Fokus Psoriasis - Dermatologica Helvetica
←
→
Transcription du contenu de la page
Si votre navigateur ne rend pas la page correctement, lisez s'il vous plaît le contenu de la page ci-dessous
AVRIL 2019
VOLUME 31 - N° 4
Fokus Psoriasis
Seite 10
Multiomics mit Stripping:
die nicht befallene Haut spricht Focus Psoriasis
Multiomics sur stripping: Page 10
la peau non lésionnelle parle
Seite/Page 8
Die Paget-Krankheit ist immer
epidermalem Ursprungs
La maladie de Paget est toujours
d’origine épidermique
Seite/Page 4
SGDV Basel Vorprogramm
SSDV Bâle pré-programme
Seite/Page 13
Seite/Page 20
Arbeitsgruppe Infektiologie / STI Klinische Fälle aus USZ
Groupe de travail infectiologie / IST Cas cliniques de USZ
Seite/Page 36 Seite/Page 40
Dieses Heft wrde für die Fortbildung der Schweizer Dermatologen dank einer Hilfe die folgenden Firmen realisiert:
Ce numéro a été réalisé grâce à une aide pour la formation continue des dermatologues suisses des firmes:
ZUR BEHANDLUNG
VON AKTINISCHEN
KERATOSEN
NEU!
EXKLUSIVES GENERIKUM
Wirkstoff: Diclofnac-Natrium
Pharmacode Menge Bezeichnung FAP*
7426305 25g Gel 30 mg/g CHF 24.30
7426311 50g Gel 30 mg/g CHF 42.80
*exkl. Mwst
Solacutan® 3% Gel Z: Diclofenac natrium (30 mg/g) I: Aktinische Keratosen. D: Erw.: 2×tgl. 0,5 g/25 cm2 während 60–90 Tagen, max. 5 g tgl. KI: Überempfindlichkeit gegenüber Diclofenac und Hilfsstoffen Schwan-
gerschaft (3. Trimenon, 1. und 2. Trimenon «FI»), Stillzeit (grossflächig, langfristig, Brust). IA: Wechselwirkungen mit Sonnenschutzpräparaten wurden nicht untersucht, weshalb eine gleichzeitige Anwendung
vermieden werden sollte. UW: Konjunktivitis, Hyperästhesie, Muskelhypertonie, lokalisierte Parästhesien, Dermatitis (einschliesslich Kontaktdermatitis), Ekzem, Hauttrockenheit, Erythem, Ödem, Juckreiz, Ausschlag,
schuppiger Hautausschlag, Hauthypertrophie, Hautulkus, vesiculo-bullöser Ausschlag. Liste: B. Stand der Information: 02/2017. Zulassungsinhaberin: Dermapharm AG, 6331 Hünenberg. Ausführliche Informationen
siehe www.swissmedicinfo.ch oder www.compendium.ch
WEISS IST NICHT GLEICH WEISS
Dermapharm AG • Bösch 104 • 6331 Hünenberg
Tel. 041 785 63 40 • Fax 041 785 62 89 • info@dermapharm.ch • www.dermapharm.ch
DH
RUBRIKEN DER DERMATOLOGICA HELVETICA –
RUBRIQUES DE DERMATOLOGICA HELVETICA
Weiterbildung – Formation continue
Redaktionsbüro, Bureau éditorial:
DERMATOLOGICA HELVETICA JH Saurat: Chefredaktor, Editeur en chef
M Harms: Chefredaktor StV, Editeur en chef adjointe
Avril 2019 - Volume 31 - N° 4 A Navarini: Assoziierter Redaktor, Rédacteur associé
C Hsu: Redaktor für die Social Media, Editeur sur les médias sociaux
Carine Herreras (derm.helv@bluewin.ch): Redaktionsbüro, Bureau éditorial
Atar Roto Presse SA, Genève: Druck, Impression
SOMMAIRE Sektionen, Sections:
JH Saurat: Journal Club, Focus
4 Journal Club Chefärzte, Médecins chef-de-service: Case reports, coups d’oeil (Koordination:
Redaktionsbüro, Coordination: Bureau rédactionel, C Herreras, derm.helv@bluewin.ch)
10 Fokus – Focus A Navarini: Peer-reviewed contributions
A Navarini: Weiterbildung der Assistenzärzte, Formation post-graduée des
16 SGDV – SSDV assistants
M Harms: Das diagnostische Photo, Photo du mois, terminologie
20 Vorprogramm – Pré-programme SSDV JP Grillet: Humor, Billet d’humour
J Hafner, C Mainetti: Tribune des Präsidenten, Tribune du président
M Tomasik: Neues aus dem Generalsekretariat, Nouvelles du secrétariat général
36 Sujets de formation post-graduée et N Griesser: Neue Mitglieder, Nouveaux membres
Neues aus den kantonalen Dermatologengesellschaften, den Kommissionen
continue und Arbeitsgruppen, Nouvelles des sociétés cantonales de dermatologie et
vénéréologie, des commissions et des groupes de travail (Koordination: Redak-
39 Terminologie tionsbüro, Coordination: Bureau éditorial, C Herreras, derm.helv@bluewin.ch)
Neues aus der Industrie, Nouvelles de l’industrie (Koordination: Redaktionsbüro,
40, 42 Reports Coordination: Bureau éditorial, C Herreras, derm.helv@bluewin.ch)
Ständige Kommission für Kommunikation, Commission permanente pour la
44, 45, 46 Portraits communication:
AK Lapointe, AM Skaria: Redaktoren Westschweiz, Editeurs députés pour la
47 Photo du mois Suisse romande
E Bianchi, F Pelloni: Redaktoren Tessin, Editeurs députés pour le Tessin
49, 50, 52, 54 Industrie B. Schlagenhauff, J Hafner: Redaktoren deutsch-sprachige Schweiz, Editeurs
députés pour la Suisse alémanique
Authors instructions (peer reviews) e-mail: derm.helv@bluewin.ch
Size: Papers should comprise approximately 700-2000 words including figures, tables and references.
Title page: The first page of each paper should indicate the title, the authors’ names, the institute where the work was conducted,
ISSN: 1420-2360
and a short title for use as running head.
Full address: The exact postal address of the corresponding author complete with postal code must be given.
Key words: For indexing purposes, a list of 3–5 key words in English is essential for all papers.
Abstract: Normally each paper needs an abstract of not more than 150 words. It should contain the following information: purpose
of the study, procedures, results, conclusions and message of the paper. Abstracts submitted for publication in the section Original
Papers should be structured as follows:
Background: What is the major problem that prompted the study
• Objective: What is the purpose of the study?
• Methods: How was the study performed?
Results: Most important findings?
• Conclusion: Most important conclusion?
Footnotes: Avoid footnotes. When essential, they are numbered consecutively and typed at the foot of the appropriate page.
Formatting rules:
• Do not use any special page layout. If you would like to see what your manuscript looks like with embedded tables and illustrati-
ANZEIGENREGIE – RÉGIE DES ANNONCES
ons, remember that we need text and illustrations as separate files!
• Enter your text continuously flush left. Do not use hard returns ("enter") within a paragraph, only at its end.
• Do not use footer and header functions.
• Use boldface and italics as well as sub- and superscript where appropriate. Carine HERRERAS
• Use your word-processing program to insert Greek letters, mathematical symbols, etc.
Legends: The legends to your figures are part of the text and should be listed at the end of your text file. Tél. +41 79 667 32 48
Line Drawings
Black and White Half-Tone Images, Color Illustrations E-mail: derm.helv@bluewin.ch
Scans
• For processing and retouching scanned half-tone images, Photoshop is recommended. Please save the original scan as well as
your processed version.
