Epuration extra-rénale et Insuffisance cardiaque - Pr Alexandre OUATTARA Department of Anaesthesia and Critical care Medico-Surgical Center ...
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous

Epuration extra-rénale et
Insuffisance cardiaque
Pr Alexandre OUATTARA
Department of Anaesthesia and Critical care
Medico-Surgical Center Magellan
Hospital Haut-Lévêque
33600 Pessac, France
Ronco C et la. J Am Coll Cardiol 2008;52:1527-39 Type 1: Abrupt worsening of cardiac function leading to acute kidney injury Type 2: Chronic abnormalities in cardiac function causing progressive chronic kidney disease Type 3: Abrupt worsening of renal function causing acute cardiac dysfunction Type 4: Chronic kidney disease contributing to decreased cardiac function, cardiac hypertrophy, and/or increased risk of adverse cardiovascular events Type 5: Systemic condition (e.g., sepsis) causing both cardiac and renal

Type 1
Scoring AKI

HÉMODYNAMIQUE ET INSUFFISANCE CARDIAQUE Cardiaques (congestion) Diminution FEVG Augmentation PTDVG Augmentation Volume sanguin intra-thoracique et Eau extra-vasculaire pulmonaire Rénales (hypoperfusion) Altération débit sanguin rénal Hypoperfusion et hypoxie médullaire externe (dysfonction endothéliale) Congestion+++

PATHOPHYSIOLOGY OF CHRONIC HEART FAILURE
Kalra PR et al. J Am Coll Cardiol 2002;39:1901
SYSTÈME NERVEUX AUTONOME
Augmentation concentration catécholamines
Toxicité cellulaire directe ( Ca++ intracellulaire)
Réabsorption directe Na et eau
1
Nor < 400 pg/ml
Nor 400-800 pg/ml
0.8 Nor > 800 pg/ml
Probabilité de survie
0.6
0.4
0.2
mois
10 20 30 40 50 60
SYSTÈME RÉNINE-ANGIOTENSINE-ALDOSTÉRONE Augmentation de l’activité de l’Angiotensine II Activation SNA (relargage pré-synaptique de NAD) Augmente hypertrophie et remodelage ventriculaire Rétention hydro-sodée Augmentation de l’activité de l’Aldostérone Augmentation réabsorption hydro-sodée
SYSTÈME VASOPRESSINERGIQUE Elévation inappropriée d’AVP « Up-regulation » récepteurs V2 Accentuation effet-antidiurétique
SYSTÈME ENDOTHÉLINE Production par cellules mésangiales rénales, cellules épithéliales glomérulaires et cellules du tube collecteur (médullaire interne) Hyperactivité Vasoconstricteur puissant Rétention hydro-sodée
RÉSISTANCE AUX DIURÉTIQUES
Elison DH Cardiology 2001;96:132–43...FLUID OVERLOAD
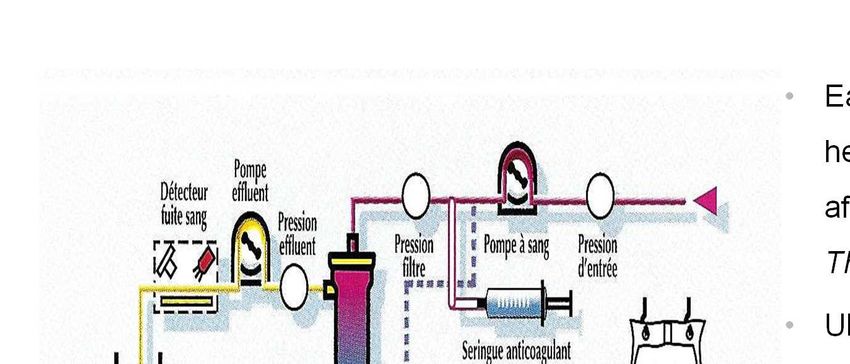
DIURÈSE « MÉCANIQUE » ULTRAFILTRATION
Slow continuous ultrafiltration (SCUF)
• Early and intensive continuous
hemofiltration for severe renal failure
after cardiac surgery (Bent et al. Ann
Thorac Surg 2001; 71: 832-7)
• Ultrafiltration Versus Usual Care for
Hospitalized Patients With Heart
Failure (RAPID-CHF Trial) (J Am Coll
Cardiol 2005 ;46: 2043-6)
• Early ultrafiltration in patients with
decompensated heart failure and
diuretic resistance (J Am Coll Cardiol
2005; 46: 2047-51)DIURÈSE MÉCANIQUE Systèmes simplifiés VV périphériques (DS=10 à 40 ml/min UF 10 à 500 ml/h
Costanzo MR et al. JACC 2007; 49:675-83
Cardiorenal Rescue Study in Acute Decompensated Heart Failure (CARRESS-HF) Fluid removal rate of 200cc/hour If blood pressure stable continue UF 200cc/hour If blood pressure drops or if volume depletion decrease UF to 100cc/hour or discontinue
SYSTEMIC CARDIOVASCULAR AND INFLAMMATORY
DISEASE
Intestinal hypoperfusion
Coronary Bacterial translocation
endothelial
dysfonction
Myocardial
depression
AVP, Ag II
(afterload increase, overload water)
Reynolds HR et al. Circulation 2008; 117:686-97CONSÉQUENCES HÉMODYNAMIQUES DE LA CVVHF MARENZI JACC 2001
CHOC CARDIOGÉNIQUE ET INFLAMMATION
Arch Intern Med 2005; 165: 1643-1650
Analyse à postériori des patients de l’étude SHOCK
(SHould we emergently revascularize Occluded
Coronaries for cardiogenic shocK)
Impact pronostic du SIRS / sepsis?
