INFECTIONS à STAPHYLOCOQUES SRLF 2018 - Nicolas Bréchot
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous
INFECTIONS à STAPHYLOCOQUES
SRLF 2018
Nicolas Bréchot
Pitié-Salpêtrière, Paris
nicolas.brechot@psl.aphp.fr
CAS CLINIQUE 1 Patient de 65 ans, polyvasculaire, à J3 de pontages aorto- coronariens. Présente une fièvre à 38,5 °C sans point d’appel clinique clair ni signe de mauvaise tolérance, pour laquelle des hémocultures, un ECBU et une radio de thorax ont été effectués. A 12 heures, le patient est discrètement marbré, la lactatémie artérielle est à 4,5 mmol/L. Le patient se plaint d’une douleur au point de perfusion veineuse périphérique, et le laboratoire de bactériologie appelle pour dire que les hémocultures poussent à cocci gram+ en amas.

CAS CLINIQUE 1 Le cathéter a été retiré et mis en culture. Quelle antibiothérapie débutez-vous? • A. Cloxacilline (Orbénine) • B. Vancomycine • C. Cloxacilline + Vancomycine • D. Vancomycine + Rifampicine • E. Vancomycine + Gentamicine
CAS CLINIQUE 1
Bactériémie à Staphylocoque à point de départ d’un cathéter
veineux périphérique, compliqué de sepsis.
France CCLIN
RAISIN Paris nord
Année 2015 2014
N 281 45 (/6mois)
SCN 27% 29%
Entérobactéries 26% 24%
S. aureus 17% 24%
P. aeruginosa 10% 9%
Candida spp. 9% 7%
Entérocoques 7 7%
Autres 4
CDDEP – The Center For Disease
Dynamics, Economics & Policy
France: 16% î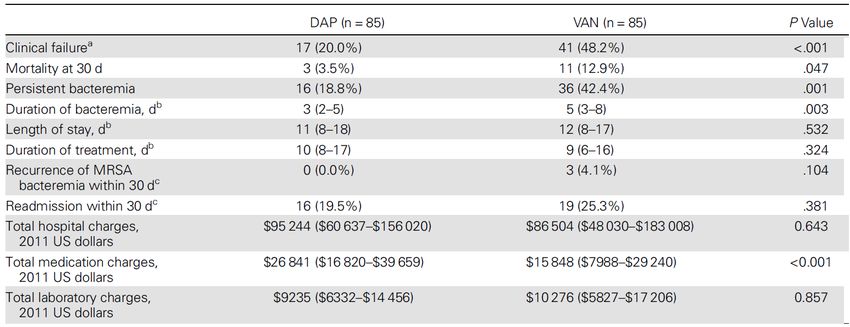
Vancomycine: Bactéricidie lente
Chang. Medicine 2003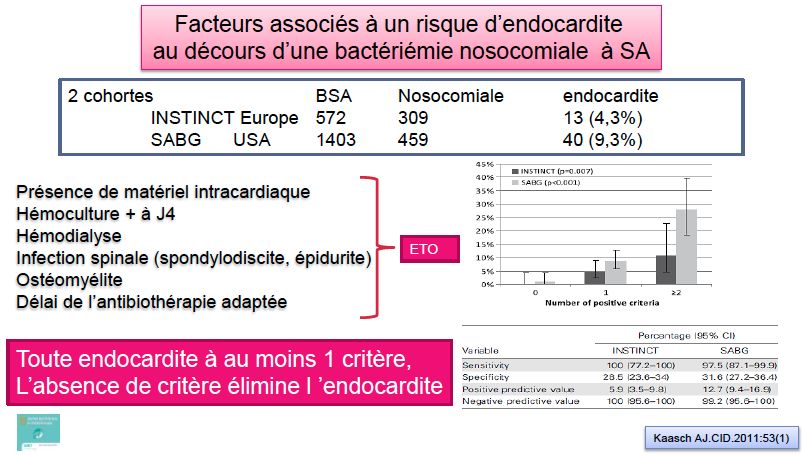
Vancomycine versus β-Lactamine pour
Bactériémies à SDMS
McConeghy KW, et al. Clin Infect Dis 2013;57(12):1760–5
SDMS: Bétalactamines équivalentes?
Paul, Clinical Microbiology and infection 2010
SDMS: Bétalactamines équivalentes?