• Export black and white half-tones and color illustrations as TIF or EPS format, as close as possible to their anticipated size in print.
• Save them as separate files, not embedded in the text.
ÉDITION
• Scanned line drawings must be digitalized with a resolution of at least 800, better 1000 dpi (dots per inch) after scaling.
• Scanned half-tone images should be digitalized with a final resolution of 300 dpi, a 12 bit grayscale accuracy and a density range Dermatologica Helvetica
of 2.8. Screen values must lie between 5% and 95%.
• Scanned color illustrations must be digitalized in RGB mode with a resolution of at least 300 dpi, a 32 bit accuracy and a density JH Saurat
range of 2.8.
• Summary. 22, rue de l’Athénée
Make sure that your original has the resolution values in this table after scaling, otherwise the printing quality may be inadequate.
CH-1206 Genève
Detailled authors instruction will soon be avaible on our upcoming website.
Warnung – Avertissement
Für den Inhalt ausserhalb des redaktionellen Teils (insbesondere Anzeigen, Industrieinformationen, Pressezitate und Kongressinformationen) übernehmen Redaktion und Verlag keine Ge-
währ. Eine Markenbezeichnung kann warenzeichenrechtlich geschützt sein, auch wenn bei ihrer Verwendung in dieser Zeitschrift das Zeichen® oder ein anderer Hinweis auf etwa bestehende
Schutzrechte fehlen sollten.
L’éditeur et la rédaction déclinent toute responsabilité concernant le contenu non rédactionel du périodique (en particulier les annonces, les informations émanant de l’industrie, les citations
tirées de la presse et les informations issues de congrès). Une marque déposée peut jouir d’une protection légale même si elle est mentionée dans le périodique sans le symbole ® ou toute
autre marque signalant, le cas échéant, une telle protection juridique.
Dosierungsangaben von Medikamenten:
Autoren und Verlag haben alle Anstrengungen unternommen, um sicherzustellen, dass Auswahl und Dosierungsangaben von Medikamenten im vorliegenden Text mit den aktuellen Vor-
schriften und der Praxis übereinstimmen. Trotzdem muss der Leser im Hinblick auf den Stand der Forschung, Änderungen staatlicher Gesetzgebungen und den unterbrochenen Fluss neuer
Forschungsergeenisse bezüglich Medikamentenwirkung und -nebenwirkungen darauf aufmerksam gemacht werden, dass unbedingt bei jedem Medikament der Packungsprospekt konsul-
tiert werden muss, um mögliche Änderungen im Hinblick auf Indikation und Dosis nicht zu übersehen. Gleiches gilt für spezielle Warnungen und Vorsichtsmassnahmen. Ganz besonders gilt
dieser Hinweis für empfohlene neue und/oder nur selten gebrauchte Wirkstoffe.
Alle Rechte vorbehalten. Ohne schriftliche Genehmigung des Verlags dürfen diese Publikation oder Teile daraus nicht in andere Sprachen übersetzt oder in irgendeiner Form mit mecha-
nischen oder elektronischen Mitteln (einschliesslich Fotokopie, Tonaufnahme und Mikrokopie) reproduziert oder auf einem Datenträger oder einem Computersystem gespeichert werden.
Posologie des médicaments:
Les auteurs et l’éditeur ont tout mis en œuvre pour s’assurer que le choix des médicaments et la posologie préconisés dans ce texte soient conformes aux recommandations et à la pratique
au moment de la publication. Cependant, compte tenu des recherches en cours, des changements dans les législations et de l’afflux constant de données nouvelles concernant la thérapie
médicamenteuse et l’effet des médicaments, il est vivement recommandé au lecteur de vérifier sur la notice jointe à chaque emballage si aucune modification n’est intervenue dans la poso-
logie et si aucune nouvelle contre-indication ou précaution à prendre n’a été signalée. Cela est particulièrement important lorsque l’agent recommandé est nouveau ou peu employé. Tous
droits de reproduction, même partielle, sous n’importe quelle forme, strictement réservés.
Dermatologica Helvetica - Volume 31(4) - Avril 2019 3
ratios (ORs) with 95% confidence intervals. Both
Warts Escape The Immune conventional and network meta-analyses (with
System Just Like Melanoma a frequentist approach) were conducted on R
software. The P-score was used to rank different
Expression of PD-L1 and PD-1 in Cutaneous Warts treatments.
Results: Network meta-analysis of 17 rando-
W.Y. Yu, et al. mized controlled trials (1676 patients) showed
Department of Dermatology, University of Cali- that PPD (purified protein derivative vaccine, OR
fornia, San Francisco, USA 39.56), MMR (measles, mumps, rubella vaccine,
OR 17.46) and interferon β (OR 15.55) had the
Background: Cutaneous warts have high preva- highest efficacy in terms of complete recovery
lence and cause significant morbidity. Unders- at the primary site compared with placebo. Re-
tanding the mechanisms by which warts evade garding complete recovery at the distant site,
the immune system may lead to targeted and autoinoculation (OR 79.95), PPD (OR 42.95), and
improved treatments. MMR (OR 15.39) were all statistically superior
Objective: To determine whether cutaneous war- to placebo. According to the P-score, MMR was
more effective than other modalities in reducing
S e l e c t e d b y J H S AU R AT
ts express programmed death ligand 1 (PD-L1)
and to characterize expression of programmed the recurrence rate at the same site.
death 1 (PD-1) within the immune infiltrate in in- Limitations: Relatively small sample size in some
flamed lesions. comparisons and variability in baseline characte-
Methods: 44 biopsies of cutaneous warts were ristics.
retrieved from the Department of Dermatopa- Conclusion: PPD and MMR were the most effec-
thology archives of the University of California, tive in achieving complete primary and distant
San Francisco. Biopsies were stained with he- recovery (along with autoinoculation for distant
matoxylin and eosin, anti-PD-L1 monoclonal recovery) and reducing the recurrence rate at the
antibody, and inflamed cases were stained with same site compared with cryotherapy and other
anti-PD-1 monoclonal antibody. immunotherapeutic modalities.
Results: PD-L1 was expressed on keratinocytes
in cases of verrucae vulgares (12/30, 40%) and Journal of the American Academy of Dermatolo-
myrmecia (7/14, 50%), and was associated with gy, 2019, 80, Issue 4, 922-930.e4
an interface inflammatory reaction. PD-1 was ex-
pressed by the inflammatory infiltrate in verrucae
vulgares (21/24, 88%) and myrmecia (5/8, 63%).
Limitations: This was a retrospective observatio-
nal study conducted at a single institution.
Conclusions and Relevance: Many cutaneous
The Epidermal Origin for
warts express PD-L1, suggesting that HPV may
use this pathway to promote immune dysfunc-
Paget’s Disease Proven
tion. This discovery may help to explain the re- By Genomics
J O U R N A L C LU B
calcitrance of warts to current therapies and pro-
vides a rationale for investigating anti-PD-1 im- Whole-Exome Sequencing Reveals Frequent Mu-
munotherapy as a potential treatment for warts. tations in Chromatin Remodeling Genes in Mam-
mary and Extramammary Paget’s Diseases
Journal of the American Academy of Dermatolo-
gy, 2019. G. Zhang, et al.
Doi: https://doi.org/10.1016/j.jaad.2019.02.063. Department of Pathology, Shantou University
Medical College, Shantou, Guangdong, China
Paget's disease (PD) is an intraepidermal adeno-
carcinoma of the skin at the breast (mammary
PD) or urogenital locations (extramammary PD
Intralesional Immunotherapy [EMPD]). At present, there is lack of clarity on
PD’s pathogenesis, the relationship between its
of Warts. Should be Promoted? subtypes, and its lineage link with the under-
lying invasive carcinomas. Here we describe that
Intralesional immunotherapy for the treatment
mammary PD and EMPD have similar mutational
of warts: A network meta-analysis
profiles, with the most frequent recurrent mu-
tations occurring in the chromatin remodeling
S. Salman, et al.
genes, such as KMT2C (MLL3, 39%) and ARID2
Department of Dermatology and Venereology,
(22%), with additional recurrent somatic muta-
Tanta University Hospital, Faculty of Medicine,
Tanta, Egypt
Background: Without clear evidence, selecting
among the existing immunotherapeutic options
for warts remains challenging.
