxygène des capillaires aux
mitochondries
Distance capillaire
Densité capillaires/mitochondries
K=2
Wagner 1995On connait PvO2
On peut calculer DO, k=2
VO2
Q max x CaO2 max
Diffusion de
l’oxygene
0
xD
VO2 K
max
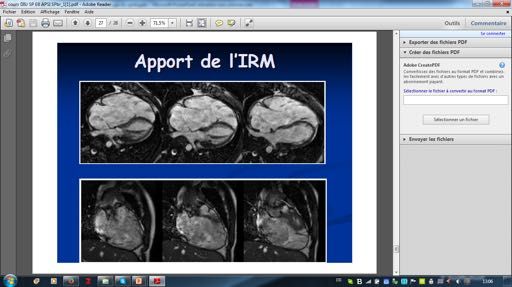
Apport de
l’oxygene
0 PvO2 au pic 100 PvO2
Wagner 1995Baisse de la VO2 max
VO2 Q x CaO2max
Baisse de la
performance
0
xD
cardiaque
VO2 K (baisse du Q max)
max
D D
0 PvO2 au pic 100 PvO2Baisse de VO2 max
VO2
Q x CaO2max Baisse de la diffusion
Déconditionnement
0
xD
VO2 K
max D 0’
K x
0 PvO2 au pic 100 PvO2Baisse de la VO2 max
Qmax x CaO2
VO2
Baisse de la
diffusion de
0
xD
’’ l’oxygene (D0)
K
D 0
Kx
VO2 +
max Baisse du
transport de
l’oxygene (Q )
0 PvO2 at maximal exercise 100 PvO2Déterminants VO2max
Cardiopathies congénitales
Guirgis, 2020Déterminants VO2max
Cardiopathies congénitales
Guirgis, 2020Tétralogie de Fallot réparée
Indication du RVP basée principalement sur les volumes VD Stratégie décevante - Pas d’effet sur fonction VD (méta analyse Cheung 2010) - Ameliore un peu la fonction VG au repos (Tobler 2012, Chalard 2012) - Pas/peu d’effet sur la VO2 max (Gengsakul 2007, Geva 2010, Tang 2010, Legendre 2015)
VES à l’effort : physiologie
• Physiologie normale
Starling inotropisme
Cycle du calcium
Affecté dans l’insuffisance
cardiaque
Higginbotham 1986
Neves 2016VES à l’effort et Fallot
spécifique de la fonction VD ?
Δ VTD VD Δ VTS VD
Δ VES VD Δ FE VD
Roest 2002, Van den Berg 2009, Lurz 2012,VES à l’effort et Fallot
spécifique de la fonction VD ?
Tulevsky 2003Risque de mort Benefice de la
subite à l’effort pratique régulière du
sport
Prescription personnalisée
de l’activité sportiveExercise-related SCD in CHD
Children Adults
11 272 children with CHD, sudden 26000 pts, 1200 deaths
death 0,2 %,
SCD = 19% of the overall deaths
• exercise-related SCD = only 10%
of SCD
• none during exercise
• = 6/10000 pts
Koyac, Circulation 2012
Zomer, Int J cardiol 2013
Jortweit, Eur Heart J 2016Exercise-related SCD (young athletes)
Coronary anomalies
Valvular and supravalvular aortic stenosis
Aortic dissection rupture
Other congenital abnormalities
Thompson, circulation 2007Risk factors of SCD (CHD)
History
Symptoms
(Arrhythmia/HF)
ECG VT
Increase QT Anti-arrhythmic
dispersion,
QRS duration
Exercise test
Defects Exercise induced
Ventricular function arrhythmias
Fallot Moderate to severe
ccTGA ventricular dysfunction
Atrial switch (pulmonary/systemic)
LVOT obstruction Overload
Eisenmenger/HTAP pressure/v
Ebstein olume
Documented
SVT
Koyac, circulation 2012
Khairy, Can J cardiol 2014
Lowe, JACC 2011
Gatzoulis, Lancet 2000En pratique: évaluation des patients
Budts Eur Heart J 2013Venticules
Fonction
hypertrophie
FONTAN
contrainte sytemic RV
Pression
pulmonaire
Aorte
Arythmie
saturation
tout Au moins 1 Au moins 1
Composante 3 2 1
statique
Intensité 3 2 1
Budts Eur Heart J 2013Monitoring de l’intensité de l’effort dynamique Frequence Echelle de cardiaque Borg
Test cardiopulmonaire Mise en place du programme d’entrainement • Importance de l’intensité de l’effort dans la recommandation de l’activité sportive
Cas particulier : switch atrial
TGV Switch atrial
VG
VG
VD
VDCas particulier : switch atrial
Mort subite
• Plus de 80% des morts subites surviennent à l’effort
• Facteur de risque: atrial arrhythmia (trigger de TV)
• Faible augmentation du volume d’ejection à l’effort
• Hypothese de l’ischemie myocardique
Kammeraad, JACC 2004
Wheeler, cong heart dis 2014
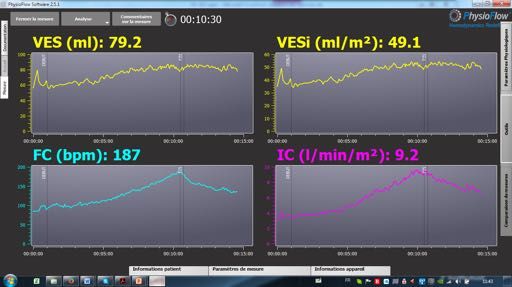
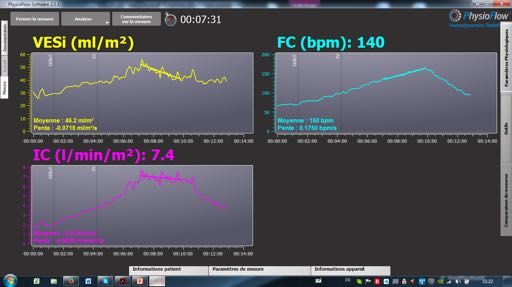
Khairy, curr opin cardiol 2017Switch atrial: monitoring du vol. d’ejection systolique (VES)
Augm. Normale du VES
Faible augm. Du VES
Baisse du VES 137/minVous pouvez aussi lire