PRIVILEGIER CLOXACILLINE IV
Tattevin, Clin Microbiol Infect 2005
SDMS: Cefazolin vs Oxacillin?
Etude rétrospective, 2008-2012, 582 patients
Bactériémies compliquées (Hc>4J, localisations IIaires, matériel
prothétique)
Clinical cure idem: 95% vs 88%, p=0.25
Durée bactériémie idem (4 jours)
Rechute idem: 29% vs 19%, p=1.0
Li, Antimicrobial Agents and Chemotherapy 2014SDMS: Cefazolin vs Oxacillin? Li, Antimicrobial Agents and Chemotherapy 2014
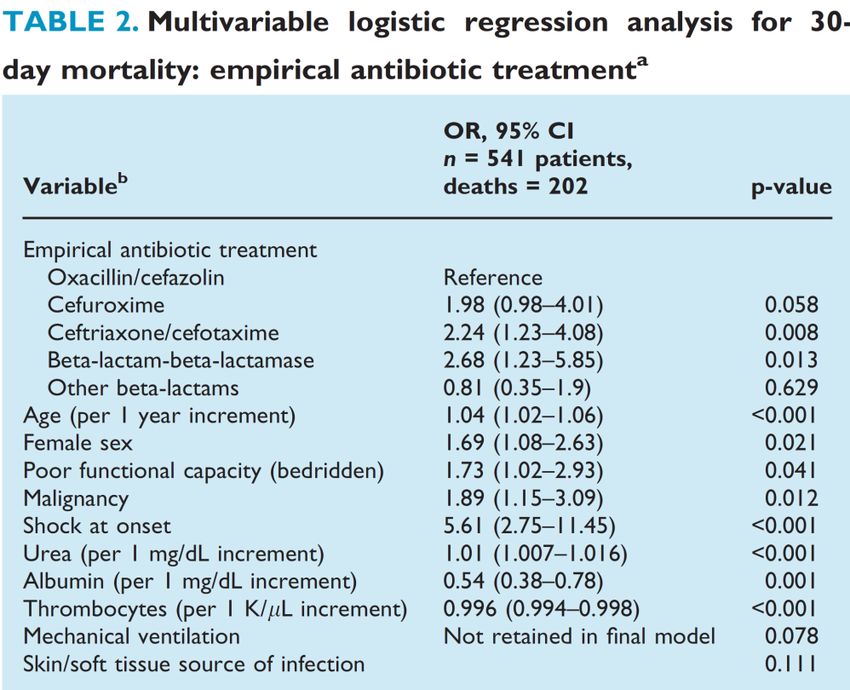
SDMS: Traitement empirique
Etude rétrospective, 2003-2010, 122 hôpitaux, 16973 patients
Bactériémies à SDMS, mortalité à 30J 14%
TRAITEMENT EMPIRIQUE
Beta-lactamine = Vanco: HR 1.03 (0.89-1.2)
Mais 32% pipe-Taz, 29% ceftriaxone
TRAITEMENT DE POURSUITE
Beta-lactamine > Vanco: HR 0.65 (0.52-0.8)
McDanel. CID 2015Bactériémie à Staphylocoque:
Quid des aminosides
ENDOCARDITES à SDMS, valve native
RDZ
Ribera. Annals of Internal Med 96Bactériémie à Staphylocoque:
Quid des aminosides
ENDOCARDITES à SDMS, valve native
Essai Randomisé, 78 patients
Nafcillin 6S vs Nafcillin 6S + gentamycine 2S
↓ bactériémie d’1 jour
Korzeniowsk. Annals of Internal Medicine 1982Bactériémie à Staphylocoque:
Quid des aminosides
373 pts
Endocardite Infectieuse
Buchholtz. CID 09Bactériémie à Staphylocoque:
Quid des aminosides
Sous-étude d’une large étude RDZ
Dapto vs tt standard ds bactériémies à Staph
236 pts
Aminosides -> OR 3.39 (1.43-8.0) pour
dégradation significative de la fonction rénale
Cosgrove. CID 09CAS CLINIQUE 1
Quelle antibiothérapie débutez-vous?