Objective: Through network meta-analyses, we
aimed to evaluate the comparative efficacy of
different intralesional immunotherapeutic mo-
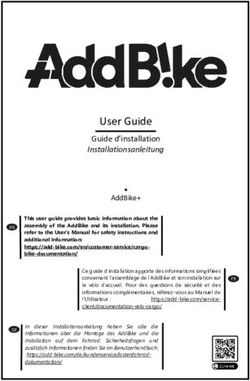
Figure 1. KMT2C, the most highly mutated gene in Pa-
dalities. get’s disease, is a histone methyltransferase that typi-
Methods: We included randomized controlled cally catalyzes H3K4me1 at gene enhancers to poise
trials comparing intralesional immunotherapeu- enhancers for gene activation, loosening the overall
tic modalities to cryotherapy, placebo, or imi- chromatin structure in order to more easily allow gene
quimod. All outcomes were presented as odds transcription to occur
4 Dermatologica Helvetica - Volume 31(4) - Avril 2019
Neu
bei
Plaque-
*, 1
Psoriasis
i s che
Dimethylfumarat
te m e
Sys rst-Lin *, 1
Fi rapie
Erste orale Fumarat-Therapie The
bei Plaque-Psoriasis*, 1
O Wirksame Therapie1–5
O Individualisierte Anwendung1, 2, 6
O Fumarate – bewährt in der Langzeittherapie4, 7, 8
almirall.ch
Referenzen: * Skilarence® Indikationen/Anwendungsmöglichkeiten: Skilarence® wird angewendet zur ausschliesslichen Behandlung von Hautmanifestationen erwachsener Patienten mit mittelschwerer bis schwerer Plaque-
Psoriasis, die eine systemische Arzneimitteltherapie benötigen.1. Fachinformation Skilarence®. http://swissmedicinfo.ch; Stand: Oktober 2018 2. U. Mrowietz et al., Efficacy and safety of LAS41008 (dimethyl fumarate) in
adults with moderate-to-severe chronic plaque psoriasis: a randomized, double-blind, Fumaderm®- and placebo-controlled trial (BRIDGE); Br J Dermatol. 2016 Aug;176(3):615-623 3. Ghoreschi K, et al., Fumarates improve
psoriasis and multiple sclerosis by inducing type II dendritic cells. J Exp Med. 2011 Oct 24;208(11):2291-303 4. Antonios G.A. Kolios et al., Swiss S1 Guidelines on the Systemic Treatment of Psoriasis Vulgaris; Consensus
Guidelines; Dermatology 2016; 232: 385–406 DOI: 10.1159/000445681 5. Thaçi D et al., Efficacy and safety of fumaric acid esters in patients with psoriasis on medication for comorbid conditions - a retrospective evaluation,
J Dtsch Dermatol Ges. 2013 May;11(5): 429–35. doi: 10.1111/ddg.12059. Epub 2013 Feb 21 6. U. Mrowietz et al. Dimethylfumarate for psoriasis: more than a dietary curiosity. Trends mol med 2005; 11 (1): 43–48. 7. D.
Pathirana et al., European S3-Guidlines on the systemic treatment of psoriasis vulgaris—Update 2015—EDF in cooperation with EADV and IPC. European Dermatology Forum Guidelines [Online] 2015 [Updated]. Available
at: https://onlinelibrary.wiley.com/doi/epdf/10.1111/j.1468-3083.2009.03389.x 8. Fachinformation Fumaderm® https://www.dimdi.de/dynamic/de/startseite Stand: Februar 2018
Kurzfassung Fachinformation: Skilarence® 30 mg magensaftresistente Tabletten / Skilarence® 120 mg magensaftresistente Tabletten. Z: 1 Tablette Skilarence® 30 mg enthält 30 mg Dimethylfumarat. 1 Tablette Skilarence® 120
mg enthält 120 mg Dimethylfumarat. Sonstige Bestandteile: Kern: Lactose-Monohydrat, mikrokristalline Cellulose, Croscarmellose-Natrium, hochdisperses Siliciumdioxid, Magnesiumstearat; Beschichtung: Methacrylsäure-
Ethylacrylat-Copolymer (1:1), Talkum, Triethylcitrat, Titandioxid (E171), Simethicon, Skilarence® 120 mg zusätzlich: Indigocarmin (E132), Natriumhydroxid. I: Ausschliessliche Behandlung von Hautmanifestationen erwachsener
Patienten mit mittelschwerer bis schwerer Plaque-Psoriasis, die eine systemische Arzneimitteltherapie benötigen. D/A: Zum Einnehmen im Ganzen während oder unmittelbar nach einer Mahlzeit. Behandlung mit niedriger
Anfangsdosis beginnen, dann schrittweise steigern. Vor und während der Behandlung Blutbild, Nierenfunktion und Urinstatus sowie Leberwerte regelmässig kontrollieren, ggfls. Dosis anpassen. KI: Überempfindlichkeit gegen
den Wirkstoff oder einen der Hilfsstoffe, schwere Erkrankungen des Gastrointestinaltraktes, schwere Leber- oder Nierenfunktionsstörungen, Schwangerschaft und Stillzeit, Leukopenie < 3,0 x 109/l, Lymphopenie < 1,0 x 109/l
(bei Therapiebeginn), bekannte Infektion mit dem Humanen Immundefizienz-Virus (HIV), bekannte schwere aktive Infektionen (z.B. Tuberkulose, Hepatitis B und C), progressive multifokale Leukenzephalopathie (PML) oder
Verdacht auf PML, gleichzeitige Behandlung mit systemischen Anticholinergika. VM: Vor Behandlung: Es muss ein grosses Blutbild (einschliesslich Differentialblutbild und Thrombozytenzahl) vorliegen. Während der Behandlung:
in den ersten 4 Monaten alle 4 Wochen und danach alle 8 Wochen ein grosses Blutbild mit Differentialblutbild erstellen. Handlungsbedarf bei Leukopenie/Lymphopenie gemäss ausführlicher Fachinformation. Bei schweren
CHDMF0424DeMärz2019
Infektionen während der Behandlung ist eine Unterbrechung der Therapie zu erwägen. Monolithische Tabletten können bei unvollständiger Entleerung im Magen akkumulieren (nicht vorhersehbare Magendarmpassage und
Resorption). Skilarence® enthält Lactose. Patienten mit der seltenen hereditären Galactose-Intoleranz, Lactase-Mangel oder Glucose-Galactose-Malabsorption sollten dieses Arzneimittel nicht einnehmen. IA: Es wurden
keine Studien zur Erfassung von Interaktionen durchgeführt. Kombination mit anderen systemischen Psoriasis-Therapien (z. B. Methotrexat, Retinoide, Psoralene, Ciclosporin, Immunsuppressiva oder Zytostatika), anderen
Fumarsäurederivaten (topisch oder systemisch), oder nephrotoxischen Substanzen (z. B. Aminoglycoside, Diuretika, NSARs oder Lithium) vermeiden. Schwerwiegende oder anhaltende Diarrhö kann die Resorption anderer
Arzneimittel beinträchtigen. Die Wirksamkeit oraler Kontrazeptiva kann vermindert sein. Übermässigen Konsum (über 50 ml) von starken alkoholischen Getränken vermeiden. Impfungen während der Behandlung mit
Skilarence® wurden nicht untersucht. Eine Immunsuppression gilt als Risikofaktor für die Anwendung von Lebendimpfstoffen. SS/SZ: Anwendung nicht empfohlen bei Frauen im gebärfähigen Alter, die keine angemessene
Verhütungsmethode verwenden. Skilarence® ist während der Schwangerschaft und Stillzeit kontraindiziert. UW: Sehr häufig: Lymphopenie (10,0 %), Leukopenie, Flush-Symptomatik (20,8 %), Diarrhö (36,9 %), abdominale
Distension, Bauchschmerzen (40,1 %), Übelkeit (10,8 %). Häufig: Eosinophilie, Leukozytose, verringerter Appetit, Kopfschmerzen, Parästhesie, Erbrechen, Dyspepsie, Obstipation, abdominelle Missempfindung, Flatulenz,
Erythem, brennendes Gefühl auf der Haut, Pruritus, Fatigue, Hitzegefühl, Asthenie, erhöhte Leberenzymwerte. UW < 1% siehe www. swissmedicinfo.ch. P: Skilarence® 30 mg: 42 magensaftresistente Tabletten, Skilarence®
120 mg: 90 und 180 magensaftresistente Tabletten, Abgabekategorie: B. Ausführliche Informationen siehe Packungsbeilage oder www.swissmedicinfo.ch, Stand der Information: Oktober 2018 ZI: Almirall AG, Alte
Winterthurerstr. 14, 8304 Wallisellen.