20% des patients ayant présenté un choc
cardiogénique ont manifesté un SIRS
Mortalité X 2CHOC CARDIOGÉNIQUE ET INFLAMMATION
HOCHMAN CIRCULATION 2003
Mortalité
43 % si Patients DC bas (PTDVG élevées), RVS élevées
et PAM conservée
66 % si Patient DC bas (PTDVG élevées), RVS basses et
PAM basse
Pronostic plus sombre
si composante vasoplégiquePHYSIOPATHOLOGIE DU CHOC CARDIOGÉNIQUE
RÔLE DES INTERLEUKINES
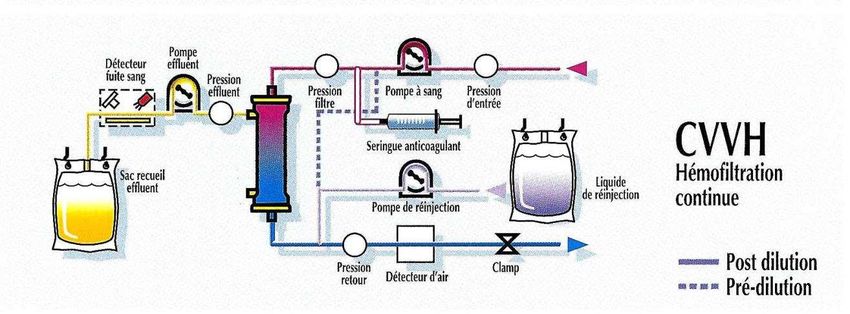
Deswal et al. Circulation 2001CVVHF : HÉMOFILTRATION CONTINUE Systèmes plus performants Voie veineuse centrale de gros calibre UF 10 à 500 ml/h DS 100-250 ml/min Meilleure tolérance hémodynamique
HEMOFILTRATION
Prédilution
Postdilution
Hémofiltration « Haut volume »
= PRE + POST-dilution > 35 ml.kg-1HÉMOFILTRATION (CONVECTION)
UF COMPENSÉE / SUBSTITUTION
Si vol substitué = Vol UF = pas de perte de poids
Si vol substitué < vol UF = perte de poids
UFFRACTION DE FILTRATION
Perte patient + pré-dilution +post-dilution
Débit sanguin + pré-dilution
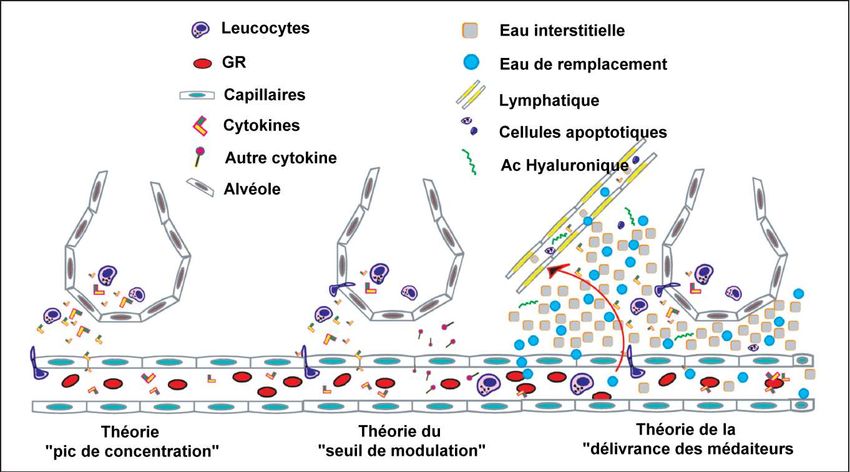
< 25%JUSTIFICATIONS DE L’EER DANS LE CHOC CARDIOGÉNIQUE : RÔLE « ANTI-INFLAMMATOIRE »
HÉMOFILTRATION : « TAXI » DES CYTOKINES
Théorie du « transport des
médiateurs »
J. Di Carlo. IJAO 2005Adsorption
Faible Forte
PolyEther Sulfone AcriloNitrile (AN69)
(PES)IMPACT PRONOSTIC: HFVVC DANS CHOC CARDIOGÉNIQUE Résultats controversés Elahi et al.Early hemofiltration improves survival in post-cardiotomy patients with acute renal failure. Eur J Cardiothorac Surg 2004; 26: 1027-31 Bellomo R, Raman J, Ronco C. Intensive care unit management of the critically ill patient with fluid overload after open heart surgery. Cardiology 2001; 96: 169-76
Am J Resp Crit Care Med 2015;192:1179-90
ESSAI PROSPECTIF RANDOMISÉ
MULTICENTRIQUE
(8 CENTRES FRANÇAIS)PROTOCOLE EXPÉRIMENTAL
CRITÈRES D’ÉVALUATION
Critère principal : Mortalité à J30
Critères secondaires :
Mortalité en réa, à l’hôpital, à J60 et J90,
Nombre de jours sans soutien hémodynamique, sans
EER, sans VM entre l’inclusion et J30
Durée d’EER, de VM, de séjour en réanimation,
d’hospitalisation