• A. Cloxacilline (Orbénine)
• B. Vancomycine
• C. Cloxacilline + Vancomycine
• D. Vancomycine + Rifampicine
• E. Vancomycine + Gentamicine
CLOXACILLINE 2g x4/J
VANCOMYCINE
15 à 20 mg/kg x2/J (résiduelle 15-20 si discontinue)
IVSE 40 mg/kg/j => concentration équilibre 25-30
Dose de charge 15-25 mg/kgCAS CLINIQUE 1 Quelques heures plus tard, vous apprenez l’identification d’un staphylocoque doré. La recherche de PLP2a est négative. Comment poursuivez-vous le traitement? • A. Cloxacilline (Orbénine) 14j • B. Cloxacilline + Rifampicine 14j • C. Cloxacilline 10 à 14j • D. Cloxacilline 14j + Gentamicine 5j • E. Cloxacilline durée guidée par la procalcitonine
Bactériémie à Staphylocoque:
Quid de la Rifampicin
• Pas à la phase initiale
20% d’émergence de souches RMP-R si début en phase bactériémique
Forrest at al. Clin Rev Microbiol 2010
• En association à 1 anti-staph majeur dans les bactériémies non
compliquées?Bactériémie à Staphylocoque:
Quid de la Rifampicin
758 pts. Bactériémie à Staph
RDZ
370 Double aveugle 388
ATB 29 centres (UK) ATB
+ +
Rifampicine 14J Placebo
(600 à 900 mg/J) ECHEC du TT/ RECIDIVE
ou
MORTALITE
Hypo: î de 35 à 25%
12 semaines Thwaites. Lancet 2018RMP Placebo
n=370 n=388
Communautaire 62% 66%
SDMR 5% 7%
Tissus mous/abcès 24% 22%
Cathéter 17% 17%
Valve native 4% 5%
Pace-maker/DAI 6% 4%
Prothèse valvulaire/
1% 2%
orthopédique RMP vs. Placebo
SOFA 2 (1-4) 2 (1-4) Echecs: 1% vs. 1%, p=0.82
Flucloxacilline 83% 81% Récidives: 1% vs. 4%, p=0.01
Durée tt 30 (18-44) 29 (17-45) Mortalité: 15% vs. 14%, p=0.6
Thwaites. Lancet 2018TOLERANCE
RMP Placebo
p
n=370 n=388
EI->Modification tt 17% 10% 0.004
IRA 5% 1% 0.01
Tbles digestifs 24% 8% 0.003
Interactions 6% 2% 0.005
Staph RMP-R 1% nd
Thwaites. Lancet 2018Bactériémie à Staphylocoque:
Quid de la Rifampicin
• Pas à la phase initiale
20% d’émergence de souches RMP-R si début en phase bactériémique
Forrest at al. Clin Rev Microbiol 2010
• En association à 1 anti-staph majeur dans les bactériémies non
compliquées? NON
• En association à 1 anti-staph majeur dans les bactériémies
compliquées?Rifampicine & matériel étranger
Expérimental chez le rat. Infection de prothèse fémorale
TT 14 J
Fémur Biofilm
Greimel. Drug design, dev & ther 2011Rifampicine & matériel étranger
RMP 60%
Mortalité à 30J: 31%
Population totale: RMP non associée à la mortalité à J30
HR 0.95 [0.68-1.34]
Matériel étranger:
HR 0.53 [0.33-0.91]
Rieg. Clin Microbiol Infect 2017Rifampicine & matériel étranger
Infections Prothèses orthopédiques à staph, tt conservateur
Flucloxa/vanco 2S puis Ciprofloxacine 3 à 6 mois
RDZ, ouvert
Exclusions 6/18 vs 3/15
Endpoint clinique
Zimmerli. JAMA 98Bactériémie à Staphylocoque:
Quid de la Rifampicin
• Pas à la phase initiale
20% d’émergence de souches RMP-R si début en phase bactériémique
Forrest at al. Clin Rev Microbiol 2010
• En association à 1 anti-staph majeur dans les bactériémies non
compliquées? NON
• En association à 1 anti-staph majeur dans les bactériémies
compliquées? RECOMMANDE dans les infections graves sur
matériel étranger laissé en place (endocardite sur prothèse,
matériel orthopédique)Bactériémie à Staphylocoque:
Durée du traitement
Etude prospective, 2008-2010
111 bactériémies à staph (47% SDMR) non compliquées (Hc negBactériémie à Staphylocoque:
Durée du traitement
Chong. Antimicrobial Agents and Chemotherapy 2013CAS CLINIQUE 1
Quelques heures plus tard, vous apprenez l’identification d’un
staphylocoque doré. La recherche de PLP2a est négative. Comment
poursuivez-vous le traitement?