tions detected in genes previously not known to are needed to confirm these observations of va-
be mutated in cancers, such as CDCC168 (34%), riable responses.
FSIP2 (29%), CASP8AP2 (29%), and BIRC6 (24%).
In paired mammary PD and underlying breast Journal of the European Academy of Dermatolo-
carcinoma samples, distinct gene mutations gy and Venereology. 2019.
were detected, indicating that they represent Doi: 10.1111/jdv.15457.
independent oncogenic events. Finally, multis-
tage EMPD tissue sequencing revealed KMT2C
gene occurring early in EMPD oncogenesis, and
that multifocal EMPD samples share the same
early gene mutations, suggesting clonal origin
of multifocal EMPD. Our results reveal similar ge- Antibiotic Use by
nomic landscapes between mammary PD and
EMPD, including early aberrations in chromatin
Dermatologists is Declining
remodeling genes. In addition, mammary PD and but the Use after Surgical Visits
underlying breast ductal carcinomas represent
independent oncogenic events. These findings is Increasing
provide approaches for developing diagnostic
tools and therapeutic interventions for PD. Trends in Oral Antibiotic Prescription in Dermato-
logy, 2008 to 2016
Journal of Investigative Dermatology, 2019, 139,
Issue 4, 789-795. JS. Barbieri, et al.
Department of Dermatology, University of
Pennsylvania Perelman School of Medicine, Phi-
ladelphia.
Importance: Dermatologists prescribe more oral
Naltrexone in Darier Disease: antibiotic courses per clinician than any other
specialty, and this use puts patients at risk of an-
Not as good as in Hailey Hailey tibiotic-resistant infections and antibiotic-asso-
ciated adverse events.
Variable response to low-dose naltrexone in pa- Objective: To characterize the temporal trends in
tients with Darier disease: a case series the diagnoses most commonly associated with
oral antibiotic prescription by dermatologists, as
D. Boehmer, etal. well as the duration of this use.
Dermatology, Technical University of Munich, Design, Setting, and Participants: Repeated
Munich, Germany cross-sectional analysis of antibiotic prescribing
by dermatologists from January 1, 2008, to De-
Background: Darier disease is a rare autoso- cember 31, 2016. The setting was Optum Clin-
mal-dominant genodermatosis with a loss formatics Data Mart (Eden Prairie, Minnesota)
of function of a Ca2+ -ATPase pump (SER- deidentified commercial claims data. Participants
CA2-pump). Clinically, the disease is characte- were dermatology clinicians identified by their
rized by red-brown keratotic papules mainly in National Uniform Claim Committee taxonomy
seborrhoeic areas and has only limited and un- codes, and courses of oral antibiotics prescribed
satisfactory treatment options. Previously, low- by these clinicians were identified by their Natio-
dose naltrexone was described as a successful nal Drug Codes.
treatment option in Hailey-Hailey disease, a ge- Exposures: Claims for oral antibiotic prescrip-
nodermatosis with a genetic mutation coding for tions were consolidated into courses of therapy
a similar loss of function of a Ca2+ -ATPase pump and associated with the primary diagnosis from
(hSPCA1-pump). the most recent visit. Courses were stratified into
Objective: To assess the efficacy of low-dose nal- those of extended duration (>28 days) and those
trexone as a treatment option in Darier disease. of short duration (≤28 days).
Methods: Six patients with biopsy-proven Darier Main Outcomes and Measures: Frequency of an-
disease (four had severe, one had moderate and tibiotic prescribing and associated diagnoses.
one mild clinical manifestations). The patients Poisson regression models were used to assess
received off-label therapy with naltrexone [5 mg for changes in the frequency of antibiotic pres-
per os (p.o.)] and magnesium [200 mg p.o.]. Pa- cribing over time.
tients were followed up every 4 weeks for mini- Results: Between 2008 and 2016 among 985 866
mally 12 weeks. Upon clinical presentation, the courses of oral antibiotics prescribed by 11 986
disease severity and subjective pain and itch unique dermatologists, overall antibiotic pres-
scores were assessed, and standardized photo- cribing among dermatologists decreased 36.6%
J O U R N A L C LU B
graphs were obtained. (1.23 courses per 100 visits) from 3.36 (95% CI,
Results: The clinical response to naltrexone va- 3.34-3.38) to 2.13 (95% CI, 2.12-2.14) courses per
ried after 12 weeks. The four patients with severe 100 visits with a dermatologist (prevalence rate
Darier disease showed worsening after initial ratio for annual change, 0.931; 95% CI, 0.930-
improvement during the first 4 weeks, whereas 0.932), with much of this decrease occurring
the two patients with a mild to moderate clinical among extended courses for acne and rosacea.
manifestation clearly improved, showing almost Oral antibiotic use associated with surgical visits
full remission after 12 weeks with complete flat- increased 69.6% (2.73 courses per 100 visits) from
tening of the keratotic papules. 3.92 (95% CI, 3.83-4.01) to 6.65 (95% CI, 6.57-6.74)
Conclusion: Low-dose naltrexone did not have courses per 100 visits associated with a surgical
an effect on severe Darier disease compared to visit (prevalence rate ratio, 1.061; 95% CI, 1.059-
Hailey-Hailey disease, but it was beneficial in mild 1.063).
to moderate forms of the disease. Further studies
6 Dermatologica Helvetica - Volume 31(4) - Avril 2019
Conclusions and Relevance: Continuing to deve-
lop alternatives to oral antibiotics for noninfec-
NOTABLE NOTE
tious conditions, such as acne, can improve an-
tibiotic stewardship and decrease complications
Valaciclovir: a culprit drug for drug reaction
from antibiotic use. In addition, the rising use of
with eosinophilia and systemic symptoms not
postoperative antibiotics after surgical visits is
to be neglected
concerning and may put patients at unnecessary
risk of adverse events. Future studies are needed
We describe three cases of drug reaction with eo-
to identify the value of this practice and the risk
sinophilia and systemic symptoms (DRESS) with
of adverse events.
proven causality by valaciclovir, illustrating this
risk.
JAMA Dermatology, 2019.