Evolution à J3, J7, J15 et J30 du score SOFAPROTOCOL: EXPERIMENTAL ARM HVHF for 48 hours 80 ml/kg/h (or maximum of 8L/h) 50% predilution, 50% postdilution HVHF stopped after 48 h if : Diuresis > 1500 ml/j and Adrenaline
PROTOCOL: CONTROL ARM CVVHDF 350 micromol/L OR x 3/ pre-op Or diuresis 24 h despite volemia optimization Or urea >36 mmol/L Or severe hyperkalemia
HVHF Control
Characteristic
(n=112) (n=112)
At randomization
Time since ICU admission, h 12·9 (11·7) 12·7 (11·8)
Patients on ECMO 47 (42%) 52 (46%)
Patients on IABP 19 (17%) 15 (13%)
Patients on IABP or ECMO 58 (52%) 60 (54%)
SAPS II 54·0 (12·3) 55·1 (12·3)
SOFA score 11·5 (2·8) 12·0 (2·9)
Glasgow coma score 13·5 (3·0) 13·2 (3·4)
Systolic blood pressure, mm Hg 113 (24) 109 (25)
Diastolic blood pressure, mm Hg 63 (14) 62 (14)
Mean blood pressure, mm Hg 79 (14) 77 (14)
Heart rate, beats/min 94 (18) 94 (16)
Epinephrine dose, µg/kg/min 0·23 (0·39) 0·27 (0·46)
Norepinephrine dose, µg/kg/min 0·23 (0·45) 0·32 (0·70)% of patients undergoing RRT
PROBABILITY OF SURVIVAL
% PATIENTS OFF-CATECHOLAMINES
CONTROL
Percent patients off-catecholam ines 60
HVHF
50
40
30
20
10
0
D1 D2 D3 D4 D5 D6 D7 D8
Days after randomizationEVOLUTION OF SERUM LACTATE
12
10
8
6
4
2
0
Day 0 Day 1 Day 2 Day 3Antibiotiques
ARTERY
Imipenem (µg/ml) Before filter
Patient 0101
25,00 After filter
EFFLUENT
20,00
15,00
10,00
5,00
0,00
0 5 10 15 20 25 30 35 40
Time2003
In-hospital mortality rate (%)
70
60
50
40
30
20
10
0
Change < 30 % 30-50 % Change > 50%, Dialysis
no dialysis
Provenchère, Anesth Analg 2003MAJOR RISK FACTORS FOR DEVELOPING AKI-CPB A B Kumar. Cardiopulmonary Bypass-associated Acute Kidney Injury. Anesthesiology 2011;114:964-70
Valve bidirectionnelle
CONCLUSION Rôle additif des phénomènes de convection (rétention hydro-sodée) et de « modulation » de l’inflammation (adsorption) Insuffisance cardiaque « inflammatoire » qui conditionne le pronostic (???) Débit d’ultrafiltration 30-35 ml.kg-1 Impact fonctionnel: « Probablement que OUI! » Impact pronostic: « Non DEMONTRE »
Bossard G et al.
Vous pouvez aussi lire