• A. Cloxacilline (Orbénine) 14j
• B. Cloxacilline + Rifampicine 14j
• C. Cloxacilline 10 à 14j
• D. Cloxacilline 14j + Gentamicine 5j
• E. Cloxacilline durée guidée par la procalcitonine
CLOXACILLINE 2g x4/J
CEFAZOLINE 2g x3/JCAS CLINIQUE 1 Trois hémocultures (/3) reviennent positives sur les 72 premières heures. Les suivantes sont négatives. Le cathéter a été retiré et pousse à SDMS (104 UFC/ml). Que pensez-vous des propositions suivantes? • A. Une échographie cardiaque trans-thoracique est indiquée • B. Une échographie cardiaque trans-oesophagienne est indiquée • C. Une endocardite associée est détectée dans 1 à 2% des cas • D. Une endocardite associée est détectée dans 5 à 25% des cas • E. Une endocardite associée est détectée dans 25 à 33% des cas
SAVOIR REPETER L’ETT à J7
CAS CLINIQUE 1 Trois hémocultures (/3) reviennent positives sur les 72 premières heures. Les suivantes sont négatives. Le cathéter a été retiré et pousse à SDMS (104 UFC/ml). Que pensez-vous des propositions suivantes? • A. Une échographie cardiaque trans-thoracique est indiquée • B. Une échographie cardiaque trans-oesophagienne est indiquée • C. Une endocardite associée est détectée dans 1 à 2% des cas • D. Une endocardite associée est détectée dans 5 à 25% des cas • E. Une endocardite associée est détectée dans 25 à 33% des cas
CAS CLINIQUE 1 Si la recherche de PLP2a avait été positive. Comment auriez-vous poursuivi le traitement? • A. Vancomycine 15-20 mg/kg x2/J • B. Vancomycine IVSE • C. Daptomycine 6 mg/kg/J • D. Daptomycine 8 mg/kg/J • E. Linezolide 600 mg x2/J
Antimicrobial Agents for the
Treatment of MRSA Infections
§ Vancomycin/teicoplanin
§ Trimethoprim-SMS /rifampicin/fosfomycin
§ Tigecycline
§ Daptomycin (excluding pneumonia)
§ Linezolid/tedizolid
§ Ceftaroline/ceftobiprole
§ Telavancin
§ Dalbavancin/oritavancinAntimicrobial Agents for the
Treatment of MRSA Infections
§ Vancomycin/teicoplanin
§ Trimethoprim-SMS /rifampicin/fosfomycin
§ Tigecycline
§ Daptomycin (excluding pneumonia)
§ Linezolid/tedizolid
§ Ceftaroline/ceftobiprole
§ Telavancin
§ Dalbavancin/oritavancinChanges in Vancomycin MIC Have Been
Observed in Many Clinical Settings
Phenotype
Year Isolates
S. aureus MRSA MSSA
All (n) 20,004 8249 11,755
2004–2009 Vancomycin MIC ≥2 µg/mL, n (%) 797 (4.0) 439 (5.3) 358 (3.0)
All (n) 2525 1158 1367
2004 Vancomycin MIC ≥2 µg/mL, n (%) 101 (4.0) 65 (5.6) 36 (2.6)
All (n) 2930 1411 1519
2005 Vancomycin MIC ≥2 µg/mL, n (%) 62 (2.1) 39 (2.8) 23 (1.5)
All (n) 3612 1531 2081
2006 Vancomycin MIC ≥2 µg/mL, n (%) 94 (2.6) 50 (3.3) 44 (2.1)
All (n) 4944 2028 2916
2007 Vancomycin MIC ≥2 µg/mL, n (%) 160 (3.2) 78 (3.8) 82 (2.8)
All (n) 4348 1481 2867
2008 Vancomycin MIC ≥2 µg/mL, n (%) 253 (5.8) 136 (9.2) 117 (4.1)
All (n) 1645 640 1005
2009 Vancomycin MIC ≥2 µg/mL, n (%) 127 (7.7) 71 (11.1) 56 (5.6)
Hawser SP, et al. Int J Antimicrob Agents 2011;37:219–24
22Using PK-PD Data to Optimize Vancomycin
Therapy
Target: AUIC/MIC >300
Peak
Antibiotic (C)
Antibiotic (C)
24h AUC 24h AUC
MIC=0.5 µg/mL MIC ≥1.5 µg/mL
Time (h) Time (h)
Adapted from: Drusano GL, Clin Infect Dis. 2007;45:753–760
41
McKinnon PS & Davis SL. Eur J Clin Microbiol Infect Dis.