Valaciclovir as a possible cause of DRESS may be
Doi: 10.1001/jamadermatol.2018.4944.
neglected due to its weak notoriety and frequent
association with more highrisk drugs, such as
allopurinol or cotrimoxazole, especially in hae-
matological diseases, as illustrated by two of
our cases. The finding of drug causality based on
An Enzyme Defect in chronological criteria should be considered with
this drug, and it should be included in the further
Disseminated Superficial allergological exploration of these patients.
Actinic Porokeratosis British Journal of Dermatology, 2019, 180, pp666–
667.
Novel mutations in mevalonate kinase cause dis-
seminated superficial actinic porokeratosis
T. Zhu, et al.
Center for Medical Genetics, School of Life Frequency of acne in lactoseintolerant adults:
Sciences, Central South University, Changsha, a retrospective cross-sectional analysis within a
Hunan, China. large Midwestern US patient population
BACKGROUND: Disseminated superficial actinic The aim of this study is to assess the frequency of
porokeratosis (DSAP) is a rare autosomal domi- acne in a large lactose-intolerant (LI) US patient
nant disease. In our previous research, we found population diagnosed with acne compared to a
that a linkage region of DSAP in a large family is non-LI patient population with acne in order to
located at 12q23·2-q24·1. Subsequently, the me- provide further insight into dairy consumption
valonate kinase gene (MVK) was shown to be pa- and acne. Findings in this study for both a signifi-
thogenic in DSAP. cantly lower frequency of acne and a less severe
OBJECTIVES: To elucidate the mechanism by acne, in LI patients compared to non-LI patients
which MVK mutations lead to keratinocyte apop- with acne, contribute to the limited existing lite-
tosis and DSAP, and to report a new missense mu- rature regarding dairy and acne. Importantly, this
tation, c.566 C>T (p.A189V), in MVK in a Chinese is the first study to utilize physician-designated
DSAP pedigree. diagnostic coding for LI as a measure of dairy ex-
METHODS: The half-life of wild-type (WT) MVK posure. Further exploration of the role for IGF-1
protein and mutants was assessed using cy- and an association between acne and dairy in-
cloheximide treatment of cells. Dimerization of take seems warranted.
MVK was analysed by coimmunoprecipitation
and glutathione S transferase pull-down assay. Journal of the European Academy of Dermatolo-
MVK kinase activity, production of cell choleste- gy and Venereology, 2019.
rol, mitochondrial complex activity and apopto- Doi: 10.1111/jdv.15441.
sis were detected, using the corresponding com-
mercial kits, in cells overexpressing MVK WT and
mutants.
RESULTS: Mechanically, we demonstrated that
both the pathogenic p.A189V mutant and a spo-
radic mutation p.H312R (c.935A>G), which we
reported previously, have rapid degradation, de- "It is not how much you read, but what you
creased kinase activity and reduced production read that counts"
of cell cholesterol. Also, we found the p.H312R
mutation confers on the MVK protein an inability Shelley, Walter B. "Advanced Dermatologic
J O U R N A L C LU B
to dimerize. Further, we demonstrated that the Diagnosis"
mutants are impaired in mitochondrial function W.B. Saunders 1992
and lead to increased apoptosis.
CONCLUSIONS: Our results provide an important
basis for elucidating the mechanism by which
MVK missense mutations contribute to DSAP.
British Journal of Dermatology, 2018.
Doi: 10.1111/bjd.17596.
Dermatologica Helvetica - Volume 31(4) - Avril 2019 7
grin and the proportion of ω-hydroxy fatty acid
New Dimension in Clinical sphingosine ceramide content in nonlesional
Research: Getting Big Data skin of children with AD FA+ were substantially
lower than in AD FA− and NA skin. These abnor-
From Normal Skin Superficial malities correlated with morphologic changes
in epidermal lamellar bilayer architecture res-
Stripping ponsible for barrier homeostasis. Shotgun me-
tagenomic studies revealed that the nonlesional
The nonlesional skin surface distinguishes atopic skin of AD FA+ had increased abundance of Sta-
dermatitis with food allergy as a unique endo- phylococcus aureus compared to NA. Increased
type expression of keratins 5, 14, and 16 indicative of
hyperproliferative keratinocytes was observed in
D.Y.M. Leung, et al. the SC of AD FA+. The skin transcriptome of AD
National Jewish Health, Denver, USA. FA+ had increased gene expression for dendritic
cells and type 2 immune pathways. A network
Skin barrier dysfunction has been reported in analysis revealed keratins 5, 14, and 16 were po-
both atopic dermatitis (AD) and food allergy sitively correlated with AD FA+, whereas filaggrin
(FA). However, only one-third of patients with AD breakdown products were negatively correlated
have FA. The purpose of this study was to use a with AD FA+. These data suggest that the most
minimally invasive skin tape strip sampling me- superficial compartment of nonlesional skin in
thod and a multiomics approach to determine AD FA+ has unique properties associated with an
whether children with AD and FA (AD FA+) have immature skin barrier and type 2 immune acti-
stratum corneum (SC) abnormalities that distin- vation.
guish them from AD without FA (AD FA−) and
nonatopic (NA) controls. Transepidermal water Science Translational Medicine, 2019, 11, 480,
loss was found to be increased in AD FA+. Filag- eaav2685.
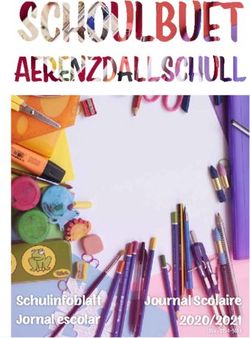
Fig. 5. Keratin expression in nonlesional skin. Comparisons between groups for markers of keratin expression mea-
sured as cumulative reporter ion signal to noise: KRT5 (A), KRT14 (B), and KRT16 (C) all assessed at skin tapes 15
and 16 on nonlesional skin. In the boxplot, the solid horizontal line represents the median, and the filled circle
represents the mean. The box margins are the interquartile range, and the whiskers extend 1.5 times the interquar-
tile range. Observations outside the whisker are marked by an open circle. The annotations are the P values from
pairwise comparisons between groups obtained from a one-way ANOVA.
Fig. 7. Network and relative impor-
tance analyses. Network (A) of the
intercorrelations between the mea-
surements of TEWL (TEWL), total UCA
(UCA), PCA (PCA), EOS CER/NS CER
ratio (EOSNS), AD severity indices
(EASI, NESS, and SCORAD), keratin
expression (KRT5, KRT14, and KRT16),
transcriptome PC1 (TPC1), the relative
abundance of S. aureus (SAUR) and
S. hominis (SHOM), and an indicator
variable for AD FA+ (yes/no) based
J O U R N A L C LU B
on peanut wheal size of ≥8 mm. TEWL
measurements were done at STS 15;
UCA, PCA and EOS CER/NS CER ratio
were evaluated at STS layers 15 and
16. The color saturation and the width
of the connecting lines correspond to
the strength of the Pearson correla-
tion coefficient, and the color of each
connecting line indicates a positive
(red) or negative (blue) correlation.
Connecting lines are only shown for
significant Pearson correlations (P <
0.01). Relative importance for predic-
tion of AD FA+ (B) and TEWL STS 15 (C).
8 Dermatologica Helvetica - Volume 31(4) - Avril 2019
BEWÄHRT BEI
PLAQUE-PSORIASIS*
NEU BEI PSORIASIS-
ARTHRITIS+
Wirksam ab Woche 11,2
Klinische Erfahrung bis zu 3 Jahren3,4
Gut verträglich
vergleichbar zu Stelara® 5 und Enbrel®2
NEU ri a s i s -
bei Psoritis+
Ar th
* Mittelschwere bis schwere Plaque-Psoriasis
+ Aktive Psoriasis-Arthritis
Stelara®, Ustekinumab, Zulassungsinhaberin Janssen-Cilag AG. Enbrel®, Etanercept, Zulassunginhaberin Pfizer AG.
