LE STRUCTUREL EN 2020 ET APRES - GRADIENTS ÉLEVÉS POST-TAVI Hélène Eltchaninoff CHU Rouen - High Tech Cardio
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous
LE STRUCTUREL EN 2020 ET
APRES
GRADIENTS ÉLEVÉS
POST-TAVI
Hélène Eltchaninoff
CHU Rouen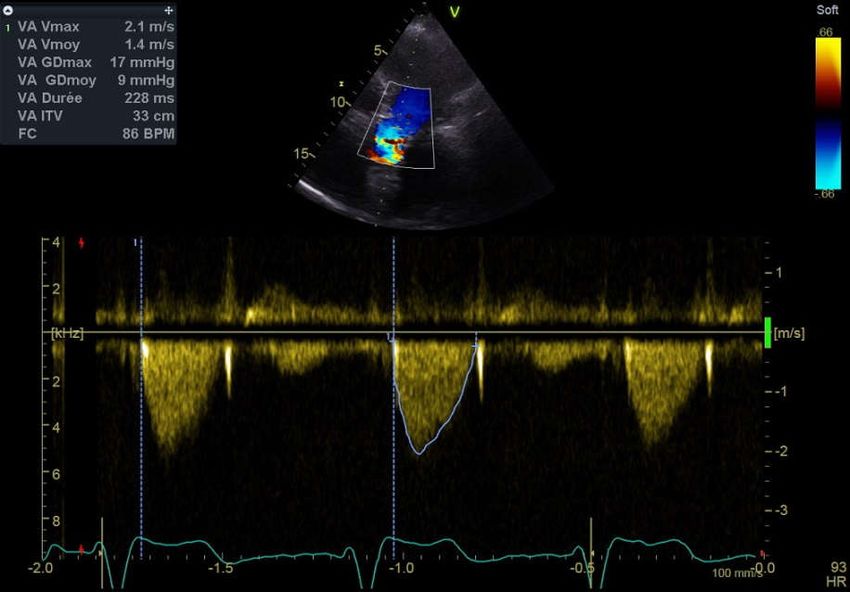
CE QUI EST NORMAL APRÈS TAVI
Pas de gradient hémodynamique
Gradient moyen < 10 mm g en ETT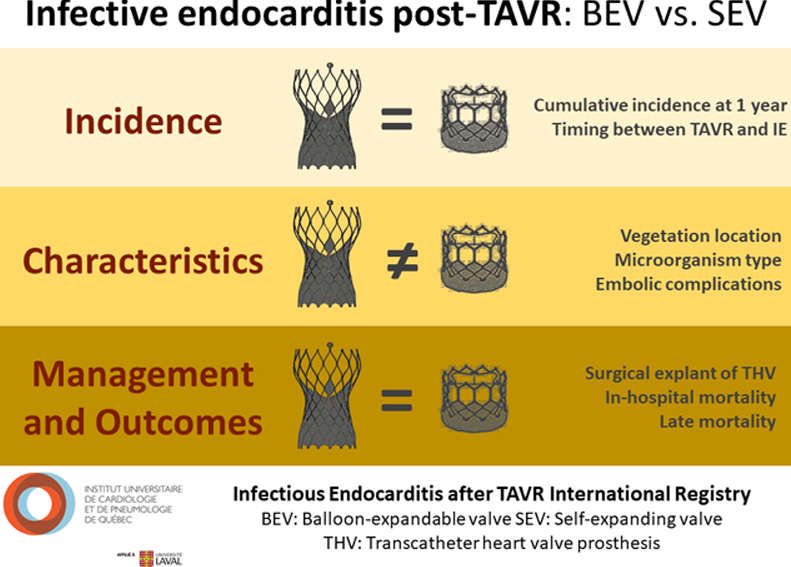
UN GRADIENT ELEVE APRÈS TAVI
N’EST PAS NORMAL – 2 SITUATIONS
1. Dès l’implantation 2. Apparition dans le suivi
Thrombose
Cela démarre mal!
Mismatch Endocardite
Dégénérescence
Conditions hémodynamiques d’augmentation du débit cardiaque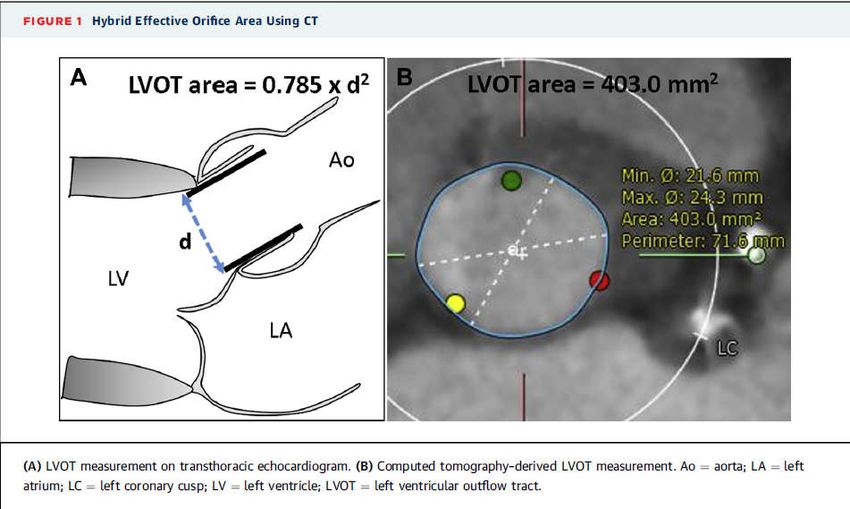
LE DIAGNOSTIC EST
INDISPENSABLE
1. Dès l’implantation 2. Apparition dans le suivi
Cela démarre mal!