2004;23:271–288Vancomycin-Associated Nephrotoxicity in 1,430
Critically Ill Patients:
A Retrospective Multivariate Regression Analysis
Precision Of Predicting Nephrotoxicity And Incremental Risk Increase Of Different Threshold
Values For Highest Measured Vancomycin Serum Concentrations
Relative Positive Negative
Threshold Nephrotoxicity Risk Sensitivit Specificit Youden
Predictiv Predictive
Level (mg/L) (%) Increase y y Index
a e Value Value
10 21.7% 1 0.043 0.043 0.217 1
15 23.2% 1.069 0.936 0.178 0.115 0.232 0.914
20 26.2% 1.207 0.84 0.372 0.212 0.262 0.898
25 33.1% 1.525 0.747 0.600 0.346 0.331 0.899
30 41.5% 1.912 0.603 0.774 0.377 0.415 0.880
> 30 47.9% 2.207 0.303 0.912 0.216 0.478 0.831
aRelative to first threshold level (10 mg/L).
Hanrahan TP, et al. Crit Care Med 2014;42(12):2527–36.Vancomycin-Associated Nephrotoxicity in 1,430
Critically Ill Patients:
A Retrospective Multivariate Regression Analysis
Hanrahan TP, et al. Crit Care Med 2014;42(12):2527–36.
§ The prevalence of new onset nephrotoxicity was reported using
RIFLE criteria.
§ Concomitant vasoactive therapy (OR=1.63; pClinical Practice Guidelines by the
Infectious Diseases Society of America for
the Treatment of MRSA Infections
Liu C, et al. CID 2011;52(3):e18-e55
¢ IV vancomycin 15–20 mg/kg/dose every 8–12 h, not to
exceed 2 g per dose, is recommended in patients with
normal renal function (B-III)
¢ In seriously ill patients, a loading dose of 25–30 mg/kg
may be considered
¢ For serious infections, vancomycin trough conc. of 15–
20 ug/mL (25-30 si Continuous) are recommended (B-II)
CMI ≥1,5 g/L -> Trouver autre choseAntimicrobial Agents for the
Treatment of MRSA Infections
§ Vancomycin/teicoplanin
§ Trimethoprim-SMS /rifampicin/fosfomycin
§ Tigecycline
§ Daptomycin (excluding pneumonia)
§ Linezolid/tedizolid
§ Ceftaroline/ceftobiprole
§ Telavancin
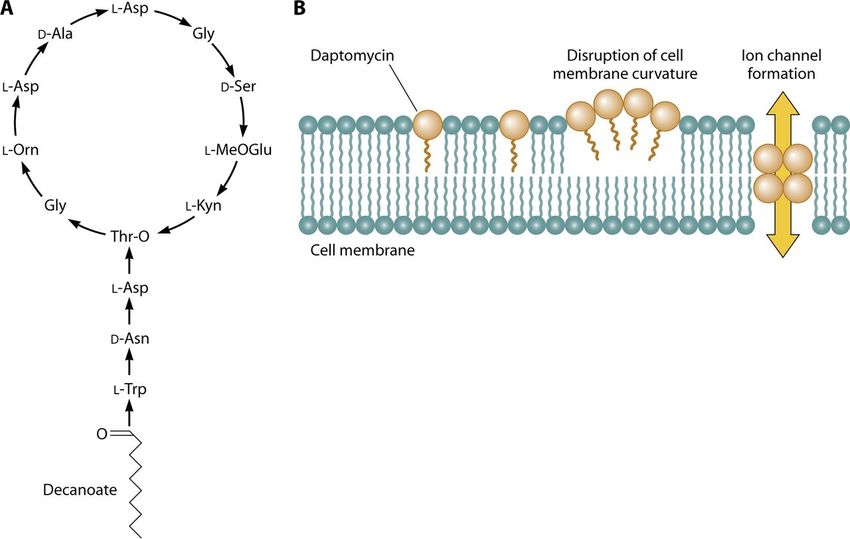
§ Dalbavancin/oritavancinDaptomycin (Cubicin®): Structure
and interaction with the cytoplasmic membrane
Humphries RM, et al. Clin Microbiol Rev. 2013;26:759-80
Daptomycin activity is
inhibited by pulmonary
surfactant245 patients, bactériémies à Staph
SDMR 37%
Bactériémies compliquées 52%
Matériel étranger 25%
Endocardite 15%
RDZ
DAPTO TT standard
6mg/kg
Fowler. NEJM 06• Insuffisance rénale 6,7% vs 18,1%, p=0,009
MAIS
• ì CPK 25% (3% arrêt)
• ì CMI
• 19 échecs microbiologiques (15,8% vs 9,6%, p=0,17)