* Taltz® ist zur Behandlung erwachsener Patienten mit mittelschwerer bis schwerer Plaque-Psoriasis indiziert, die auf andere systemische Therapien (einschliesslich Ciclosporin oder Methotrexat oder PUVA) nicht angesprochen
haben, bei denen diese Therapien kontraindiziert sind oder die diese Therapien nicht tolerieren. + Taltz®, alleine oder in Kombination mit konventionellen krankheitsmodifizierenden Antirheumatika (DMARD), ist zur Behandlung
erwachsener Patienten mit aktiver Psoriasis-Arthritis indiziert, die auf eine Behandlung mit einem oder mehreren DMARDs unzureichend angesprochen haben oder diese nicht vertragen haben.
1. Mease et al, Ixekizumab, an interleukin-17A specific monoclonal antibody, for the treatment of biologic-naive patients with active psoriatic arthritis: results from the 24-week randomised, double-blind, placebo-controlled and
active (adalimumab)-controlled period of the phase III trial SPIRIT-P1, Annals of the Rheumatic Diseases 2017;76:79-87. 2. Griffiths et al, Comparison of ixekizumab with etanercept or placebo in moderate-to-severe psoriasis
(UNCOVER-2 and UNCOVER-3): results from two phase 3 randomised trials, Lancet 2015; 386: 541–51. 3. Leonardi C, et al. Maintenance of Skin Clearance With Ixekizumab Treatment of Psoriasis: Three-Year Results From the
UNCOVER-3 Study. JAAD (2018), doi: 10.1016/j.jaad.2018.05.032. 4. Chandran V et al. Efficacy and Safety of Ixekizumab in Patients With Active Psoriatic Arthritis: Three Year Results From a Phase 3 Study (SPIRIT-P1), Poster
THU0333, EULAR Congress 2018, Amsterdam. 5. Reich K, et al. Comparison of ixekizumab with ustekinumab inmoderate-to-severe psoriasis: 24-week results from IXORA-S, a phase III study. British Journal of Dermatology.
2017;177;1014–1023.
Taltz® (Ixekizumab) Injektionslösung. I: Taltz ist zur Behandlung erwachsener Patienten mit mittelschwerer bis schwerer Plaque-Psoriasis indiziert, die auf andere systemische Therapien (einschliesslich Ciclosporin oder Methotrexat
oder PUVA) nicht angesprochen haben, bei denen diese Therapien kontraindiziert sind oder die diese Therapien nicht tolerieren. Taltz, alleine oder in Kombination mit konventionellen krankheitsmodifizierenden Antirheumatika
(DMARD), ist zur Behandlung erwachsener Patienten mit aktiver Psoriasis-Arthritis indiziert, die auf eine Behandlung mit einem oder mehreren DMARDs unzureichend angesprochen haben oder diese nicht vertragen haben. D:
Plaque-Psoriasis: die empfohlene Dosis beträgt 160mg als subkutane Injektion (zwei 80mg Injektionen) in Woche 0, gefolgt von 80mg (eine Injektion) in den Wochen 2, 4, 6, 8, 10 und 12, und danach 80mg (eine Injektion) alle
4 Wochen. Bei Patienten
Background: Plaque psoriasis, a chronic inflammato-
Cutaneous Lymphomas ry disease primarily affecting the skin, is thought to
Appearing Under Biologics. have a multifactorial etiology, including innate im-
mune system dysregulation, environmental triggers,
Side Effect or Mis-Diagnosis and genetic susceptibility.
Purpose: We sought to further understand the role of
Cutaneous lymphomas appearing under biologics: skin microbiota in psoriasis pathogenesis, as well as
44 cases from the French Study Group on Cutaneous their response to therapy. We systematically analy-
Lymphomas and French Pharmacovigilance Da- zed dynamic microbiota colonizing psoriasis lesions
Psoriasis inflammation autoimmunity
tabase and adjacent nonlesional skin in 114 patients prior
to and during ustekinumab treatment in a Phase 3b
L. Dequidt. Et al. clinical trial.
Dermatology Department, University Hospital, Bor- Results: By sequencing the bacterial 16S ribosomal
deaux, University of Bordeaux, France RNA gene from skin swab samples obtained at six
anatomical sites, we identified minor, site-specific
Controversy exists regarding the risk and prognosis differences in microbial diversity and composition
of lymphomas under biologics. Risk evaluation must between pretreatment lesional and nonlesional skin.
consider the underlying medical condition -as chro- During therapy, microbial communities within lesio-
nic inflammatory diseases are associated with an nal and nonlesional skin diverged, and body-site dis-
excess risk of lymphoma- and ongoing treatments persion increased, reflecting microbial skin site-spe-
(azathioprine, cyclosporine). To date, a few isolated cificity. Microbiota demonstrated greater pretreat-
cases and two small series of primary cutaneous ment heterogeneity in psoriatic lesions than in non-
lymphomas (PCL) under biologics- mostly mycosis lesional skin, and variance increased as treatment
fungoides (MF) - have been reported. Our purpo- progressed. Microbiota colonizing recurrent lesions
se was to describe PCL under biologics outsourced did not overlap with pretreatment lesional microbio-
from 2 national registries in order to evaluate their ta, suggesting colonization patterns varied between
behaviour and to propose management recommen- initial and recurrent psoriatic lesions.
dation. We conducted a retrospective multicentre Conclusions: While plaque psoriasis does not appear
declarative study based on the files of the French to be associated with specific microbes and/or mi-
Study Group on Cutaneous Lymphomas (8,364 pa- crobial diversity, this large dataset provides insight
tients registered between 2010 and 2017), and from into microbial variation associated with 1) disease in
the French Pharmacovigilance Database among all different body locations, 2) initial versus recurrent le-
events reported under biologics from 2000 to 2017. sions, and 3) antiinterleukin-12/23 therapy.
The following data were collected: patient (age at
PCL diagnosis, dermatological history, previous or Journal of Investigative Dermatology, 2018.
current immunosuppressive treatment, disease jus- Doi: 10.1016/j.jid.2018.03.1501.
tifying biologics), biologic subtype and PCL (time
to onset after initiation of biologics, subtype, stage,
outcome). We describe 44 PCL under biologics,
which represents the larger case-series to date. In
this declarative "real-life" study, PCL were of various Higher BMI Leads to a Higher
types, mostly but not exclusively represented by MF,
as in non-exposed patients. Interestingly, 13 of the 24
Risk of Psoriasis
patients with MF had a previous dermatosis, mostly Evidence of a causal relationship between body
psoriasis, but that was the indication for biologics mass index and psoriasis: A mendelian randomiza-
in only 6 cases. Patients with limited MF stage had tion study.
mostly a non-dermatological indication for biologics
and an indolent outcome. Conversely, the MF beha- A. Budu-Aggrey, et al.
ved aggressively when the indication for biologics Medical Research Council (MRC) Integrative Epide-
was uncontrolled psoriasis. This leads us to identify miology Unit, University of Bristol, Bristol, United
three scenarios: 1. pre-existing MF misdiagnosed as Kingdom.
psoriasis with an aggressive outcome (aggravating
role of biologics); 2. coexistence of MF and psoriasis Background: Psoriasis is a common inflammatory
(the biologic improves the psoriasis and reveals MF skin disease that has been reported to be associated
lesions); 3. MF de novo (either fortuitous or trigge- with obesity. We aimed to investigate a possible cau-
S e l e c t e d b y J H S AU R AT
red by biologics on a predisposed background). This sal relationship between body mass index (BMI) and
occurs mainly in patients treated for rheumatism or psoriasis.
inflammatory colitis.