Thrombose
Mismatch
Endocardite
Dégénérescence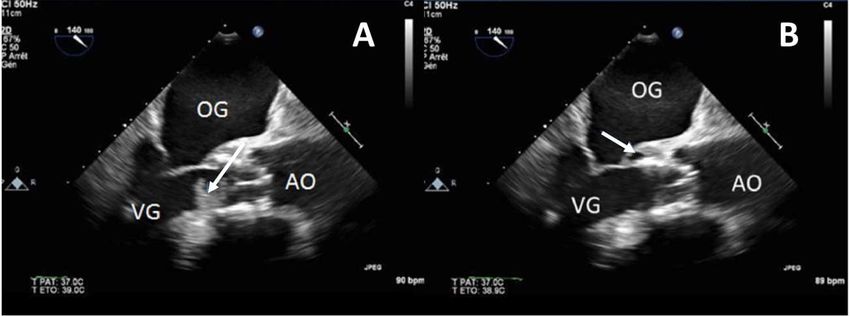
LE MISMATCH APRES TAVI
Définition:
Un « mismatch » se définit par une surface valvulaire une fois
implantée chez le patient inférieure à une valve humaine normale
La surface effective (EOA) plus petite que ne le voudrait la surface corporelle
(BSA) va donc engendrer un gradient trans-valvulaire plus élevé selon:
Gr moyen = Q²/k x EOA²
Mismatch si Sao < 0,85 cm²/m²
-Sévère si Sao < 0,65 cm²/m²
-Modéré si Sao >0,65 et
LE MISMATCH
1. Plus fréquent après chirurgie qu’après TAVI
2. Facteur de moins bon pronostic
ELEVATION DU GRADIENT DANS LE
SUIVI
1. Dès l’implantation 2. Apparition dans le suivi
Cela démarre mal!
Thrombose
Mismatch
Endocardite
Dégénérescence
LA THROMBOSE Gradient moyen = 29 mm Hg

THROMBOSE DE
BIOPROTHESE
Anticoagulation orale
Thrombose clinique < 1% prolongée
Thrombose INFRA-clinique i.e au scanner
13%
Etudes en cours: AAP, AC meilleur traitement préventif après TAVI?
Makkar RR et al. NEJM 2015:373:2015-24.
Rashid HN et al. EuroIntervention 2018;13:e1748-55. Chakraverty et al., Lancet 2017:389;2383-92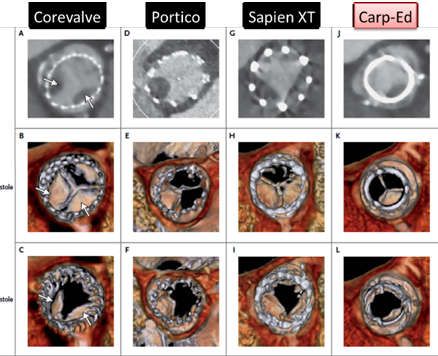
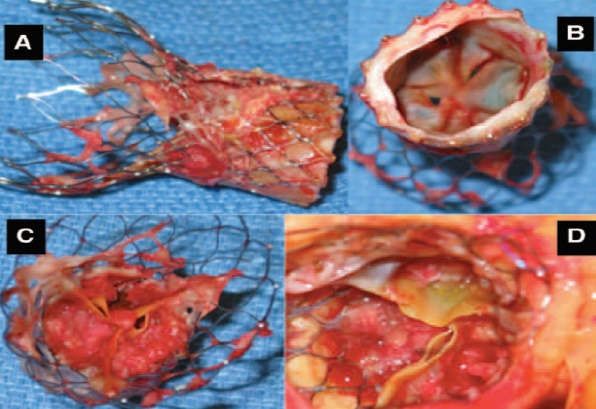
ENDOCARDITE Gradient moyen = 40 mm Hg
ENDOCARDITE
0.3-1.2% / patient / an
Localisation
Présentation cinique Feuillet (39%)
Ins cardiaque (>50%) Stent (17%)
AEG (20%) Mixte (9.2%)
Fièvre (75%) Abcès (47%)
AVC (7.5%) Fistule (9%)
Micro-organismes
Imagerie
Coagulase-negative Staph. (24.5%) ETO (végétations 50%), (négative 32%!), Gradient
Staph. Aureus (21%) Scanner (abcès, végétations)
Enterocoque (21%) 18F-FDG PET ou leucocytes marqués SPECT (>3Mo)DÉGÉNERESCENCE (SVD) Gradient moyen = 32 mm Hg
DEGENERESCENCE APRÈS TAVI
A 5 ans Au-delà de 5 ans
M Mack et al. PARTNER 1
Lancet 2015:385(9986):2477-84 7/8-y 7-8 yr
7-y
Author N Period Valve Severe Re-
Survival
SVD intervention
Eltchaninoff 378 2002-2012 BE (100%) 18% 1% 0.6%
4 .2 %
Deutch 300 2007-2009
SE (71%)
: 0 -
23.2%
.3 %
3.7% 1.3%
BE (29%)
è r e 0 - 1
r gie v
sSEé(100%) ntio35%n : 3.3%
h i r u gé Holy 152 2007-2011
D
SV eSE r(83%) e
0%
(not for SVD)
= c an v
V I ch 2007-2012int
TA n t in Barbanti 288
R é - BE (17%)
29.8% 2.4% 0.7%
ad ie
Gr
BE (84%)
Durand 1403 2002-2012 18.6% 4.2% 1%
SE (16%)
SE (64%)
Blackman 241 2007-2011 ? 0.4% 0%
BE (36%)
SE (69%)
Orwin 184 2008-2011 - 3.3% (BVF) 1.6%
BE (31%)
Circulation 2018 Panico 278 2007-2013 SE (100%) 20% 1.8% 1.1%Elévation du gradient à l’échographie
COMMENT FAIRE LE DIAGNOSTIC ?