• 5/45 CMI dapto 0,25-0,5->2-4 ng/ml
Fowler. NEJM 06DAPTOMYCINE
Moore. CID 2012DAPTOMYCINE vs VANCOMYCINE
Rétrospective matchée
Bactériémies à Staph MR
CMI vanco >1 µg/ml
Murray. CID 2013Dapto vs les autres… Méta analyse de 13 essais randomisés
He W, et al. J Antimicrob Chemother. 2014;69:3181-9
51Comparative Effectiveness of Vancomycin
vs. Daptomycin for MRSA BSI With Vanc. MIC
>1 mg/L: A Multicenter Evaluation
Moise PA, et al. Clin Ther. 2016;38:16-30
¢ Nationwide, retrospective, multicenter (N = 11), matched,
cohort study compared outcomes of early daptomycin with
vancomycin for MRSA BSI with vanc. MICs 1.5 to 2 µg/
mL.
¢ Matching variables based on propensity regression analysis
included age, ICU, and type of BSI.
¢ Outcomes were as follows: (1) composite failure (60-day
all-cause mortality, 7-day clinical or microbiologic failure,
30-day BSI relapse, or EOT failure ;(2) nephrotoxicity; and
(3) day 4 BSI clearance.
52Comparative Effectiveness of Vancomycin
vs. Daptomycin for MRSA BSI With Vanc. MIC
>1 mg/L: A Multicenter Evaluation
Moise PA, et al. Clin Ther. 2016;38:16-30
¢ Overall composite failure was 35% (59 of 170): 15% due to 60-day
all-cause mortality, 14% for lack of clinical or microbiologic response
by 7 days, and 17% due to failure at EOT.
¢ Predictors of composite failure according to multivariate analysis
were age >60 years (OR, 3.7; PDAPTOMYCINE CONCLUSIONS
• PAS EN PROBABILISTE
• PAS DANS LES PNEUMONIES (inhibition par surfactant)
• 8 mg/kg/J
• Bonne alternative à la VANCO si SDMR et
Insuffisance rénale
CMI ≥ 1,5 ng/ml
• Attention rhabdomyolyse (arrêt statines)Antimicrobial Agents for the
Treatment of MRSA Infections
§ Vancomycin/teicoplanin
§ Trimethoprim-SMS /rifampicin/fosfomycin
§ Tigecycline
§ Daptomycin (excluding pneumonia)
§ Linezolid/tedizolid
§ Ceftaroline/ceftobiprole
§ Telavancin
§ Dalbavancin/oritavancinLinezolid: Mechanism of Action
Oxazolidinones exert antibacterial activity by binding to the 50S subunit of
the bacterial ribosome, resulting in inhibition of protein synthesis
Oxazolidinone binding site
50S subunit
Peptidyl Amino acid
Transferase
center
Decoding
region A P E
mRN
A 30S subunit
Figure adapted from Locke et al. (2010)Linezolid/tedizolid penetrate well and
rapidly into the lung
Tedizolid in ELF
Tedizolid in AM
Tedizolid in free plasma
Boselli et al. Crit Care Med 2005;33:1529-33
Housman ST, et al. Antimicrob Agents Chemother.