FOCUS -
Methods and findings: Following a review of publi-
shed epidemiological evidence of the association
Doi: 10.1111/bjd.17834. between obesity and psoriasis, mendelian randomi-
zation (MR) was used to test for a causal relationship
with BMI. We used a genetic instrument comprising
97 single-nucleotide polymorphisms (SNPs) asso-
Skin Microbiome Diversity ciated with BMI as a proxy for BMI (expected to be
much less confounded than measured BMI). One-
Restored During Ustekinumab sample MR was conducted using individual-level
data (396,495 individuals) from the UK Biobank and
Longitudinal study of the psoriasis-associated skin the Nord-Trøndelag Health Study (HUNT), Norway.
microbiome during therapy with Two-sample MR was performed with summary-level
ustekinumab in a randomized Phase 3b clinical trial data (356,926 individuals) from published BMI and
psoriasis genome-wide association studies (GWASs).
M. Loesche, et al. The one-sample and two-sample MR estimates were
Departments of Dermatology and Microbiology, Pe- meta-analysed using a fixed-effect model. To test for
relman School of Medicine, University of Pennsylva- a potential reverse causal effect, MR analysis with
nia, Philadelphia, USA. genetic instruments comprising variants from recent
genome-wide analyses for psoriasis were used to
10 Dermatologica Helvetica - Volume 31(4) - Avril 2019NICHTS
SOLL IHRE
PSORIASIS
PATIENTEN
ZURÜCK
HALTEN1,2
Psoriasis beeinflusst viele Aspekte
des Lebens. 3-5 Die Belastung für die
Patienten nimmt im Laufe der Zeit zu.1,6
Grössere Symptomfreiheit bedeutet für
Betroffene eine stärkere Verbesserung der
Lebensqualität.7
Referenzen: 1. Feldman SR, et al. BMC Health Serv Res.
2017;8;17(1):337. 2. Feldman SR, et al. Am Health Drug
Benefits. 2016;9(9):504-13. 3. Leino M, et al. Eur J Dermatol.
2014;24(2):224-8. 4. Samponga F, et al. Acta Derm Venereol.
2012;92(3):299-303. 5. Griffiths CEM, et al. Br J Dermatol.
2018;179(1):173-81. 6. World Health Organisation.
Global report on psoriasis. 2016. Available at: http://apps.who.
int/iris/bitstream/handle/10665/204417/9789241565189 _eng.
pdf;jsessionid=EB265FC1DCDD109BF58CC19D80FB31D9?
sequence=1. [Accessed: October 2018]. 7. Strober B, et al.
J Am Acad Dermatol. 2016;75(1):77-82.e7.
AbbVie AG, Neuhofstrasse 23, 6341 Baar
CH-RISN-190006test whether genetic risk for this skin disease has a cological treatments reported conflicting results and
causal effect on BMI. Published observational data no RCTs of bariatric surgery were identified. Two co-
showed an association of higher BMI with psoriasis. hort studies suggested bariatric surgery, particularly
A mean difference in BMI of 1.26 kg/m2 (95% CI 1.02- gastric bypass, reduces the risk of developing psoria-
1.51) between psoriasis cases and controls was ob- sis (hazard ratio 0·52; 95%CI 0·33-0·81; pInhibition of the Interleukin-36 IL-36 & IL-37 & IL-38
Pathway: a Fascinating Proof Trio Targets of the Future
of Concept IL-36, IL-37, and IL-38 Cytokines in Skin and Joint In-
flammation: A Comprehensive Review of Their The-
Inhibition of the Interleukin-36 Pathway for the rapeutic Potential
Treatment of Generalized Pustular Psoriasis
M.-A. Boutet, A. Nerviani, C. Pitzalis
H. Bachelez, et al. Centre for Experimental Medicine & Rheumatology,
Sorbonne Cité Université Diderot, Paris, France Queen Mary University of London, UK;
We report the results of a phase 1 proof-ofconcept The interleukin (IL)-1 family of cytokines is com-
study involving seven patients who presented with posed of 11 members, including the most recently
a generalized pustular psoriasis flare and were discovered IL-36 IL-37, and IL-38. Similar to IL-1, IL-36
treated with a single, open-label, intravenous dose cytokines are initiators and amplifiers of inflamma-
of BI 655130, a monoclonal antibody against the tion, whereas both IL-37 and IL-38 display anti-in-
interleukin-36 receptor, 5 at 10 mg per kilogram flammatory activities. A few studies have outlined
of body weight Three patients had a homozygous the role played by these cytokines in several inflam-
IL36RN mutation, one of whom also had a heterozy- matory diseases. For instance, IL-36 agonists seem
gous mutation in CARD14 (which has been linked to to be relevant for the pathogenesis of skin psoriasis
pustular skin disease), and four did not have any of whereas, despite being expressed within the syno-
the target mutations (IL36RN, CARD14, and AP1S3). vial tissue, their silencing or overexpression do not
Among the study patients, the mean percent impro- critically influence the course of arthritis in mice. In
vement in the GPPASI score from baseline was 59.0% this review, we will focus on the state of the art of the
at week 1, 73.2% at week 2, and 79.8% at week 4. molecular features and biological roles of IL-36, IL-37,
Pustules were completely cleared in three patients and IL-38 in representative skin- and joint-related in-
within 48 hours after treatment, in five patients by flammatory diseases, namely psoriasis, rheumatoid
week 1, and in six patients by week 2. The efficacy of arthritis, and psoriatic arthritis. We will then offer an
BI 655130 regardless of the presence of the IL36RN overview of the therapeutic potential of targeting
mutation suggests that the interleukin-36 pathway the IL-36 axis in these diseases, either by blocking
may play a pathogenic role among patients with the proinflammatory agonists or enhancing the phy-
generalized pustular psoriasis who have different siologic inhibitory feedback on the inflammation
genetic backgrounds, including those without tar- mediated by the antagonists IL-37 and IL-38.
get mutations. This proof-of-concept study suggests
that the inhibition of interleukin-36 receptor with International Journal of Molecular Sciences, 2019,
a single dose of BI 655130 may reduce the severity 20, 1257. Doi:10.3390/ijms20061257.
of generalized pustular psoriasis over a 20-week pe-
riod, as was observed in our patients. However, fur-
ther clinical investigation is required to determine
the clinical efficacy, duration of effect.
The new england journal of medicine, 2019.
Doi: 10.1056/NEJMc1811317.
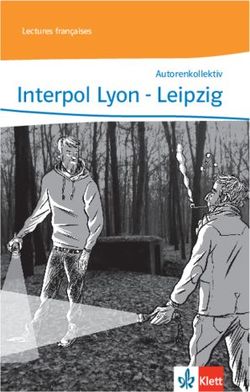
Figure 1. Overview of the IL-1, IL-36, IL-37, and IL-38 re-
ceptors and intracellular signaling. IL-1β binds the IL-1R1
receptor. Activated IL-1R1 recruits the IL-1RAcP com-
mon subunit and enables MyD88 to form a complex of
signalization with IRAK and TRAF, which leads in turn
to the phosphorylation/activation of the downstream
signaling. A counter-regulatory pathway is represented
by IL-1β binding its decoy receptor IL-1R2 (membrane-
bound or soluble) (not shown). IL-36α, β, and γ bind to
the IL-1Rrp2 and recruit the common subunit IL-1RAcP,
inducing similar downstream signaling cascades as IL-
1β. IL-37 binds IL-18Rα, which recruits IL-1R8 instead of
the usual IL-18Rβ, causing sequestration of Myd88 and
transduction of a weak signal because of the IL-1R8 mu-
Figure 1. Response to Treatment among the Seven Study Patients. tated intracellular domain. IL-38 might be able to bind
Panel A shows photographs of two patients with generalized pustular psoria- IL-1R1, IL-1Rrp2 and/or IL-1RAPL1 but further studies
sis, one of whom had the IL36RN mutation (upper row) and one of whom did need to confirm its preferential intracellular mechanism
not have the mutation (bottom row). The images were taken at baseline (before of action. IL1R = IL-1 Receptor; IL-1RAcp = IL-1 Receptor
treatment) and at week 1 and week 4 after treatment with a single intravenous Accessory Protein; IL-1RAPL1 = IL-1 Receptor Accessory
dose of BI 655130. Protein Like 1; IL-1Rrp2 (or IL-1RL2) = IL-1 Receptor Like
2; MyD88 = Myeloid Differentiation Primary Response
Fo c u s
Protein 88; IRAK = IL-1R-Associated Kinase; TRAF = TNF
Receptor-Associated Factor;JNK = Jun N-terminal Kinase;
AP1 = Activator Protein 1; NFκB = Nuclear Factor-kappa
B; MAPK =Mitogen-Activated Protein Kinases.