Elévation isolée du gradient
1. Ecarter le mismatch En comparant à l’ETT post-TAVI
2 Exclure anémie, hyperthyroidie …(hyperdébit)
3 Exclure la thrombose CT-scan +/- anticoagulation orale
Exclure l’endocardite* ETO; +/- Hémocultures; +/- PET-CT
4 Probable dégénérescence* (SVD) * Surtout si IA associéeIMPORTANCE DU SUIVI DE TOUTES
LES BIOPROTHESES
ETT post-TAVI
Tous les ans
Suivi clinique + Echographie
À répéter en cas de doute
Si nécessaire: CT-scan, ETO, hémocultures, PET-scan
Participation aux registres France-TAVI et RHU STOP-AS
Participation à la recherche (innovation française)Remerciements à Adrien Sanches et Thibault Verrez
SELF VS. BALLOON-EXPANDABLE PROSTHESIS
Circulation Cardiovascular Interventions. 2019;12:e007938Isolée sans IA Associée à une IA
Thrombose ou Dégénérescence ?
dégénérescence ? Endocardite ?
Scanner
Anticoagulation ETT +/- CT
Thrombose confirmée de contrôle
per os prolongée
Dégénérescence confirmée RVA ou TAVI in TAVI si
sévèreComment suivre un patient après TAVI?
• Surveillance régulière (MT et cardiologue)
• Interrogatoire et examen clinique
• Echocardiographie trans-thoracique annuelle
En cas d’anomalies ou de doute et selon le cas:
– Scanner devant une élévation de gradient
– ETO devant l’apparition ou l’aggravation d’une IA
(centrale)
– IRM si doute sur la sévérité pour quantifier l’IA
– PET-scan si doute sur endocarditeImportance du suivi
ETT de référence Tous les ans: CS + Echographie cardiaque
à la sortie (à répéter au moindre doute)
Si nécessaire: scanner, ETO, IRM, PET-
scan
Participation à France-TAVI et au RHU STOP-AS
Participation aux études (Innovation
française/expansion/potentiel d’amélioration et de recherche)Investissements d’Avenir – RHU programme
complementary and
16 Partners multidisciplinary 5 Work packages
4 Industrials 4 UH
7 Research teams 1 Scientific society 4 Goals
1 Competitive cluster
2 Local organisations
Identify and treat the
WP2
vulnerable aortic valve
21,0 millions Animal models, biobanks,
cohorts
Full cost
Search Treatment and improve Include the cardiac
Requested 6,6
millions
Outcome WP3 impact in the therapeutic
funding
decision
of Patients Cohorts et biobanks
Project
coordinator with Aortic Stenosis
TAVI for all patients and
WP4 new non-invasive
Hélène Eltchaninoff approaches
Registries and social & economic
ROUEN University Hospital impact
Dissemination, training
126 WP5
and industrial transfer
YEARS Contributors
16 to be recruitedLe « mismatch » après RVA est associé à un moins bon pronostic chez les patients à FE altérée (< 50%) Moindre régression de la masse VG Mortalité accrue
Mais chez les Pts à FE préservée , seul le « mismatch » sévère est associé à un moins bon pronostic et ce uniquement chez les patients < 70 ans et/ou obèse
QUE NOUS OFFRENT LES BIOPROTHÈSES TAVI ?
2018
QUEL IMPACT DU « MISMATCH »
APRÈS TAVI ?
62 125 Pts
2014-2017
JACC 2018;72(22)Se méfier des limites des mesures TTE Apport du scanner pour la mesure de la chambre de chasse
Vous pouvez aussi lire

















