2012;56:2627-34
57
Tedizolid is not approved by ANVISA in Brazil.Tedizolid Exposure in ELF and Alveolar Macrophage Cells
(AM) are Above MIC90 for Entire Dosing Period
Tedizolid ELF & AM Concentrations (200 mg QD Day 3)
10
ELF: epithelial lining fluid Penetration
9 AM: alveolar macrophage
Ratio
8
EL A
Concentration (µg/mL)
7 F M
6 Tedizoli 41. 20.
d1 2 0
5
Linezoli
5.2 0.2
4 d2
3
2
1
0
0 2 4 6 8 10 12 14 16 18 20 22 24
Time (hours)
TZD ELF TZD AM MRSA MIC90 SP MIC90
Compared with linezolid, ELF penetration is 8x and AM penetration is 100x MRSA: methicillin-resistant S. aureus
higher for tedizolid than linezolid SP: Streptococcus pneumoniae
Housman ST, et al. AAC 2012;56(5):2627–2634.
Tedizolid is not approved by ANVISA in Brazil. Conte JE, et al. AAC 2002;46(5):1475–1480.
58Pneumonie à SDMR:
Linezolide vs Vancomycine
1184 pts. Pneumonie nosocomiale à Staph. 348 PP pts
RDZ
172 Double aveugle 176
Linezolid 7-14J Multicentrique Vancomycine
(600 mg x2/J) 7-14J
(15 mg/kg x2/J)
Succès clinique per-protocole
Wunderink. CID 2012Pneumonie à SDMR:
Linezolide vs Vancomycine
Wunderink. CID 2012Pneumonie à SDMR:
Linezolide vs Vancomycine
Wunderink. CID 2012Meta-analysis of MRSA hospital-acquired pneumonia treatment
EU.AI.2014.02 Date of preparation September 2014
*Includes some methicillin-sensitive cases
Wunderink RG, et al. BMJ 2014;348:g1469.Vancomycin nephrotoxicity is higher
than that of linezolid
nephrotoxicity (%)
(n=224) (n=224)
Patients with
*0.5 mg/mL increase in serum creatinine if normal at baseline, or 50% increase if abnormal at baseline
GFR, glomerular filtration rate
Adapted from: Wunderink R, et al. Clin Infect Dis 2012;54:621–629Bactériémies à SDMR:
Linezolide vs Vancomycine
739 pts. Suspicion de bactériémie sur cathéter. 382 ME
RDZ
193 Ouvert 189
Linezolid 7-28J Multicentrique Vancomycine
(600 mg x2/J) 7-28J
(1gx2/J)
Succès microbiologique mITT
Wilcox. CID 2009Bactériémies à SDMR:
Linezolide vs Vancomycine
Cathéters centraux 89%
Staph Doré 22%
SDMR 10%
SCN 16%
Gram neg 15%
Succès microbiologique 88% vs 88%; IC 95% (-6,4; 6,4)
Mortalité globale 21,5% vs 16%; HR 1,38 (IC95% 0,99-1,94)
Wilcox. CID 2009Bactériémies à SDMR:
Linezolide vs Vancomycine
Wilcox. CID 2009Bactériémies à SDMR:
Linezolide vs Vancomycine
Meta-analyse infections à Gram+, succès clinique
Beibei. Int J Antimicrob Agents 2010Antimicrobial Agents for the
Treatment of MRSA Infections
§ Vancomycin/teicoplanin
§ Trimethoprim-SMS /rifampicin/fosfomycin
§ Tigecycline
§ Daptomycin (excluding pneumonia)
§ Linezolid/tedizolid
§ Ceftaroline/ceftobiprole
§ Telavancin
§ Dalbavancin/oritavancinCAS CLINIQUE 1 Si la recherche de PLP2a avait été positive. Comment auriez-vous poursuivi le traitement? • A. Vancomycine 15-20 mg/kg x2/J • B. Vancomycine IVSE • C. Daptomycine 6 mg/kg/J • D. Daptomycine 8 mg/kg/J • E. Linezolide 600 mg x2/J
Bactériémies à STAPHYLOCOQUES
CONCLUSIONS
• SDMS: Cloxacilline/ Cefazoline
• Pas d’indication à l’adjonction d’aminoside/rifampicine
• Durée 14-28 jours
• SDMR Daptomycine en alternative à la vanco si CMI≥1,5
ng/ml
• Prudence avec le Linézolide dans les bactériémies
• Traquer l’endocarditeVous pouvez aussi lire