Dermatologica Helvetica - Volume 31(4) - Avril 2019 1314
Forschungspreis «Dermato-Onkologie 2019» Prix pour la recherche en dermato-oncologie 2019
Der Verein für Hautkrebsforschung www.skincancer.ch ist eine Vereinigung von Dermatologen Nous avons le plaisir de vous annoncer que l’Association pour la Recherche sur le Cancer
zur Erforschung und Behandlung von Hautkrebs. In Zusammenarbeit mit der Firma Pierre de la Peau (www.skincancer.ch) en collaboration avec les Laboratoires dermatologiques
Fabre 2012 hat er einen Forschungspreis für junge Wissenschaftler im Bereich Dermato- Pierre Fabre décerneront un prix de recherche destiné aux jeunes scientifiques dans le
Onkologie ins Leben gerufen hat, der jährlich vergeben wird. domaine de la dermato-oncologie.
Pierre Fabre, ein französisches Pharmaunternehmen, engagiert sich neben der Dermatologie Entreprise pharmaceutique française, les Laboratoires Pierre Fabre sont engagés depuis
und anderen Gebieten bereits sehr stark in der Krebsforschung. 2011 eröffnete eines der toujours dans les domaines de la dermatologie ainsi que dans la recherche sur le cancer à
grössten Krebsforschungszentren Europas seine Pforten, das Oncopole. Pierre Fabre war laquelle ils consacrent une attention toute particulière. En 2011, le plus grand centre de lutte
einer der Gründungsmitglieder dieses unabhängigen Forschungszentrums im Herzen von contre le cancer d’Europe, l’Oncopôle, ouvre ses portes. Pierre Fabre figure parmi les
Toulouse. principaux membres fondateurs de ce pôle de recherche en plein cœur de Toulouse.
Der 2001 gegründete Verein für Hautkrebsforschung unterstützt klinische und experimentelle L’Association pour la Recherche sur le Cancer de la Peau fondée en 2001 vient en soutien à
Forschung im Bereich der Dermatologischen Krebserkrankungen mit besonderer Förderung la recherche clinique et expérimentale dans le domaine de la recherche sur les maladies
der sogenannten translationalen Forschung. Daneben werden Projekte zur Früherkennung, cancéreuses, notamment dans la recherche dite translationnelle. En outre, elle encourage les
zur Vorsorge und Öffentlichkeitsarbeit gefördert. Die aktuellen Aktivitäten sind auf der projets s’articulant autour du dépistage précoce, de la prévention et des campagnes de
Webpage des Vereins www.skincancer.ch nachzulesen. sensibilisation. Plus d’informations sur les activités actuelles sont disponibles sur le site
internet de l’association: wwww.skincancer.ch.
Mit dem Pierre Fabre Skin Cancer Award soll die wissenschaftliche Aktivität in der Schweiz im
Bereich Hautkrebs gefördert werden. Der Preis richtet sich vor allem an Jungwissenschaftler Le Pierre Fabre Skin Cancer Award a pour but de promouvoir l’activité scientifique en Suisse
(jünger als 40 Jahre), die bereits in diesem Gebiet tätig sind. Er soll die laufenden Projekte dans ce domaine. Cette récompense s’adresse aux jeunes scientifiques (de moins de 40 ans)
auszeichnen und eine Basis schaffen, um neue Projekte voranzutreiben. Dieser Preis ist mit qui travaillent déjà autour de ce thème. Il vise à primer les projets en cours et à fournir une
10‘000 CHF dotiert. Bei gleichwertigen Projekten kann der Preis ausnahmsweise auch geteilt base pour la promotion de nouveaux projets. Ce prix est doté d’une récompense de 10‘000
werden. CHF. Pour les projets d’importance équivalente, le prix pourra exceptionnellement être
partagé.
Dem Vorstand des Vereins für Hautkrebsforschung ist es gelungen, ein internationales,
Le comité directeur de l’Association pour la Recherche sur le Cancer de la Peau est parvenu
renommiertes Expertenteam zu gewinnen, das die eingereichten Projektvorschläge objektiv
à réunir une équipe d’experts de renommée internationale pour l’évaluation objective des
und unabhängig bewertet. Das Komitee setzt sich zusammen aus Prof. Celeste Lebbe, propositions de projet soumises. Ce comité d’évaluation réunira notamment Dr. Celeste Lebbe
Hopital de St. Louis, Paris; Prof. Dr. Jürgen Becker, Universität Duisburg-Essen, Dept. de l’Hôpital de St. Louis à Paris; le Prof. Dr. Jürgen Becker, Université Duisburg-Essen, Dept.
«Translational Skin Cancer Research»; und Prof. Antonio Costanzo, Humanitas Research « Translational Skin Cancer Reserach »; et Prof. Dr. Antonio Costanzo, Humanitas Reserach
Hospital, Mailand. Hospital, Milane.
Die Einreichung der Projektbeschreibungen erfolgt bis zum 01.06.2019 an den Schweizer Les projets sont à adresser jusqu’au 01.06.2019 à l’adresse suivante: L’Association pour la
Verein für Hautkrebsforschung zuhanden von Prof. Reinhard Dummer, Klinikdirektor Stv., Recherche sur le Cancer de la Peau, Prof. Reinhard Dummer, Universitätsspital Zürich,
UniversitätsSpital Zürich, Dermatologische Klinik, Gloriastrasse 31, 8091 Zürich / Dermatologische Klinik, Gloriastrasse 31, 8091 Zürich / reinhard.dummer@usz.ch.
reinhard.dummer@usz.ch. Le projet retenu sera communiqué à l’Assemblé Annuelle de la SSDV 2019, 19-20 septembre
Der sechste Preisträger wird in Basel auf der SGDV-Jahresversammlung (Messe Basel), 19.- 2019, à Bâle (Messe Basel).
20. September 2019, bekannt gegeben. Les documents pour les candidatures devront être structurés de la manière qui suit:
Die Bewerbungsunterlagen müssen folgendermassen aufgebaut sein: 1. Titre
1. Titel 2. Description du projet en anglais (500 mots maximum)
3. Liste des publications antérieures sur le sujet (10 maximum)
2. Projektbeschreibung (maximal 500 Wörter in englischer Sprache)
4. Lieu de réalisation du travail de recherche suivi de l’autorisation du directeur de l’institut
3. Auflistung der bisherigen Publikationen in diesem Themenbereich (maximal 10)
en question.
4. Durchführungsort der Forschungsarbeit sowie Bestätigung durch den Leiter des
Dermatologica Helvetica - Volume 31(4) - Avril 2019
entsprechenden Institutes, dass die Arbeit hier durchgeführt werden kann.Vous pouvez aussi lire